 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
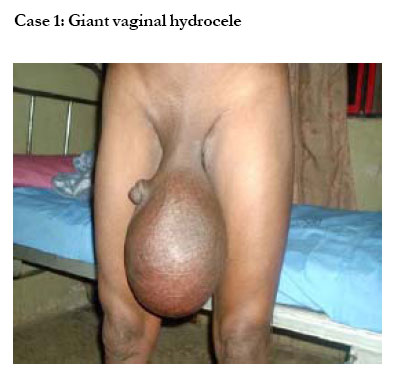
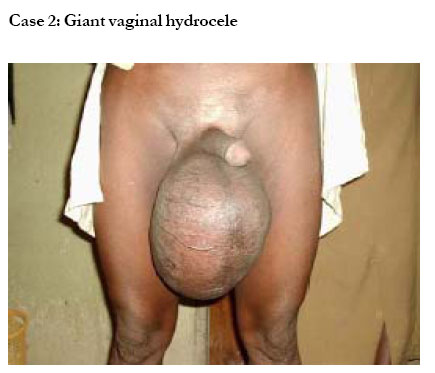
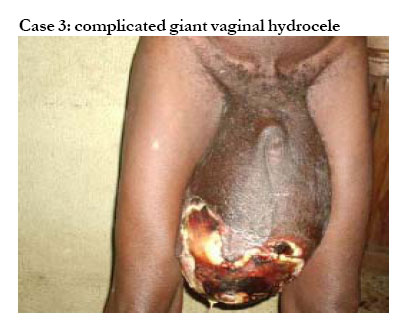
African Health Sciences, Vol. 5, No. 4, December 2005, pp. 343-344 Giant hydrocele - an epitome of neglect Emmanuel E. Akpo Head, Surgery Department, Dalhatu Araf Specialist Hospital, Lafia. Nasarawa State, Nigeria. Code Number: hs05062 Abstract Hydrocele [Greek: water - sac] is abnormal fluid collection within the tunica vaginalis of the scrotum or a patent tunica vaginalis. It is a relatively common condition in surgical practice. However, a giant hydrocele, here defined for clinical purposes, as a hydrocele equal to or bigger than the patient’s head, is rare as indicated by the limited number of reported cases in the literature. Keywords: Giant hydrocele, definition, quality of life Case 1 A 50-year-old man who presented with bilateral scrotal swellings for 10 years. No history of chronic cough, leg swelling or trauma to the scrotum. He is married with five children and has regular coitus. General examination revealed nothing significant. The abdomen was essentially normal with intact hernial orifices. The external genitalia revealed a near buried phallus and a bilateral cystic scrotal swelling up to knee level. The testis could not be felt. The cord contents felt normal. An assessment of giant vaginal hydrocele was made. The patient tested negative to microfilaria. Hydrocelectomy revealed 4litres of straw colored fluid with normal testes. Recovery was uneventful. (Case 1) Case 2 A 47-year-old man with 6-year history of painless bilateral scrotal swelling. He is married with five children. No history of trauma or cough. The swelling has been slowly progressive and no other swellings. Examination revealed a well-built man with intact inguinal hernial orifices. The phallus was normal. The scrotum showed a bilateral tense but cystic swelling up to knee level. Testes were not felt. He was negative to microfilaria test. Hydrocelectomy revealed normal testes and a 3.7litre straw colored fluid. Recovery was uneventful. (Case 2) Case 3 A 65-year old man with a 20-year history of bilateral progressive scrotal swelling and primary infertility. Three months prior to presentation he noticed a wound that became offensive with time. He was unable to walk without an assistant supporting the mass. No cough or prior trauma to the scrotum. His last coital contact was about four years prior to presentation. The external genitalia showed a buried phallus, a bilateral scrotal swelling up to knee level with part necrosis of the scrotal skin that was quite offensive. The abdomen showed prominent pyramidal muscles. The inguinal hernia orifices were intact. Wound swab yielded pseudomonas sensitive to ciprofloxacin. Microfilaria test was negative. Hydrocelectomy revealed 6.5litres of straw-coloured fluid with flattened testes. Seminal fluid analysis showed decreased sperm count. Recovery was uneventful. Discussion Case reports in the literature on ‘giant hydrocele’ are scanty. Giant hydrocele has been defined as a hydrocele having more than 1,000ml of contents1. Clinically, this is difficult to diagnose except by way of investigation such as ultrasound scan or surgery. This diagnosis becomes quite difficult in centers lacking such investigative armamentarium particularly in the African sub-region. Besides, a giant hydrocele in a child may not necessarily contain the same volume of fluid as that in an adult even though estimates of fluid contents may be done using a tape measure. There are reports on giant hydrocele1, giant abdominoscrotal hydrocele2 and large abdominoscrotal hydroceles3 but none, to the best of my knowledge, has concretely defined a giant hydrocele or reported on its effect on the quality of the patient’s life following acquisition of the disease. This is probably because of rarity of this condition. For clinical purposes and comparison sake therefore, I have defined a giant hydrocele as that equal to or bigger than the patient’s head. Giant hydroceles are primarily due to neglect on the part of the patient, poverty, fear of impotence/sterility and/or death from the operation4. Giant hydoceles may reduce the patient’s work capacity, impair sexual function and have a negative effect on the quality of the patient’s life, his family and the community by becoming socially embarrasing4, 5, 6. This may be as a result of the weight of the enlarged scrotal sac causing discomfort and impairing the patient’s mobility while the pull on the scrotal skin as well as the pressure on the penile urethra may result in venous engorgement with occasional difficulty in micturition1. Giant hydroceles may also affect the quality of patients’ life by posing psychosocial problemsand men with giant hydroceles tend to have more severe psychosocial problems than physical ones7.In assessing the quality of life of patients with hydrocele, Gyapong et. al. reported that men with small hydroceles sought healthcare services more than those with giant ones and the ridicule from community members was a major problem in patients with giant hydroceles8. In the Gyapong et. al. series, unmarried men with giant hydroceles in particular found it difficult to find a spouse with their condition, and various degrees of sexual dysfunction were reported amongst married men8. The low quality of life inflicted on the sufferer forms a major problem in terms of socioeconomic burden as reported by Ahorlu C.K. et. al. were patients with giant hydroceles expressed the view that the presence of the giant hydrocele severely reduced their work capacity and impaired their sexual function, and that overall it had a considerable negative effect on the quality of their lives, their families and the community4. The condition affected their work output and subjected them to hardships such as teasing, unsuitability for marriage, sexual dysfunction and divorce9. Ramu K. et. al. reported that giant hydrocele has an average of 27.4% reduction on the productivity and wage-earning capacity of patients10. Complications that may arise following this condition include pressure necrosis with wound infection which can be quit offensive and demoralizing to the patient (Case 3), septicemia, hematocele, calcification of the sac, calculus formation and infertility5, 11. Coitus may be impaired, not only as a result of the dragging effect on the phallus by the size of the mass (Cases 1 and 3) but also from the psychosocial stigma8. Little attention has been paid to this important, but hidden, disability (sexual disability) associated with this disease12. In one study, hydrocele accounted for 10.43% cases of male infertility13. This is attributed to partial or total arrest of spermatogenesis with resultant subfertility or infertility probably due to pressure on the testes with progressive testicular flattening or atrophy5, 14. This might explain the cause of infertility in case 3. Following hydrocelectomy, all three cases agreed to improved sexual function six weeks after surgery and could attend social functions and farm work more effectively. The dejection faced by case 3, in particular, among his family members was also obviated following the surgery. It is important therefore, that health education be intensified to address the issues of sexual disability and quality of life in patients with giant hydroceles. References
Copyright 2005 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs05062f2.jpg] [hs05062f1.jpg] [hs05062f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}