 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
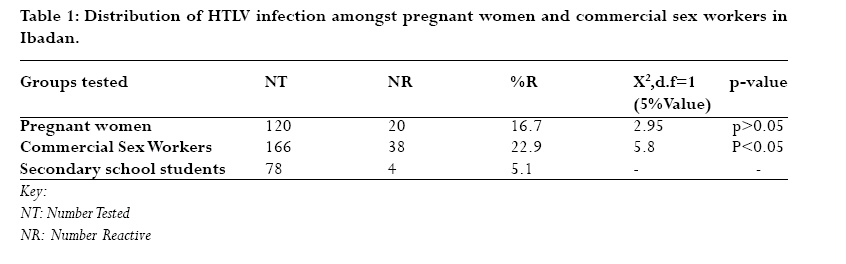
African Health Sciences, Vol. 7, No. 3, June, 2007, pp. 129-132 Human T-cell lymphotropic virus in a population of pregnant women and commercial sex workers in South Western Nigeria J.C. Forbi1*, A.B. Odetunde2 *1Virology laboratory, Innovative Biotech-Keffi, PO Box 30 Keffi, Nasarawa State,Nigeria 2Institute of Advanced Medical Research and Training, University of Ibadan,Nigeria *Address for correspondence: Forbi JC, Virology laboratory, Innovative Biotech-Keffi, PO Box 30 Keffi, 1. Abdu Abubakar Street, GRA-Keffi, Nasarawa State, Nigeria. cforbi79@hotmail.com Code Number: hs07026 Abstract Background: Over 20 million persons are infected with HTLV-I/II globally.The virus is endemic in Africa and it is also transmitted sexually. Continued identification of high risk groups is important for the control of the disease. Keywords: HTLV, prevalence, pregnant women, commercial sex workers, Nigeria. Introduction Human T-cell lymphotropic virus types I and II (HTLV I/II) are closely related yet distinct human retroviruses that share approximately 60% of their overall nucleotide sequence1. HTLV-I has been shown to be associated with at least two well-defined clinical entities, namely Adult T-cell leukemia/lymphoma (ATLL) and HTLV-I associated myelopathy/tropical spastic paraparesis (HAM/TSP)2,3,4. HTLV-II was initially isolated from a patient with hairy cell leukemia but its pathogenicity is not clearly understood5. .Recently, HTLV-II has also been shown to be linked with other neurological syndromes 6. Over 20 million persons are infected with HTLV-I/II globally7. Most are described in highly endemic areas such as Japan, intertropical Africa, the Caribbean’s and surrounding regions. On the contrary, low HTLV seroprevalence rates are observed in nontropical areas8,9. Several studies have reported high prevalence of HTLV infections in Africa10,11,13. It is therefore necessary to find out which group of individuals are reservoirs of the virus in the population. In Nigeria, routine diagnosis of HTLV infection is rare. This is worsened by the fact that government focuses on HIV (another retrovirus) that is presently establishing itself in Nigeria. To date, no vaccine or drugs have been licensed for use against HTLV infection. HTLV-I/II infections can be transmitted by vertical route (mother –to-child and breast milk), sexual intercourse and parenteral (blood transfusion and intravenous drug use)13. In Nigeria, transmission of HTLV infection to transfused recipients and in patients with leukaemia/lymphoma are well documented14,15,16,17,18,19,20. Olaleye et. al.,21 had shown that vertical transmission of HTLV infection may not be the major route of transmission of HTLV infection in South Western Nigeria. On the other hand, information on sexual transmission of HTLV infection is scanty in Nigeria and we think that this might well be a very important mode of transmission in Nigeria. Recently, a Nigerian-born CSW with ATL exported HTLV infection to Italy19. Identifying high risk groups remains one of the greatest opportunity to reduce the spread of the virus. This study was therefore designed to determine the prevalence of HTLV infection amongst two highly sexually active groups, pregnant women and CSWs in South Western Nigeria. Subjects and Methods Study area and population This study was carried out among pregnant women attending the antenatal clinic of the Oyo state hospital, Oyo and CSWs from brothels in Ibadan metropolis. Only females were eligible to participate in the study. After explaining the purpose and importance of the study to the clients, blood samples were collected by venepuncture from individuals who agreed to be bled. Blood samples were also collected from sex-matched control group consisting of students from a secondary school in Ibadan.These students were chosen as a control group since it is believed that this group of people are not as sexually active, hypothetically conferring on them a lower risk of acquiring HTLV-infection. HTLV- I/II MicroELISA System To detect antibodies against HTLV-I/II, sera were tested with a commercial enzyme immunoassay in which the solid phase (micro wells) were coated with a purified HTLV-I viral lysate, a purified HTLV-II viral lysate and a recombinant HTLV-I p21E antigen (Vironostika HTLVI/II MicroELISA system: Biomerieux, Inc, Durham, North Carolina; Lot No. 43-01808; sensitivity = 100% , specificity = 99.95%). The plates were read at a wavelength of 450nm. Reactive and non-reactive results were then determined according to the instructions of the manufacturers. Statistical Analysis The prevalence of HTLV-I/II antibodies in the different groups were compared using the chi-Square test at 95% confidence level with the aid of the SigmaStat statistical SoftwareVersion 2.0 running on a window NT platform (Jandel Scientific Software, USA). Results Samples were collected from 120 pregnant women, 166 commercial sex workers (CSWs) and 78 secondary school students from Ibadan/Oyo state-Nigeria.The mean ages of the pregnant women and CSWs were 26 years and 23 years respectively.The mean age of the secondary school students (control group) was 13 years. All participants in the study were females. Of the 120 pregnant women tested, 20(16.7%) were found to have antibodies against HTLV while 38 of 166 (22.9%) CSWs were found to have anti - HTLV antibodies. Only 4 of 78 secondary school students had detectable antibodies against HTLV in their sera. Although the prevalence of anti - HTLV antibodies was high amongst pregnant women, that of CSWs was significantly higher (p<0.05). The detailed results are summarized in Table 1 & 2.
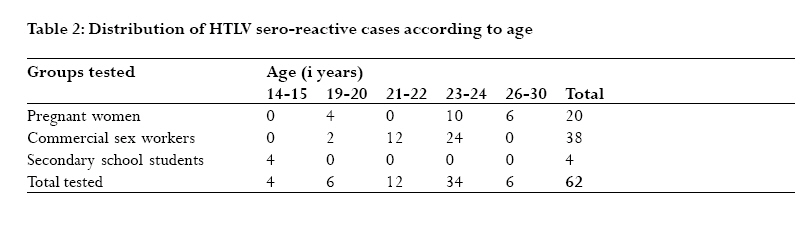
Discussion The assessment of the prevalence of HTLV infection is important especially in endemic areas like Nigeria because transmission of the virus could in some cases result in malignancies. In this study, we report the prevalence HTLV in two important sexually active groups, pregnant women and CSWs in South Western Nigeria.These are a group of people who have a higher risk of contacting, spreading and maintaining the virus in the community.We used an ELISA which is both sensitive and specific (99.89-100%) and which is a method approved by the Food and Drug administration (FDA) for the routine screening of blood donors for HTLV antibodies 20. The result of this study shows that 22.9% of CSWs who participated in the study had antibodies to HTLV (p<0.05). Also, 16.7% of the pregnant women were sero-reactive.This is high although not statistically significant.This is one of the highest percentages of HTLV sero-reactivity ever recorded in Nigeria and this indicates a high prevalence of the virus in the population (Table 1). These finding confirms the strong suggestions by Olaleye et. al.,21 that HTLV infection is predominantly transmitted by horizontal route in Nigeria. The high prevalence of infection seen in CSWs when compared to blood donors and patients with leukemia in Nigeria suggest that this group of people are actively involved in the maintenance and transmission of the virus in the population. Counseling and screening of blood donors and pregnant women for evidence of HTLV infection could be justified due to possible interaction of high risk individuals with the general population. Interestingly, 5.1% of the control group was HTLV sero-reactive (Table 1).This supports the fact that HTLV infection is endemic in Nigeria although less in this group when compared to the highly sexually active groups. Since unfortunately at the current time no vaccines or treatment are available for those with HTLV infection, then knowledge of a person’s antibody status is only helpful from a preventive point of view to substantially reduce the rate of spread of the virus. Mothers who are reactive could be advised not to breastfeed their infants and the use of condoms can be expected to reduce the spread of the virus among persons engaging in sexual intercourse with an infected partner. The lower prevalence in the control group could also be attributable to the lower ages of the participants in this group (14-15 years).The age relatedness of HTLV infection needs a closer look. Previous studies have shown that HTLV infection increases with age from 20 to 40 years14, 22.The increased age may be an indication of greater sexual involvement, which is a major mode of transmission of the virus (Table 2). Perhaps in the future, it would be necessary and helpful to screen virgins and celibates for HTLV infection to further prove this point, as even secondary school students are now known to be sexually involved although not probably as much as pregnant women and CSWs.This will further better define the epidemiology of the virus in Nigeria. We have recorded one of the highest prevalence of HTLV infection in Nigeria among pregnant women and commercial sex workers and it is obvious that these groups of people serve as reservoirs of HTLV in Nigeria. Increasing attention should be given to the routine screening of HTLV in Nigeria as this can make the greatest contribution to reducing the risk of this infection and alter its course in humans. Limitations The assay used was not designed to discriminate between HTLV-I and II infection but it was highly specific and sensitive to detect infection in the same microelisa well. Secondly, confirmatory test for HTLV-I/II was not readily available to us. Despite this limitation, HTLV ELISA has been known to be very sensitive, specific and highly reproducible. Acknowledgement We are grateful to Mr.Aboderin of the Oyo State Hospital, Oyo, for providing the sera from pregnant women. References
Copyright © 2007 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs07026t1.jpg] [hs07026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}