 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
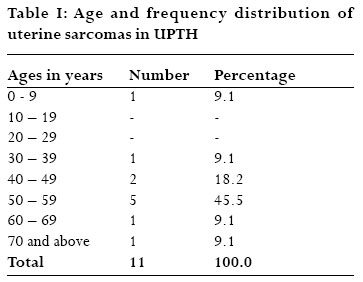
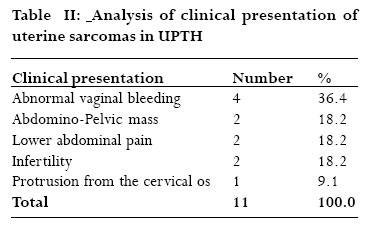
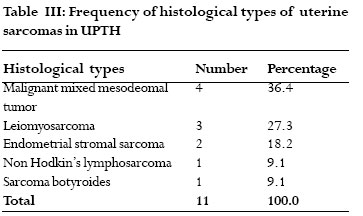
African Health Sciences, Vol. 7, No. 1, March, 2007, pp. 10-13 Uterine sarcomas in Port Harcourt, Nigeria A 12-year clinico-pathologic study *Seleye-Fubara, D, Uzoigwe, S. A. *Department of Anatomical Pathology,University of Port Harcourt Teaching Hospital, PMB 6173, Port Harcourt, Nigeria. Department of Obstetrics and Gynecology, University of Port Harcourt Teaching Hospital, PMB 6173, Port Harcourt, Nigeria. Correspondence: *D. Seleye-Fubara Department of Anatomical Pathology, University of Port Harcourt Teaching Hospital PMB 6173, Port Harcourt, Nigeria E-mail: dsfubara@yahoo.com Code Number: hs07003 Abstract Background: Uterine sarcomas are rare gyneacologic malignancies with a high mortality.There is the need to determine its frequency, clinical presentation and histologic variants.This may form the basis for further research and management inorder to reduce the morbidity and mortality associated with it. Key words: Uterine Sarcoma,Age, Presentation, Port Harcourt. Introduction Uterine sarcomas are not true soft tissue sarcomas because it does not fall into the definition of soft tissue sarcomas.1,2 The etiology is unknown but associated with Epstein-Barr virus in immunodeficiency state and/or following therapeutic immunosuppression in transplant setting.1 It is also associated with pelvic irradiation for other uterine tumors and genetic predisposition (familial cancer syndrome)2. Mutation of P53 tumor suppressor gene are critical to sarcoma genesis in patients with Li-fraumeni syndrome.1,2 Uterine sarcomas are locally aggressive tumors that are capable of invasion, recurrence and distant metastasis. They are rare primary tumors of the uterine messenchymal tissue3. The various sarcomas of the uterus occur when the malignant cells differentiate along smooth muscle or occasionally, transformation of benign smooth muscle tumor4,5. Differentiation along the uterine mesoderm affects both epithelial and messenchymal structures6,7 while in other cases, differentiation along the supportive tissue of the endometrium and in very rare occasions, along lymphoid tissues and smooth muscles to give lymphomas (lymphosarcomas) and rhabdomyosarcomas.8-11 Different age groups are affected; of which some are age and AIDS defining.2,11,12 Different clinical presentations ranging from abnormal vaginal bleeding, lower abdominal pains, lower abdominal mass, and infertility to cervical os protrusion are common. This study is the first of its kind in this setting. It aims at analyzing the histo-pathologic patterns of the uterine sarcomas with respect to the patient’s age, clinical presentation, which may serve as a baseline for further research. Materials and methods The University of Port Harcourt Teaching Hospital is a 600 bed hospital, rendering tertiary health care services to Rivers, Bayelsa, parts of Delta, Abia, Imo and Akwa Ibom States of Nigeria. The hospital records for histopathology consultation of all patients in whom a diagnosis of uterine sarcomas has been made were reviewed covering January 1st 1990 to December 31st 2001 for the study. The variables considered include: age of patients, clinical presentation of the patients and the histologic types. This information were retrieved from the patient’s case notes, histologic request forms and reports. Thirteen cases were diagnosed; of which only eleven had adequate records for the study.Two tissue had inadequate records and were excluded from the study. The data collated were analyzed and tabulated in multiway frequency tables. Results A total of 2,105 malignant tumors were histologically diagnosed at the University of Port Harcourt Teaching Hospital (UPTH) during the study period (1990 – 2001) of which thirteen cases were uterine sarcomas. This accounted for 0.5% of the total malignancies and 4% of gynaecologic malignancies.The youngest was 3 years old and the eldest was 72 years old. Table I shows the age and frequency distribution of uterine sarcomas seen in UPTH. The highest frequency (45.5%) occurred in the age group 50-59 years and the least was recorded in the age groups 0-9, 30-39, 60-69 and 70 years and above (9.1% each). Table II shows the frequency analysis and the clinical presentation of uterine sarcoma in UPTH. Majority of the tumors (36.4%) presented with abnormal vaginal bleeding.This is followed in decreasing order of frequency by palpable abdomino-pelvic mass, lower abdominal pain and infertility (primary/secondary); each accounting for 18.2%.There was only one case of tumor protruding from the cervical os (9.1%). Table III shows the frequency analysis of the various histologic types of uterine sarcomas diagnosed in UPTH during the period under review. Majority (36.4%) was malignant mixed mesodemal tumor which was followed in decreasing order of frequency by leiomyosarcoma (27.3%), endometrial stromal sarcoma (18.2%) and non Hodgkin’s lymphosarcoma and sarcoma botryoides 9.1% each. Discussion Sarcomas of the uterus are rare messencymal tumors worldwide; accounting for only 1 – 3% of female genital tract malignancies, yet they are the most aggressive of all the malignancies of the female genital system13 - 15. This observation is confirmed by our study as uterine sarcomas accounted for 0.5% and 4% of the total malignancies and gynaecological malignancies in this setting.The figures recorded in this centre corroborates the reports of other workers in this specialty5,10,16-19 irrespective of the small sample size. The rate of soft tissue sarcomas are few because, in addition to its rarity worldwide, only those diagnosed in this hospital were used for the study. The number would have increased if data from other peripheral hospitals and private histology laboratories were to be included.There is age variation in occurrence of these tumors hence some of them like the sarcoma botryoides are known to be age defining, since they occur mainly below the age of five years11,20 corroborating our case though, the uterous is not a soft tissue by definition. Most of the tumors (45.5%) occur in the age group 50 – 59 years which co-relate well with the age distribution in other studies elsewhere21,22.This study also recorded majority (81.8%) of these cancers in the ages 40 years and above; meaning, uterine sarcoma is mainly a disease of old age. Our patients generally present with variable symptoms. Foremost (36.4%) was abnormal vaginal bleeding. Abdomino-pelvic mass, lower abdominal pain also brought some of these patients to hospital.This is an important symptom in patients with uterine sarcoma and physicians should not be complacent about it. Uterine sarcomas were diagnosed from biopsies taken from patients that presented with infertility because they also presented with abnormal vaginal bleeding. Few malignancies constituted the sarcomas of the uterus in this communication. Malignant mixed mesodermal tumor (MMMT) is the most common uterine messenchymal malignancy in this report and it occurred in post menopausal women corroborating other studies where the patients presented at the age of 50 years and above13,21,22.This tumor is highly aggressive as three of our cases presented with extensive myometrial invasion; of which one has pelvic involvement. The remaining one showed polypoid mass expanding in the uterine cavity on sectioning, in addition to hemorrhage and necrosis. Microscopy of the four cases were similar, showing biphasic infiltration of the atrophic uterus by malignant epithelial and messenchymal tumors. The epithelial component appears endometroid in three and squamous in one. In the single squamous epithelial proliferation, the stromal cells also showed individual cell keratinization hence making the tumor a homologus type while in the other three, the stromal malignancy showed chondroid cells giving the biphasic pattern or heterogenous type of malignant mixed mesodermal tumors (carcino-sarcoma). In America, a good majority of patients with MMMT had a past history of radiotherapy for other earlier pelvic neoplasia24,25 but this history was not stated by any of our patients. Leiomyosarcoma is known to be the most common uterine sarcoma arising from the smooth muscle walls of the uterus26 but this is at variance with our report. It is second only to MMMT in this study and the reason for this variation is unclear. The idea that, leiomyosarcoma emerge from a pre-existing myoma is difficult to predict yet various figures ranging from 1 - 8 per thousand have been reported13. This tumor is reported to be more common in blacks than whites23 but this is not confirmed by our study since no white patient was seen. The onset of this disease in our patient was in the 4th decade of life which agrees with various reports in Nigeria2 and elsewhere13,27 though the study was on soft tissues.This cancer accounted for 27.3% of uterine sarcomas, a figure similar to the 25% recorded in USA10. The slight disparity may be attributed to the sample size. Patients with this tumor in our experience mainly presented clinically with abnormal vaginal bleeding as against palpable abdomino-pelvic mass in another study26. Grossly, the tumor is large and soft, yellow or tan in color with poorly circumscribed margin. Microscopy show swirling masses of spindle-shaped smooth muscle cells containing myofibrils, large hyperchromatic nuclei with irregularly clumped chromatins. There were few large pleomorphic or anaplastic tumor cells with twelve to fifteen mitoses per high power field. One of these contained numerous giant cells. Endometrial stromal sarcoma occurs in the perimenopausal age group with an average age of 45 years9. This age is corroborated by the ages of our patients which ranged from 43 to 52 years. This tumor therefore occurs in younger patients than those of the MMMT. The diagnosis of this tumor is usually by endometrial curettings or hysterectomy for histopathologic evaluation; if the lesion is intramural.The uterine curetting is indicated because they present with abnormal vaginal bleeding. Grossly, the uterus is enlarged, irregularly contoured with bulky polypoid tumor bulging into, and filling the endometrial cavity. Microscopy shows proliferation of the endometrial stromal cells with inconspicuous nuclei. The cytoplasm is amphophilic with ill defined cell boarder. There are numerous mitoses ranging from 10 – 12 per high power field. Non-Hodgkin’s Lymphosarcoma (Lymphoma) of the uterus is very rare in the literature and in this environment.To the best of our knowledge and search, this is the first reported case in this hospital. The uterus is not the usual site for this tumor since it is not a lymphoid organ. It was diagnosed in a 30 year old HIV positive patient. Though the occurrence of lymphosarcoma of the uterus have been reported by another author,28 there was no reference to HIV positivity. It is therefore important to research further into the relationship between non- Hodgkin’s lymphosarcoma of rare anatomic sites and HIV sero-positivity. It may be one of the AIDS defining tumors. Grossly, the uterus is bulky and fleshy with areas of hemorrhage and necrosis. Microscopy shows uterine tissue with infiltration of malignant lymphoid cells which are punctuated in areas by fibrillary tissues, and numerous atypical chronic inflammatory cells. Sarcoma botryoides of the uterus is another tumor of unusual site since the uterine muscle is not a skeletal muscle.This lesion was diagnosed in a 3 year old girl; corroborating a text book account of the tumor affecting the cervix and vagina in young children; usually in their first decade of life23,27. Grossly, the tumor showed aggregates of grapelike growth. Microscopy showed infiltrating columns of immature small spindle shaped myocytes with tapering bipolar cytoplasmic extensions. The tumor cells are in a loose myxoid stroma, and rimmed by a fibrillary cambium layer. There are numerous abnormal mitotic figures. Finally, uterine sarcoma are rare malignant tumors in this environment and worldwide. It should be suspected if a previously diagnosed myoma or other benign tumor of the uterus grows rapidly in a post menopausal woman.The fifth decade of life is a risk factor and though these tumors are rare, the morbidity and mortality rate associated with them are very high. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07003t1.jpg] [hs07003t3.jpg] [hs07003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}