 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 1, March, 2009, pp. 26-33 Factors influencing disclosure of HIV positive status in Mityana district of Uganda Isaac Kadowa1, Fred Nuwaha2 1 Mityana Hospital, P.O.Box 52 Mityana, Uganda. Tel: +256-(0) 77-468777. E-mail: kadisaac@yahoo.com Code Number: hs09005 Abstract Background: Disclosure of HIV positive sero-status to sexual partners, friends or relatives is useful for prevention and
care. Identifying factors associated with disclosure is a research priority as a high proportion of persons living with HIV/AIDS (PHA)
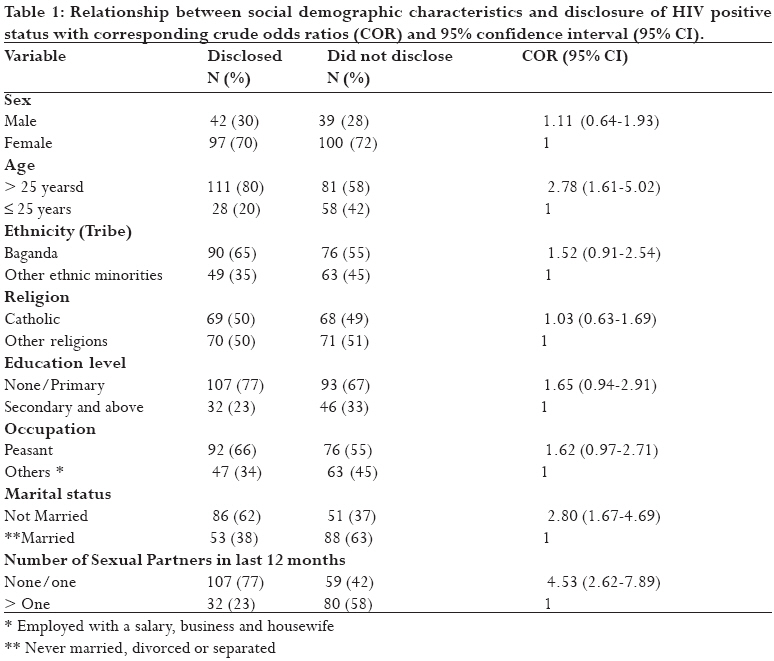
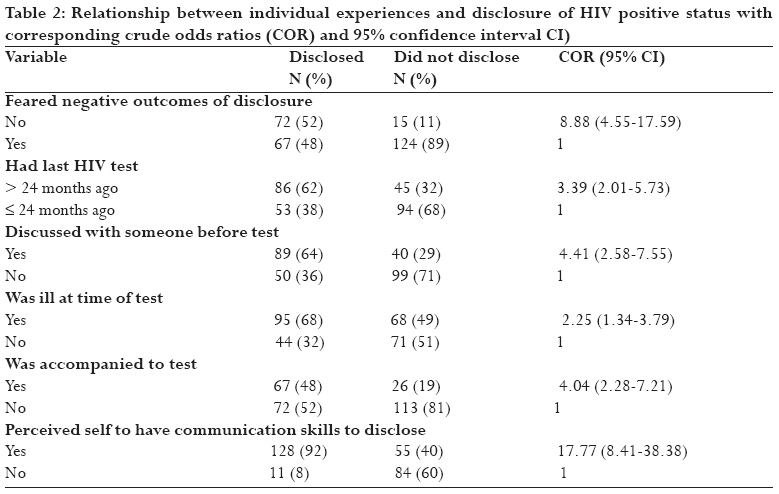
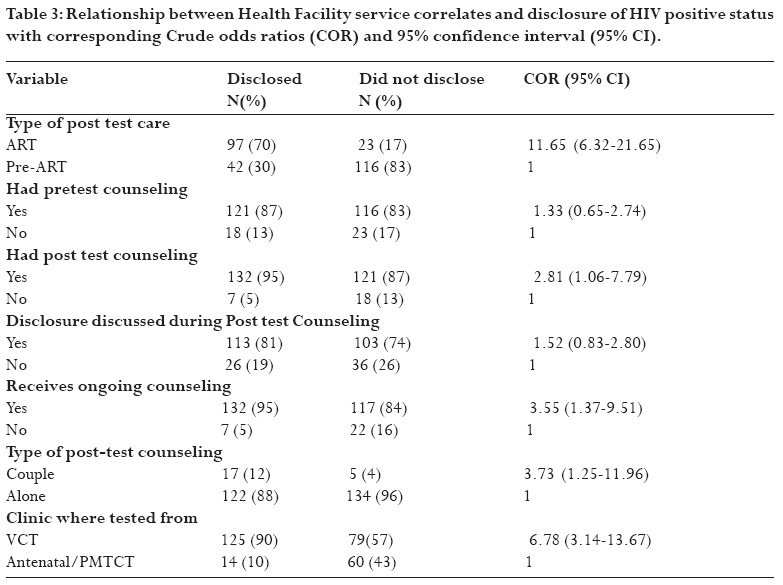
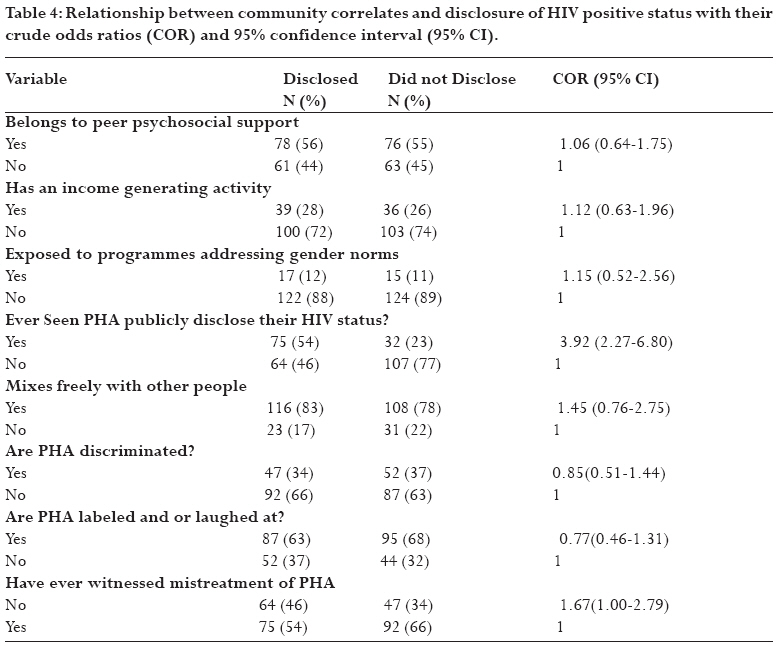
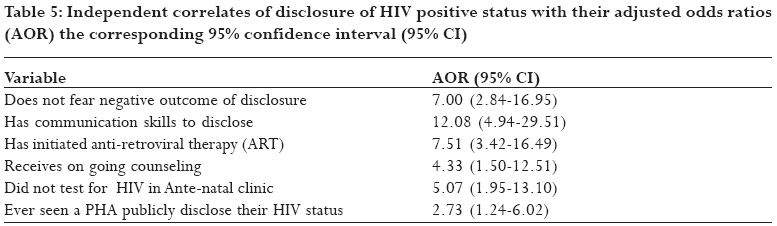
never disclose. Key words: HIV/AIDS, disclosure, communication skills, HAART, HIV counselling and testing, Voluntary counselling and testing, HIV care, ongoing counselling Running title: Disclosure of HIV positive status Introduction Disclosure of HIV positive sero-status to sexual partners and or close relatives and friends (significant others) is an important public health strategy because it offers a number of benefits to the infected individual and to the general public. 1, 2 HIV counselling and testing (HCT) programmes as well as post test care services such as of antiretroviral therapy (ART) and pre-ART care, emphasize HIV status disclosure among persons living with HIV/AIDS (PHAs). Disclosure to significant others would provide emotional and psychological support to PHAs whereas disclosure to sexual partners could lead to the partners also undertaking HCT. 3, 4 Since disclosure creates the awareness of HIV risk to untested sexual partners, it subsequently leads to greater uptake of HCT. 5. Furthermore, disclosure to sexual partners enables couples to make informed reproductive health choices that may ultimately lower the number of unintended pregnancies among HIV positive couples, and even reduce the risk of HIV transmission from the mother to child (MTCT). 6-10 Not only does disclosure motivate people to reduce risky sexual behaviours thereby decreasing the transmission of HIV, but it is also associated with improved access to HIV prevention and treatment programmes and with better treatment outcomes via improving adherence to ART. 3, 4 Inspite of all antecedent benefits of disclosure some people may decide to keep their positive HIV status a secret, others may disclose partially to specific people while others may have full/public disclosure. 1, 2 Indeed the disclosure of HIV positive status has potential risks such as blame, divorce, abandonment, physical and emotional abuse, discrimination and stigma, as well as loss of custody of children and property especially for women. 1, 8 The rates of disclosure from various studies in low income countries range from 16.7% to 86%, with the lowest rates (16.7% to 32%) being among pregnant women tested in antenatal care in Sub-Saharan Africa. 1 According to the 2003-2006 HIV/AIDS records obtained from Mityana District Uganda, only 43% of PHAs attending post test care had disclosed their sero-status to sexual partners and or to close relatives and friends. Thus, there is need to understand factors associated with disclosure of HIV positive status among PHAs with a view of suggesting measures for increasing the rates of disclosure. Methods Setting The study was conducted in Mityana District Uganda between 1st March and 15th April 2007 at health facilities that provide HIV/AIDS post test care services. Mityana District lies in the Central Region of Uganda 68 kilometres west of the capital Kampala. The district has a population of 266,108 people, with females equal to males. 11 It is estimated that 10.6% of the adult population in the district is HIV positive and of the PHA who know their sero status about 51% attend post test care services. 12 Twelve health facilities provide HIV counselling and testing (HCT) and post test care services, out of which four provide anti-retroviral therapy (ART). Counsellors discuss and encourage the clients to disclose their HIV positive status during pre-test and post-test counselling sessions and during attendance of treatment and care programmes. Voluntary counselling and testing (VCT) and Prevention of mother to child transmission (PMTCT) have been implemented in the district since 2002. Testing at the PMTCT/antenatal care clinic is done routinely and the pregnant women are encouraged to bring their partners along for HCT. However, less than 5% of the men test for HIV along their pregnant women. The Aids Model District project (AIM) which was operating in the district facilitated several PHAs in income generation and supported the initiation of psychosocial peer support groups and post test clubs. UNICEF also supported the sensitization of the community about negative gender norms such as those aimed at reducing partner violence and sexual abuse. This sensitization was done through several initiatives such as workshops, community dialogue (community members' discussion groups), and through radio programmes. Design We conducted an un-matched case control study to compare 139 PHAs who had disclosed their HIV positive sero-status with 139 PHAs who had never disclosed their HIV positive sero-status to sexual partners and or to close relatives and friends. This sample size is enough to identify factors associated with disclosure with a power of 80% at 95% confidence interval if the prevalence of factors influencing disclosure is between 10 and 90% in the study population (Epi Info 2000 CDC, Atlanta, Georgia). Selection of study participants The number of respondents consecutively interviewed from each of the twelve health facility was obtained by dividing the registered attendance per facility by total district attendance then multiplied by the total sample size. Only clients who had known their HIV status for at least 12 months were invited to participate. A case was a PHA who attends post test care and had disclosed his/her HIV positive status to at least one other person, either a sexual partner for those who had partners and or to a close relative/friend. A control was a PHA who had not disclosed their HIV positive status to any of the above people. Data collection A pretested semi structured interview schedule was used to collect data. Four trained research assistants (2 males and 2 females) who were clinical officers or registered nurses with experience in HIV/AIDS care interviewed the PHAs. The average length of each interview was 30 minutes. Female interviewers interviewed the women whereas men were interviewed by male interviewers. The interviews were conducted in Luganda the local language. The interview schedule was translated from English into Luganda during the training of the research assistants and thereafter back translation was done to ensure that there was no loss of meaning. Most people from the ethnic minorities understood Luganda. Dependent variable: Disclosure status was the outcome of interest. This was specifically whether the PHA had disclosed to a sexual partner, and or a close relative/friend. Independent variables: These were sex, age, ethnicity, level of education, occupation, marital status, number of sexual partners in the previous 12 months; fear of negative outcomes of disclosure, time since HIV test was done, prior discussion with another person to undertake HIV test, health status at time of test, whether PHA was accompanied by another person for the HIV test, perceived adequacy of communication skills; type of HIV care (ART or pre-ART), type of counselling received (pre-test, post-test, ongoing counselling, individual or couple), clinic where HIV testing was done (whether VCT or PMTCT/ante-natal care); income generating activity by PHA, psychosocial support, being exposed to programmes addressing negative gender norms, having witnessed discrimination of PHA, and having ever seen PHA openly declare their HIV positive sero-status. Analysis SPSS statistical software package version 12.0 (SPSS Inc., Chicago, IL) was used to analyze data. First, we carried out univariate analysis to generate frequencies and proportions and secondly bivariate analysis to test for association between the independent and the outcome variables. The strength of association was determined using crude odds ratio (COR) with 95% confidence intervals (CI). Finally we did multivariate analysis using binary logistic regression with backward elimination procedures. All variables which were significant at bivariate analysis and known predictors of disclosure of HIV sero-status from other studies were used in the multivariate analysis. Adjusted odds ratios (AOR) were calculated after the logistic regression. Ethical consideration The study was approved by the Research and Ethics Committee of Makerere University School of Public Health and the Uganda National Council for Science and Technology. Permission to collect data was sought from district authorities and the in charges of the health facilities. Informed consent was obtained from participants before interview. Results The 278 respondents were predominantly female (71%), mostly peasant farmers (60%), and 72% either had no education or stopped in primary school. The mean age of those who disclosed was 38.2 years (SD = 10.5) compared to 31.0 years (SD = 11.1) for those who never disclosed. The difference in mean age between the two groups was statistically significant (t = 5.54, P = 0.005). The majority 166/278 (60%) of the respondents were Baganda by tribe and 49% were Catholics by religion. Of the respondents 74 (27%) had tested during ANC, and 204 (73%) at VCT clinics. One hundred and twenty out of 278 (43%) had initiated anti-retroviral therapy (ART). Reasons for disclosure or non-disclosure Among the 139 people who had disclosed, 91/139 (66%) had sexual partners and 73/91 (80%) of PHA with sexual partners had disclosed to them. Most 125/139 (90%) had disclosed to multiple people including their parents (30%), siblings (34%), children (20%) other close relatives (34%) and close friends (50%). The main reasons cited for disclosure were multiple and included to get financial and social support 48/139 (35%) followed by the need to get treatment 46/139 (33%) and 45/139 (32%) said they wanted their partners to also undertake the test. Among the 139 people who had not disclosed, 88/139 (63%) had sexual partners. The reasons cited for their non disclosure were fear of divorce and violence 58/139 (42%) for those in sexual relationships, fear of discrimination and stigma 40/139 (29%), fear of rumour mongering 29/139 (21%), fear of accusation of promiscuity/infidelity 32/139 (23%), and 11/139 (8%) said that they saw no reason to disclose. Asked whether they need any kind of support to disclose, the majority 72/139 (52%) said they did not need any support, while 38/139 (27%) said they need skills of telling others about their status. Factors associated with disclosure The association of socio-demographic, sexual behaviour, individual experiences, health facility services, and community factors on disclosure of HIV positive status to sexual partners, relatives and friends were assessed. Social demographic characteristics Comparison of clients who disclosed (cases) with those who had not disclosed (controls) regarding socio-demographic factors and sexual behaviour at bivariate analysis is shown in Table 1. Respondents who were more than 25 years of age, who were not married and those who had less than 2 sexual partners in the last 12 months were more likely to disclose their HIV positive status. There was no significant difference between the cases and controls in relation to sex, tribe, education level, religion and occupation. Individual experiences Table 2 shows that respondents who did not fear negative outcomes of disclosure, those who tested more than 24 months ago, those who discussed with another person to undertake the HIV test, those who were ill at the time of testing, those accompanied by another person to the testing site, and those who perceived themselves to have communication skills to disclose, were more likely to disclose their HIV status. Health facility factors Table 3 shows that respondents who had initiated ART, who received post-test counselling and ongoing counselling at every clinic visit, who tested at voluntary testing and counselling clinic (VCT) and those who were post-test counselled as a couple were more likely to disclose. Discussion of disclosure during post-test counselling and having had pre-test counselling did not influence disclosure to significant others. Community factors Table 4 shows that respondents who had ever seen PHA publicly disclose, and those who had never witnessed mistreatment of PHA were more likely to disclose their HIV status. Belonging to a peer psychosocial support group, having an income generating activity, and being exposed to programmes that address negative gender norms did not influence disclosure. Similarly perceiving PHA as mixing freely with other people, and that PHA are discriminated, labelled or laughed at were not significantly associated with disclosure. Key factors associated with disclosure of HIV sero-status Multivariate analysis (Table 5) showed that the independent factors that favour disclosure were not fearing negative outcomes of disclosure adjusted odds ratio (AOR) 7.00, 95 % confidence interval (95% CI) 3.03-16.95, having communication skills to disclose (AOR 12.08, 95% CI 4.94-29.51), having initiated anti-retroviral therapy (AOR 7.51, 95% CI 3.42-16.49), not having tested for HIV during ante-natal clinic (AOR 5.07, 95% CI 1.95-13.10), receiving ongoing counselling (AOR 4.33, 95% CI 1.50-12.51) and having ever seen a PHA publicly disclose their HIV status (AOR 2.73, 95% 1.24-6.02). The multivariate model with these 6 variables showed that 70% of the variation in the dependent variable which is the disclosure status can be explained by the factors in the regression model (Nagelkerke R2 = 0.70). Discussion This study aimed to identify the independent predictors of disclosure of HIV positive status among PHAs. One limitation of the study is that disclosure was assessed at one point in time yet disclosure is a process and not a single event. 13 The decision to disclose consists of several steps, including adjusting to the diagnosis, assessing one's disclosure skills, deciding whom to tell, evaluating the recipient's circumstances, anticipating the recipient's reaction and having a motivation to disclose.13 Therefore studying disclosure at one point in time may not reveal all these attributes. Another limitation is the wide confidence intervals meaning that the power of the study may be low. Despite these limitations, very important correlates associated with disclosure are identified. Clients who experienced fear of negative consequences of disclosure were less likely to disclose their HIV positive status. Specifically people mentioned fear of divorce, discrimination and stigma, rumour mongering, violence from their partners and fear of being accused of infidelity. These findings are similar to those in published literature 14-18 and could be explained from applied social psychology where attitudinal outcome beliefs such as these are extremely important in predicting behaviour. 19, 20 People who reported to have good communication skills were more likely to disclose their HIV positive status. Indeed other studies have showed that personal communication skills and communication patterns are important determinants of disclosure. 13, 21 The skills to effectively communicate are quite important in patient's negotiation and decision making around disclosure. Perceived good communication skills may be related to the individual's inherent self confidence in dealing with potentially confrontational situations such as disclosure to significant others. The circumstances under which people get tested and the services and type of care they receive thereafter have been shown to be important determinants of disclosure. 1, 16 This study showed that people who were on ART were more likely to disclose compared with people who were not on ART. This could be explained by the fact that people on ART receive pre ART counselling where disclosure is emphasized as a precondition and requirement for starting the treatment. Secondly ART in low income countries is initiated by people who have already developed overt AIDS symptoms and signs that cannot easily be concealed from people. In addition people on ART have closer follow-up as well as continuous ongoing counselling and guidance. Our study showed that people who received ongoing counselling at every clinic visit were more likely to disclose. This might be due to the fact that during ongoing counselling issues and doubts about benefits of disclosure is adequately addressed. The finding agrees with other studies that showed that rates of disclosure increased with the number of times that a health professional discussed issues of disclosure at the HIV clinic where clients received care. 21, 22 In a Tanzanian study for instance men and women were reported to have mentioned the important role counsellors played in their decision to disclose. 16 The clinic where the HIV test was done was independently associated with disclosure. People tested at the antenatal/PMTCT clinic were less likely to disclose compared with people tested at the Voluntary Counselling and Testing (VCT) clinic. The extensive decision making that people who present to VCT have gone through have been described elsewhere. 16 It has been reported that the people who test at VCT were motivated to test by their high perception of risk of HIV, they have possibly thought about testing for a long period of time prior to being tested and many could have talked with their significant others about HIV risk and HIV testing prior to the test. In contrast it may reasonably be assumed that people from antenatal /PMTCT clinics have generally not thought about HIV testing prior to being offered the opportunity as part of their antenatal care, and as such most of these people have not talked with their significant others about the need to test. We also showed that people who have witnessed a PHA publicly disclose their sero-status were more likely to disclose. Probably witnessing public openness about HIV may motivate PHAs to disclose by increasing self-efficacy. 23 Besides witnessing openness of disclosure may ensure that the perceived negative outcomes of disclosure may after all not be real. 24 Implications for interventions Our findings imply that in order to increase rates of HIV status disclosure to sexual partners and or close relative and friends among PHAs, special emphasis should be made to support and counsel clients who test in antenatal/PMTCT clinics, those who have not initiated ART and those that express fear of negative outcomes. Voluntary counselling and testing compared to routine counselling and testing (as done in PMTCT) improves disclosure. This means that HIV counselling and testing including disclosure of results should be promoted in community HIV programmes so that people have gone through the mental challenges of disclosure before actual testing in PMTCT programmes. Our data also suggest that improved skills in interpersonal communication are needed for disclosure and the skills can be achieved through training of post test care clients by use of appropriate methods such as rehearsal techniques, role plays, videos, and drama. 1 These data also suggest that ongoing counselling for PHAs is essential and since witnessing PHA disclosing increases the rate of disclosure, the effectiveness of messages through such ongoing counselling may be improved by use PHAs as peer counsellors. Acknowledgements We would like to thank the research assistants John Mwesigwa, Isaac Lubega, Mary Gorretti Nalwoga, Margaret Asiimwe and Flora Mawanda for taking part in data collection. Grateful thanks to Mityana district health sector and the Makerere University School of public health for the financial support. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09005t2.jpg] [hs09005t1.jpg] [hs09005t5.jpg] [hs09005t3.jpg] [hs09005t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}