 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 8, No. 1, March, 2008, pp. 57-59 Case Report Intrapartum Rupture of the Uterus Diagnosed by Ultrasound Ogbole GI1, Ogunseyinde OA1, Akinwuntan AL2, 1) Department of Radiology 2) Department of Obstetrics and Gynaecology, University College Hospital Ibadan, Nigeria Code Number: hs08013 Background: Spontaneous uterine rupture is a life threatening obstetrical emergency encountered infrequently in the
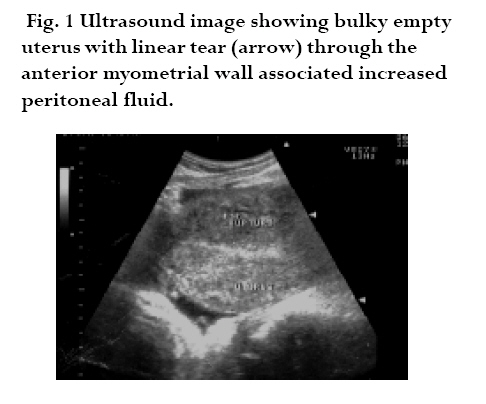
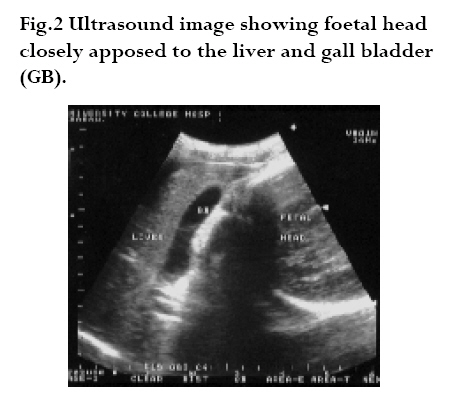
emergency department. Its diagnosis is often missed or delayed, leading to maternal and fetal mortality. Keywords: Intrapartum Rupture, Uterus, Ultrasound Introduction Spontaneous uterine rupture is a serious and potentially catastrophic event and must be considered by emergency physicians in pregnant patients with abdominal pain.1 An incidence of 1 in 167 was reported in Ibadan2, 1 in 416 in Lagos3, compared with 1 in 1,666 for Ireland and between 1 in 1148 and 1 in 2,250 for the USA.4 Modern obstetric practice has caused a decrease in the overall incidence of uterine rupture but a recent report shows that it is on the increase in Ibadan.5 When presented with uterine hemorrhage in a gravid patient, a broad yet focused differential diagnosis is critical to a successful outcome and management. There are a variety of definitions for uterine rupture, but the most accepted one is that of Plauche et al.6 "those cases of complete separation of the wall of the pregnant uterus with or without expulsion of the fetus." Whenever uterine rupture occurs, there is a significant increase in the maternal and perinatal morbidity and mortality. The chance of fetal survival, especially after rupture and expulsion into the peritoneal cavity, is dismal, and mortality rates reported in various studies range from 46 to 70%.7 One of the main risk factors is previous cesarean section. Presented is a case of uterine rupture diagnosed by ultrasonic examination during the first stage of labor in a young woman with two previous cesarean sections. The correct diagnosis led to prompt surgical intervention. Case Report O.M is a 33-year-old mother of two children, from two previous caesarean sections admitted via the gynaecological emergency having been referred to UCH Ibadan from a private health centre at a gestational age of 43 weeks and 3 days. She presented with labour pains of 9 hours, generalized abdominal pains and bleeding per vaginam of 5 hours duration. She presented first at the referral centre where she had booked for antenatal care. Her contractions were said to have been strong and regular but subsequently subsided and became replaced by persistent generalised abdominal pains. She however received no injections or infusions. She felt foetal movements last at the onset of labour. Vaginal bleeding was moderate in nature and contained blood clots. There were no attempts at instrumental vaginal delivery. There was also no history of haematuria, dizziness, fainting spells or progressive abdominal distension. She was booked for antenatal care at the referral centre at a gestational age of 21 weeks and had received two doses of tetanus toxoid. Obstetric ultrasound scan done at 33 weeks, showed a singleton live intrauterine foetus in breech presentation with an anterior placenta and adequate liquor volume. Her two previous deliveries were through caesarean sections in 1997 and 2001 on account of breech presentation in a primigravida and decreased foetal movement following premature rupture of membranes respectively. Examination revealed a young woman in painful distress; she was afebrile, and not pale. Her respiratory rate was 32 cycles per minute and the lung fields were clinically clear. Her pulse rate was 112 beats per minute, regular and of moderate volume. The blood pressure was 160/100 mmHg. Heart sounds were normal. The abdomen was distended with generalized tenderness and guarding. There were no palpable uterine contractions, in spite of patient groaning in pain. The foetal parts were easily palpable. The foetal heart sounds were not heard. Fluid thrill was demonstrated and bowel sounds were absent. The vulva and vagina were normal. There was no active vaginal bleeding. The cervical os and presenting part were high and unreachable. An impression of ruptured uterus with foetal death was made. An abdominopelvic ultrasound scan, obtained in the emergency room showed a bulky empty uterus with a linear serrated sonolucency through the anterior uterine wall in keeping with an extensive uterine tear (Fig. 1). The foetus and placenta were seen outside the uterus in the abdominal cavity with increased intra-peritoneal fluid (Fig. 2). The placenta was seen underneath the anterior abdominal wall with the foetus lying obliquely with the head closely apposed to the inferior border of the liver and gall bladder (Fig. 3). No foetal movement or cardiac activity was seen. An emergency laparotomy was performed. Findings at the operation were consistent with ultrasonic images. Surgical findings included a fresh stillbirth foetus and placenta extruded into the peritoneal cavity, a ragged anterior midline tear extending from the lower to the upper segment and one litre of haemoperitoneum. The extruded baby was delivered by breech extraction along with the placenta. The tear was repaired and the haemoperitoneum drained. She made satisfactory clinical progress and was discharged home on the twelfth post-operative day. Discussion Rupture of a pregnant uterus is one of the life-threatening complications encountered in obstetric practice. Although it may occur in an unscarred uterus, the most common cause of uterine rupture is separation of a previous cesarean section scar. Rupture of the uterus is a major contributor to maternal and foetal morbidity and mortality,1 especially in developing countries.2 Several aetiological factors may be responsible for rupture of the uterus. These include previous hysterotomy, caesarean section, trauma, uterine over distension, uterine anomalies, placenta percreta and choriocarcinoma.4 The relative incidence of the factors will depend on the level of obstetric practice in the community. A review in Ibadan noted a positive history of previous trauma in 73.6% of cases, the lower segment caesarean section constituting 52% of these and prolonged obstructed labour contributing in 45.4% of the cases.6 The only identifiable predisposing factor in our patient was two previous caesarean sections, which is the most common factor. Both the maternal and the foetal prognoses are worsened by delay in the correct diagnosis. Although the use of ultrasound in obstetrics is routine nowadays, very little has been written about the possibilities in connection with the rupture of the uterus.8 This catastrophe might have been avoided if an emergency caesarean section had been resorted to earlier at term. A combination of poverty, ignorance, illiteracy and aversion to abdominal delivery has been cited as being responsible for this grim state of affairs.2 Diagnosis of ruptured uterus in this patient was fairly straight forward, given the history of two previous caesarean sections, abdominal pain, cessation of labour and foetal movements, and the clinical findings of vaginal bleeding and easily palpable foetal parts, followed by an ultrasonographic confirmation of a tear. Abdominal pain and vaginal bleeding are the commonest modes of presentation in Ibadan.5 Ultrasonography is probably the safest and most useful imaging technique during pregnancy. Extra-peritoneal haematoma, intrauterine blood, free peritoneal blood, empty uterus, gestational sac above the uterus, and large uterine mass with gas bubbles have been reported as sonographic findings associated with uterine rupture.9,10 Free peritoneal blood, empty uterus, and an extra uterine foetus were some of the findings in our patient. Obstetric consultation in all pregnant women with abdominal pain must be considered.11 In addition, if the pregnancy is advanced, foetal well-being can be established with ultrasonography. The management of ruptured uterus is laparotomy as soon as possible, after resuscitation has been commenced. The correct surgical procedure is that which is the shortest, taking into consideration the surgeon's skill12 References
Copyright © 2008 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs08013f1.jpg] [hs08013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}