 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
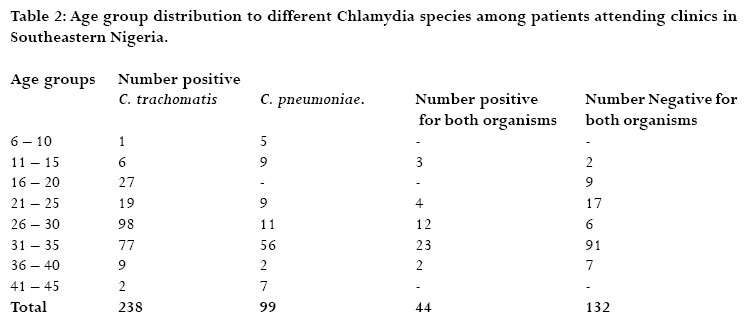
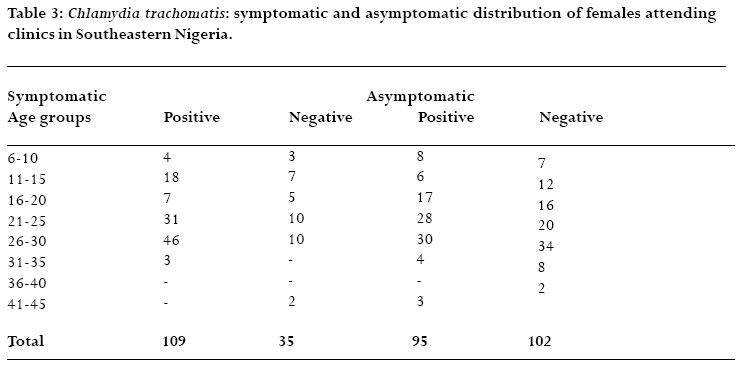
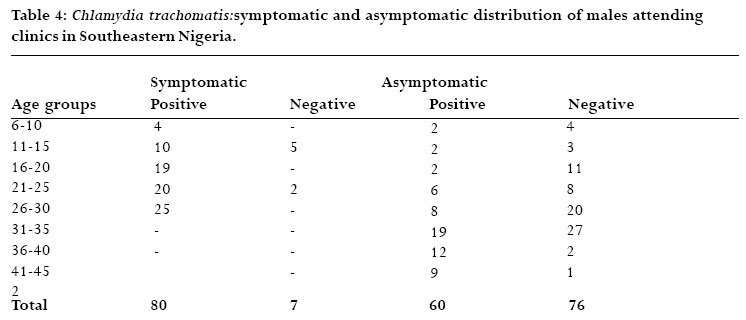
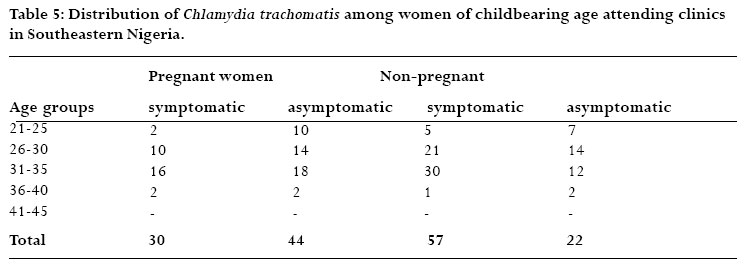
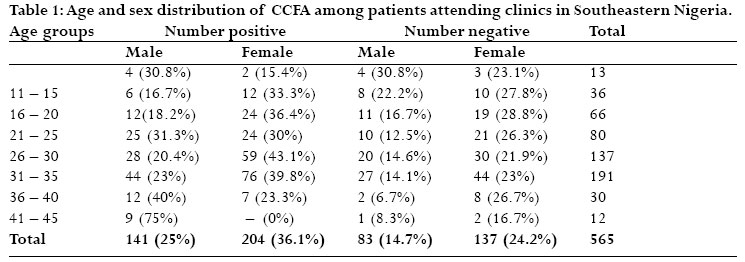
African Health Sciences, Vol. 7, No. 1, March, 2007, pp. 18-24 Prevalence of chlamydia in patients attending gynecological clinics in south eastern Nigeria *Okoror L E., Agbonlahor DE, Esumeh F I, Umolu P I Department of Microbiology, Faculty of Natural Sciences, Ambrose Alli University. PMB 14, Ekpoma. Nigeria. *Correspondence: Okoror L E Department of Microbiology Faculty of Natural Sciences Ambrose Alli University. PMB 14, Ekpoma. Nigeria. Email: Larison86@Yahoo.Com Code Number: hs07005 Abstract Background: Chlamydia infections have been reported to cause silent infections in communities which becomes endemic and could remain unnoticed for a very long time. In most parts of Nigeria these organisms are not screened for, and hence relative information about frequencies of the organisms are sparse. Key words: Chlamydia, Complement fixation test, Chlamydia Complement Fixing Antibody Introduction The Chlamydiae are obligate intracellular parasites of eucaryotic cells1 found in the leucocytes and consist of minute particles. Chlamydiae are non-motle, coccoid, ranging from 0.2 to 1.5um. Chlamydiae are exquisitely adapted for extra cellular survival and intracellular growth. They prevent their phagosomes from fusing with lysosomes, and they inhibit host synthesis of protein and DNA. They make all their own macromolecules, but parasitize their host for metabolic energy, they do not oxidize pyruvate by way of tricarboxylic acid cycle and do not appear to generate (ATP) 1 Taxonomically, they are in the order chlamydiales, which have one family Chlamydiaceae and one genus Chlamydia. They contain formally three main species, which includes Chlamydia trachomatis, Chlamydia psittaci, Chlamydia pneumoniae (formally called TWAR)3 and a new Chlamydia pecorium isolated from stomach of ruminants2. Chlamydia pneumoniae has been recognized as an important acute respiratory pathogen in man4. Chlamydia trachomatis is composed of two biovars; the lymphogranuloma venereum agents and the ocular genital serotype, which may be distinguished by welldescribed seroprevalent with distinctive antigens in their outer membrane proteins. Chlamydia psittaci is a diverse species that has poorly been characterized, strains that infect psittacine birds seem to differ from those that infect poultry; several mammals and marsupials have species-specific strains4. Chlamydiae were once thought to be viruses and were referred to as large viruses because of their smallness and their inability to multiply outside the susceptible host and they are filterable7. They look like bacteria by having cell wall which lack muramunic acid, they contain both DNA and RNA, they divide by binary fusion and are susceptible to a range of antibiotics4. They are now thought to be a special kind of bacteria. Chlamydiae have two morphologically and functionally distinct developmental cycle, the infectious elementary body (EB) and the reproductive reticulate body (RB)5,6. They multiply in the host cell cytoplasmic vacuole. A Chlamydia filled vacuole is large enough to be seen by light microscope. When properly stained the cell stain differently while the Chlamydia inclusion stain differently. Chlamydia inclusion stain with giemsa while Chlamydia trachomatis stain with iodine because its cell wall and matrix is rich in glycoprotien7. Both large and small parasites are seen outside the cell lying close to cell debris. All Chlamydia have a group reactive antigen detectable in the supernatant of lysates (or heat suspension).The antigen is heat stable lipopolysaccharides with 2-keto-3 deoxycholic acid as an immodorminant component.This antigen can be detected by complement fixation test8. This justifies the use of species specific monoclonal antibody to screen for different species so as not to have false positive results as complement fixation test will only detect the group reactive antigen. It also justifies a confirmation by culture methods. Chlamydia trachomatis causes about 40% to approximately 50% non gonococcal urethritis in men, Chlamydia trachomatis causes epididymitis, mucopurulent cervicitis, proctitis, urethritis, endometritis, salpingitis, endemic trachoma, inclusion conjunctivitis, newborn pneumonia, perihepatitis (Fitz-High-Curtis syndrome) and later post partum endometritis. This accounts for why women with suspected case of pelvic inflammatory diseases and cervical pains were included in the study. It can also cause post gonococcal urethritis. Chlamydia trachomatis can cause pelvic inflammatory diseases resulting in infertility and ectopic pregnancy9. Hence the screening of women with infertility cases, though they were asymptomatic. It has been found from studies reported in Italy, Sweden and USA that about 60% of 70% of Chlamydia trachomatis positive cases are asymptomatic10,11. It was also reported that the risk is higher for women under 25 years of age who have sex before the age of 1810. Okoror, et. al.18 reported a 51% prevalence among pregnant and non pregnant women and their spouses pre and antenatal clinic in the College of Medicine of the University of Lagos, Lagos Nigeria18. Chlamydia trachomatis could cause pharyngitis in children and newborn acquire the infection during passage through an infected birth canal13. Chlamydia trachomatis similar serotype has been isolated from the eye of a baby; the vagina of the mother and urethra of the father and the prevalence varies with maternal age13. Hence the inclusion of pregnant women, their spouses and the newborns and infants in this study. Chlamydia psittaci, a common pathogen of avian and lower mammalian species is relatively uncommon is humans, causes psittacosis in birds but could be transmitted to those keeping psittacine birds and those handling and slaughtering poultry14. Chlamydia pneumoniae formally known as TWAR was first obtained in 1969’s in chick embryo yolk sac culture16. Chlamydia has been recognized as an important acute respiratory pathogen in man5. It causes upper and lower respiratory tract infection which includes pharyngitis, sinusitis, bronchitis and otittis media16. Information about the relative frequencies in developing countries is sparse18. Hence this study, which is aimed at establishing the prevalence of the pathogens in southeastern Nigeria where reports on Chlamydia is relatively few. Complement fixation test though cumbersome, still remains one of the most reliable serotypical tests and it becomes diagnostic especially when the paired serum sample is taken.Though antibody titre higher than 1:160 is also regarded as diagnostic. However, confirmation could be done using other methods like the culture method whose specificity and sensitivity have been reported to be very high20 but requires a great degree of expertise to interpret. This again justifies the use of culture method ass confirmatory in this study. This study also aims at establishing the prevalence of Chlamydia trachomatis infection among women visiting gynaecological clinics, since little reports exists regards the relations between Chlamydia trachomatis and and infertility cases generally in this part of the world. This study will help clinician in proper administration of treatment in such cases as studied, and also help government to decide on whether to embark on community screening of Chlamydia, which so far one may refer to as a “silent epidemic”. However, there have been reports on the increase of infertility cases in this part of the world and Chlamydia trachomatis may just be implicated as have been reported in other parts of the world. Materials and methods Study design The study was carried out mainly on patients visiting the gynaecological clinics, which will include those for prenatal diagnosis which may be symptomatic or asymptomatic and also those in the antenatal clinics in order to know the risk of contacting of contacting Chlamydia trachomatis infection by the unborn fetus during birth.That is why this study also screened infants and any infant whose either parent was screened and available for screening automatically qualified for inclusion in the study. Those for prenatal counseling include mainly women for infertility cases who were mainly asymptomatic. Most of their spouse who visited the clinics was also included in the study. The objective of this study was to screen for Chlamydia trachomatis but we went ahead to confirm for Chlamydia pneumoniae since the genus Chlamydia have a group reactive antigen which is detected by complement fixation test a method we used in this study, so in order not to report false positive result, we have to distinguish the two human species, both by culture methods and the monoclonal antibody method. By this we underscore the use of PCR, which is not readily available in this part of the world. Sample collection: Five hundred and sixty five (565) blood samples were collected from pregnant and nonpregnant women including their spouses, infants and newborns attending gynecological clinics in various hospitals in the Southeastern part of Nigeria.Ten umbilical cord fluids were also collected.The blood samples were aseptically collected into sterile vacutannier, centrifuged (Hetituch) at 3,000rpm and serum collected into vials and stored at –20oC until used. Some of the non-pregnant women were asymptomatic women visiting the clinic with their spouses on infertility cases while some had cases of pelvic inflammatory disease or cervical pains. Procedure: Complement fixation test was carried out as described by Krivoshein19. The antigen used was obtained by inoculating embryonic egg with materials obtained from Chlamydia trachomatis positive patients and later titerated to the required concentration.The sheep red blood cell used was obtained by bleeding the jugular vein of a sheep aseptically. The blood was washed and stored until used in a 4oC refrigerator as described by Krivoshein19. The complement and haemolysin used to sensitize the sheep red blood cells were obtained commercially (Wellcome, Middlesex, U.K). Patients whose samples were positive to complement fixation test had their endocervical swab for females and Urethral discharge or scrapings for males collected with sterile swab stick with the help of clinicians.Those patients with respiratory diseases had their throat washings, sputum or nasal swab collected for Chlamydia pneumoniae analysis. The swabs were emulsified with sterile phosphate buffered saline and then inoculated into the yolk sac of embryonic eggs as described by Krivoshein19 and Romanowsky-Giemsa staining technique was then carried out on smears prepared from materials obtained from the harvested yolk sac of embryonic eggs. Observing for species-specific inclusion bodies under the oil immersion objective did identification of specific species. To further confirm the positive samples, the Chlamydia monoclonal antibody spot test kit was used to test for both Chlamydia pneumoniae and Chlamydia trachomatis in sera collected and test was carried out as described by the manufacturer (Immunocomb). Since not all spouses visited the clinic, the student test of the SPSS statistical package version 11 was used to access any significant difference between the number of males and females that visited the clinics. Result Of the five hundred and seventy five (565) blood samples screened for CCFA only three hundred and forty five (345) samples were positive. From the positive samples were two hundred and four (204) females and one hundred and forty one (141) males.Ten umbilical cord fluids collected from some of the women who attended prenatal clinic in some of the clinics were negative, even as the women were positive to CCFA.Age group distribution shows that 31-35 years of age had the highest number of samples testing positive to CCFA, which was closely followed by age group 26-30 years of age.Age group 41-45 had the lowest number of samples testing positive CCFA (table 1). The culture and the spot test result shows that more of the patients were positive for Chlamydia trachomatis with two hundred and thirty eight (238) samples while only ninety- nine (99) were positive for Chlamydia pneumoniae. However, forty-four (44) samples were positive for both Chlamydia pneumoniae and Chlamydia trachomatis while one hundred and thirty two (132) samples were negative for both Chlamydia trachomatis and Chlamydia pneumoniae. (Table 2). The sample mean for the positive female samples was 25.5 with a standard deviation of 27.78 while for males 17.5 and 13.71 mean and standard deviation respectively. The paired t test at 95% confidence limit was 1.425. The paired sample correlation was 0.929 with Table 3 shows that 109 positive females to Chlamydia complement fixing antibody were symptomatic while 95 had no clear cut symptoms. From the asymptomatic samples were 102 negative females for Chlamydia though 35 negative females had symptoms of Chlamydia infections (Table 3). While 80 positive males were symptomatic, 60 were asymptomatic and 7 and 76 were negative for symptomatic and asymptomatic respectively (Table 4).Thirty pregnant women ere symptomatic while 44 were asymptomatic, of the 79 non-pregnant 57 were symptomatic while 22 were asymptomatic (Table 5). Discussion Chlamydia spp. has long being known to cause mild to chronic infection in humans. It has previously been reported that relative frequencies developing countries are scanty19 and infection could be higher in developing countries. Hence the high positive result recorded in this part of Nigeria is likely to be the first kind of study.This result may not be unconnected with the fact that Chlamydia infections are usually latent with no clear-cut symptoms and hence are not usually treated. As diagnosis for Chlamydia infections are not usually carried out, hence most infection caused by Chlamydia is usually taken for other infections.Also since Chlamydia are usually found of latent infection, the infection pass unnoticed and remain endemic in the population for a long time. Sex distribution (table1) shows that more females were positive to CCFA than males, which may not be unconnected to the fact that more females visited the hospitals than males. More of the females also presented themselves for screening since most of them were in house prenatal patients, which makes sample collection easier, but most spouses refused samples collection, and this also accounts for reasons why more females were positive to CCFA than males. However, it could be that more females habour this infection than males because of the nature of their urinogenital organ since most of them were actually more positive to Chlamydia trachomatis than their male counterparts who were more positive to Chlamydia pneumoniae. A comparison of the result obtained in the CCFA (Table 1) and the culture result (Table 2) shows that there was differences in both results and this may be as a result of the fact that Chlamydia posses a group reactive antigen which could be detected by Complement Fixation Test (CFT). However, the culture results were more specific to each species since there cultural differences were observed. Negative results also obtained in table 2 could be accounted for, since CFT results depends on the time of infection, some infections could be acute, such infections could still be having active multiplying organisms in the patients which could pass undetected by CFT but is detected by the culture method. Also CFT may detect antibody in convalescing patients which may no longer be shedding the organisms but remains positive to CFT unless paired serum sample is collected and a four fold rise in titer is observed. Age group 31-35 years of age had the highest positive result to CCFA due to the fact that most of the women and spouses screened were those attending pre natal diagnosis in various clinics and this age group happens to be the child bearing age in this part of the world.They may have also acquire the infection during their adolescent ages which also accounts for the reason why age group 26-30 years of age have the highest positive samples to Chlamydia trachomatis since it is also an adolescent age with most of the males and females in the age group unmarried.This further support previous reports that Chlamydia trachomatis is a disease of the adolescent17. Age group 6-10 and 11-15 years who were positive to CCFA may have acquired the antibody through the maternal source since the antibody acquired from the mother could persist to certain age in life. Some could also have acquired the infection during from their during delivery15 or from their mothers through unhygienic processes. However, this is further differentiated in table 2 as most of the patients in this age group were positive to Chlamydia pneumoniae, which also suggest that they could have acquired the infection after birth since most of the infants attend nursery homes where children are rounded together confirming an earlier report by Schachter and Dawson11. Older men (41-45 years) had more number of positive patients to Chlamydia pneumoniae which may have resulted due to old age and other factors available due since aging could have brought down their immunity. Chlamydia pneumoniae infection is actually a disease of extreme life as well as that of immune compromised as various studies have previously implicated the organism in such patients9. More of those older men having Chlamydia pneumoniae would have due to the fact that men mixes up with each other than their female counterparts since men have to go out always to fend for the family and are thereby exposed to more risk than their female counterparts. Statistical analysis however, shows that there was no significant difference between the number of males and females who visited the clinic which further justify their comparison even not all the spouses visited the clinics.A high number of women were asymptomatic (197) (table 3) which infer that Chlamydia trachomatis is endemic or significant in the population as confirmed by statistical analysis using the chi square at 95% confidence limit. This infection therefore may be responsible for all the abnormalities faced by the women who visited the clinics like in the case of pelvic inflammatory disease and/or cervical pains and infertility. It could however pose a great danger to the unborn fetus as a significant number of pregnant women are said to be carrying the infection (table 5). It is even worse when a large number of married men harbour the infection which in most cases are asymptomatic (table 4), the risk of re-infection to both pregnant and non-pregnant women cannot be ruled out as most of the men sampled in this study ae spouses of the women that visited the clinics and they reported in significant numbers. Hence Chlamydia trachomatis is no longer an infectrion of the adolescents alone as was previously assumed. It has become a disease of all who have started having sex as men become more promiscus. Chances of re-infection could be seen in the high number of pregnant women who harbour the infection (table 5). Hence this study recommends proper diagnosis of infection so as to stem the spread of this infection, which is now going unchecked. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07005t3.jpg] [hs07005t2.jpg] [hs07005t5.jpg] [hs07005t4.jpg] [hs07005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}