 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 2, June, 2009, pp. 109-117 Intra-household differences in health seeking behaviour for orphans and non-orphans in an NGO-supported and non-supported sub-county of Luwero, Uganda Wilson Winstons Muhwezi1, Denis Muhangi2, Firminus Mugumya2 1Department of Psychiatry, Makerere University College of Health Sciences, School of Medicine P.O. Box 7072 Kampala. Tel:
+256 772 430 287. E-mail: wmuhwezi@med.mak.ac.ug; wilsonmuhwezi@hotmail.com Code Number: hs09019 Abstract Objective: Comparing healthcare dynamics among orphans and non-orphans in an NGO supported and a non-supported
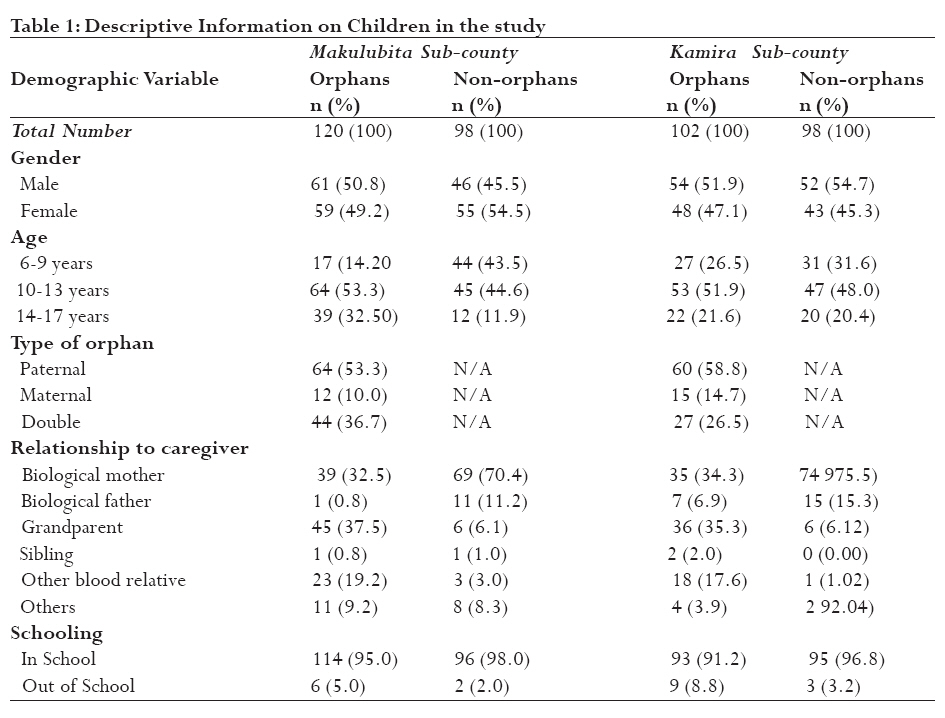
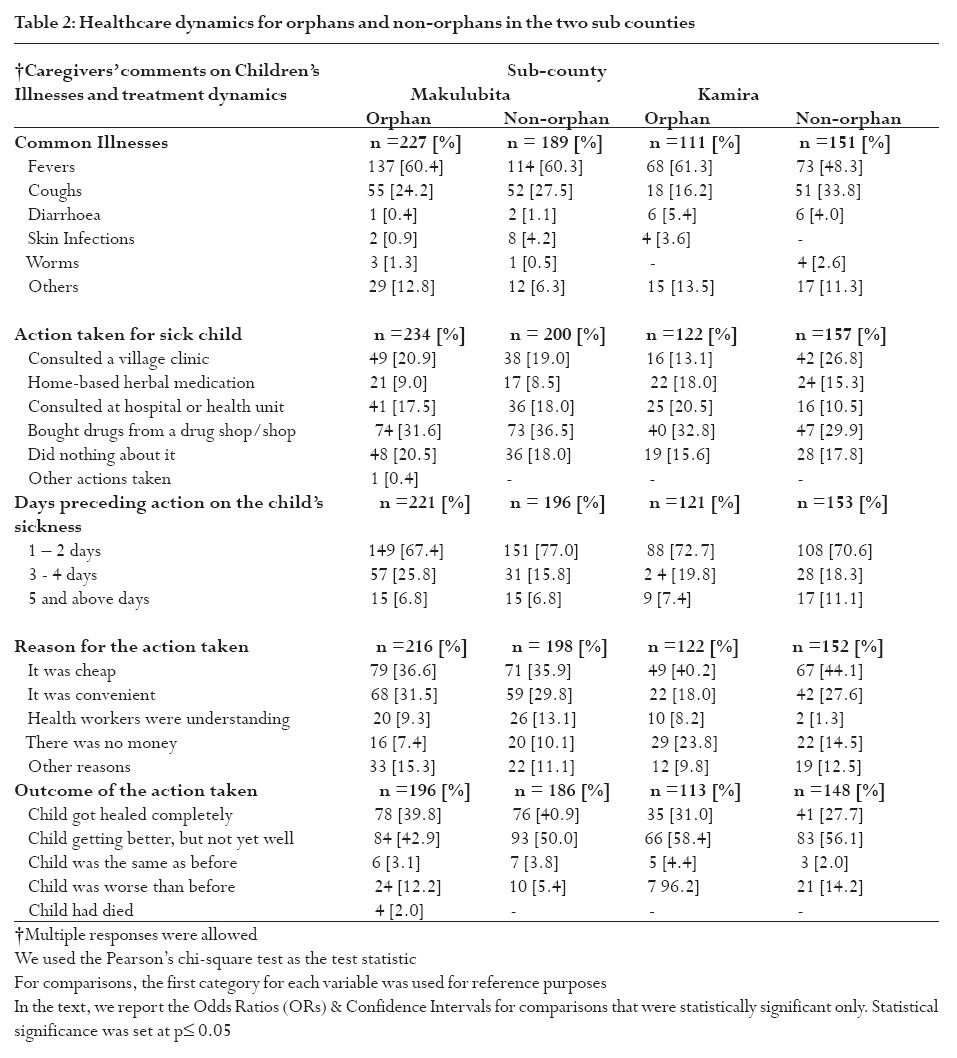
sub-county so as to identify the level of equity. Key words: Orphans; caregivers; health seeking behaviour, Uganda, discrimination, NGO support Introduction Globally, the number of orphans is increasing and estimates suggest that it is expected to hit 40 million in 23 developing countries by 2010 1. In Uganda, orphans were estimated to be more than 2 million constituting about 20% of all children in the country 2. Therefore, it is not surprising that the issue of orphanhood attracts significant attention. Most of the orphans live and are cared for within their communities 3. The majority of orphans are under the care of female-headed families, and caregivers are usually grandmothers or surviving mothers 4, 5. The orphans are in most cases a burden to the extended families and friends and in most cases, they increase the dependency ratio within the households 6. Compared to non-orphans, more orphans are known to drop out of school or have most of their educational requirements and needs remaining unmet 7-9. Most literature about orphans has suggested that they are children who grow up without the care and support of their families, who have poorer learning and knowledge levels, and who suffer from the absence of adults in their socialization 10. Few studies have explicitly assessed intra-household differences in health seeking behaviour between orphans and non-orphans 11. Many international and local Non-Governmental Organisations (NGOs) have set up programs in Uganda to help orphans. In spite of the many years of NGO support, there is lack of a common understanding about the contribution of the support to closing the gap between orphans and non-orphans. This paper discusses health seeking behaviour of orphans and non-orphans in light of the role played by the Association Francois-Xavier Bagnoud (AFXB), an international NGO that supports orphans in Luwero District, Central Uganda. AFXB whose origin is from Switzerland has worked in Luwero District since 1990 covering three sub-counties of Semuto, Makulubita and Kasangombe (In Uganda, a sub-county is a geographical jurisdiction that constitutes a Local Government level with an elected council as established by the Local Governments Act 1997). There are more than 30 such sub-counties in Luwero district, each with a total population of between 25,000 to 70,000 people. To appraise the role of NGOs in ensuring equity of care for orphans and non-orphans in Uganda, AFXB was selected as a unique case for this study. Secondly, the NGO specifically targets improvement of the well-being of orphans. By the time of doing fieldwork for the research, the NGO had operated in Luwero District for over 10 years, a considerably longer period. The primary goal of AFXB which is synonymously referred to as the NGO in this paper is to strengthen the capacity and improve the life conditions of HIV-positive people and to reintegrate orphans and vulnerable children who are affected by or infected with HIV and AIDS in their communities. The main program activities of the NGO include; capacity strengthening through supporting primary education for orphans and other vulnerable children; enhancing socio-economic security through provision of assistance to children's guardians to undertake income generating projects (IGAs) so that they acquire capacity to generate resources to meet orphans' basic needs like healthcare; child protection by safeguarding rights of orphans; care and support for health particularly in sensitization of communities about HIV/AIDS prevention and positive living, HIV/AIDS care and treatment; food security and nutrition and, psychosocial support12. The NGOs' strategy consists of a community-based approach, with emphasis on involving guardians and the entire community to facilitate formation of community based structures in form of committees to oversee implementation of her aims and objectives. Ultimately, AFXB assists Ugandans in her areas of operation to evolve community-based solutions for problems faced by orphans, and equips them to be able to meet the basic needs of orphans. Despite the 3 years of AFXB support to orphans and vulnerable children in Uganda, there was little understanding of the impact of the support on healthcare needs of supported children hence the reason for this research. Whether NGO support has closed the welfare gap between orphans and non-orphans was not known. Specifically, the impact of the NGO's support on orphans' health seeking behaviour and patterns had not been investigated before. Internal monitoring by the staff of the NGO and external program reviews indicated positive results, but also pointed to certain deficiencies in program effectiveness 13. No comparisons had been made between households that received the NGO support and those that did not. In summary, the degree to which the NGO support had translated into better satisfaction of orphans' needs like meeting healthcare costs was poorly understood. This study therefore sought to fill these information gaps and to generate additional information about support services for orphans. With respect to health seeking behaviour, the objective of this article is to compare key healthcare dynamics among orphans and non-orphans in the NGO supported sub-county and the non-supported sub-county to establish the level of equity in orphan care. Another aim was to analyse the differences in healthcare dynamics between orphans and non-orphans within the two sub-counties and the magnitude of the difference. Methods The study setting The study was carried out in Makulubita and Kamira (at the time of the study, all other sub-counties in Luwero District had one or more forms of orphan support except Kamira. None of the NGOs in Kamira sub-county was providing support targeting orphans) sub-counties of Luwero, a district with an estimated orphan population of about 16,575 by 199114. Makulubita is the sub-county where AFXB's support for orphans had been taking place since 1996. Kamira was a control sub-county in the study since it resembled Makulubita in aspects like; orphan prevalence, HIV/AIDS prevalence, resource base, demography, geographical location, and political history. The only exception was that Kamira had no orphan support from any NGO at the time of doing fieldwork for this research. Research design A cross-sectional unmatched case-control research design was used. Makulubita where NGO support for orphans existed was used as the case while another sub-county, Kamira, where no similar NGO support existed was used as the control. Three main strands of comparisons were carried out; (i) between orphans in Makulubita and Kamira sub-counties, (ii) between orphans and non-orphans in each of the two sub-counties, and (iii) between the differences in orphans and non-orphans in the two sub-counties (difference of the two differences in (i) & (ii) above). Sample size The Sample size was determined using the STATCAL Calculator (EPI-INFO 6.04b) for an unmatched case-control design. The desired significance level was 95% and a power of 80%. Using these parameters, the minimum required sample size was calculated to be 195 children (an equal number of orphans and non-orphans) in Makulubita sub-county and 195 children (an equal number of orphans and non-orphans) in Kamira sub-county. A total of 98 children for each group was therefore derived and studied, making a total of 392 children from 392 households. From each selected household, one caregiver and one child (either orphan or non-orphan depending on the orphan status of the household) was selected in the sample. Orphans were selected from households that had at least one orphan while non-orphans were selected from households without any orphan at all. Through a simple random sampling technique (lottery method), 15 village clusters from where the sample was recruited were chosen from each sub-county making a total sample of 30 villages. Caregivers of children that participated in the study gave informed written consent for their children to participate and the children gave written assent. Research instrument All study participants were interviewed to complete a demographic data sheet, which had questions on gender, age, marital status, ethnicity, religious affiliation, number of children, and size of family, family structure, educational attainment and occupation. In addition, a number of pre-coded questions to tap into healthcare dynamics were asked to study participants. Questions were asked about; (i) common illnesses that children used to suffer from, (ii) whether any children in the household had been sick over the last 2 weeks, (iii) who of the children had been sick, (iv) action taken when the child/children fell sick, and (v) the reason for the action taken. Children were asked questions about: (i), whether they suffered from any of the common physical illnesses over the last 2 weeks (ii) action taken when they fell sick and (iii) if nothing was done, the reason for that. The questions were designed by the researchers. To ensure that each interviewee remained anonymous, the research instrument had no personal identifiers. Data collection Fieldwork to collect data for this research was conducted between the 29th July 2003 and 16th August 2003 in the sub-counties of Makulubita and Kamira. To ensure a high response rate among a largely illiterate/semi-literate study population, face-to-face interviews were conducted, using structured interview schedules in Luganda. All instruments were translated from English to Luganda and back-translated by Luganda speakers fluent in English, thereby ensuring content validity, achieving conceptual equivalence and cultural sensitivity. To attain face validity, the interview schedule was first pre-tested on respondents similar to study participants from the neighbouring sub-county. The pre-tested version of the questionnaire was also peer-checked by other researchers, thereby checking content and criterion validity again. Following the comments raised, appropriate changes on the suitability of instruments from the pre-test participants were made. Conducting of interviews Interviewers were all University graduates of social sciences who had prior experience in data collection. They were offered more training about the study, field surveys, data collection methods, dynamics of fieldwork, content of research instruments, and their ethical obligations as interviewers. All respondents were interviewed in private to minimise interruptions, elicit candid individual responses and to ensure confidentiality. Female research assistants interviewed female children to ensure candid responses. Ethical considerations Ethical clearances were obtained from the following sources: the Uganda National Council for Science and Technology, Boston Medical Centre Institutional Review (Human Studies Committee), the political leadership of Luwero District, and the local leaders of villages and households visited. Conduct during the study adhered with the Helsinki Declaration 15. After identifying potential respondents in households, researchers identified themselves and explained that the study was interested in orphan-care, education, health and other living conditions and the role of AFXB. For children, their caregivers had to consent on their behalf but each child had to assent to be interviewed. Although the study exposed no potential harm to the participants, all the researchers got prior training on how to be sensitive while interviewing. No interview was terminated before concluding and achieving closure of any emotional discomfort caused to the respondent. Although anticipation was that some participants while being interviewed could experience emotional turbulence due to being reminded about losses that they would have preferred to forget and would therefore need referral for professional specialist attention, none of them showed such a reaction. Data management and statistical analyses Data was entered in EpiInfo computer programme and exported to the Statistical Package for Social Scientists (SPSS) version 10.0 for cleaning, editing and analysis. Comparisons were made basing on pre-determined study parameters. Descriptive statistics like frequencies and percentages were generated. To explore relationships between variables, correlation statistical tests were used including use of frequency distributions and 2-way contingency table (Pearson's chi-square) and unadjusted odds ratios. The level of statistical significance was set at 5% (i.e. p ± 0.05). ResultsDemographic characteristics of study participants From the sample of orphans and non-orphans that participated in the study, male children were slightly more than females. The age range of children in the study was from 6 to 17 years. Among the orphans, majority above summarises the demographic characteristics of the children (orphans and non-orphans) in the study. On the other hand, data on caregiver characteristics (reported elsewhere) had a majority who were females16. Females were 85.4% in Makulubita sub-county and 81.6% in Kamira sub-county. Most caregivers (80.4%) were middle-aged (ranging from 18-54 years). While close to half of caregivers of orphans and non-orphans were in monogamous marital relationships, more than one quarter was widowed. By occupation, a big proportion of the caregivers in the study was of peasant cultivators, and was of Baganda. More than half of the caregivers in the study had attended some primary school, but had not completed this level of education16 Illnesses common among children in the ctudy and control sub-counties There were no significant differences between orphans and non-orphans in the two sub-counties in terms of reporting illnesses they suffered from in a period of two weeks before the study. Fevers were reported to be the most common health problem affecting orphans in the two sub-counties. There were 137 (66.8%) orphans that were reported to have had fevers in Makulubita, compared to 68 (33.2%) in Kamira and the difference was not significant. However, 1 (14.3%) of children reported an experience of diarrhoea in Makulubita as opposed to (6) 85.7% in the control sub-county [Crude OR 12.1; 95% CI: 1.40-276.19; ÷2 = 6.08; p = 0.014]. Using fever as a basis for comparison again, 2 (20%) of the orphans in Makulubita county reported presence of skin infections, a proportion significantly smaller than 8 (80%) in Kamira sub-county [Crude OR 8.06; 95% CI: 1.53-56.5; ÷2 = 7.22; p = 0.008]. Although the orphans suffering from diarrhoea and skin infections in Makulubita where NGO support existed were significantly fewer than in control sub-county, the confidence intervals for the test statistic were too wide implying the need to be cautious in drawing incisive conclusions from such findings. The result could have been accidental given the small sample sizes of orphans with the two illnesses. However, it is important to note that orphans in Makulubita were not different from non-orphans in terms of suffering from fevers [137 (60.4%) versus 114 (60.3%)] and coughs [55 (24.2%) versus 52 (27.5%)]. On the other hand, majority of orphans as opposed to non-orphans in Kamira reported significantly higher proportions with fevers [68 (79.1%) versus 18 (20.9%)] compared to coughs [73 (58.9%) versus 51 (41.1%)] respectively (Crude OR 2.64; 95% CI: 1.35-5.23; ÷2 = 8.49; p = 0.004). Therefore, significantly more orphans in a sub-county without NGO support seem to be more bothered by fevers compared to coughs. Action taken about children's illnesses in the control and study sub-counties After comparisons of orphans together and doing the same for non-orphans, there was no significant difference between actions taken for orphans' and non-orphans' illnesses in the two sub-counties. However, when orphans fell sick, their caregivers in Makulubita as opposed to those in Kamira sub-county had a significantly higher tendency to consult village clinics compared to home-based herbal medication as reflected in the respective proportions [49 (75.4%) versus 16 (24.6%)] and [21 (48.8%) versus 22 (51.2%)] (Crude OR 3.21; 95% CI: 1.31-7.96; ÷2 = 6.88; p = 0.009). Appreciation of the role of modern biomedical healthcare for orphans appeared to be significantly higher in a sub-county with NGO support. Again, in Makulubita sub-country, there was no significant difference in terms of caregivers either accessing healthcare from village clinics or government-supported hospitals/health centres for orphans and non-orphans. On the contrary, a significant majority of caregivers for orphans compared to those for non-orphans in the control sub-county tended to take them to village clinics as opposed to hospitals/health centres as reflected in the respective proportions [42 (72.4%) versus 16 (39%)] and [16 (27.6%) versus 25 (60.1%)] (Crude OR 4.10; 95% CI: 1.61-10.57; ÷2 = 9.70; p = 0.002). It therefore looks as if orphans in the control sub-county which had no NGO support were less likely to be seen by health workers in hospitals/health centres. In control sub-county, fewer caregivers sought healthcare from village clinics or other formal health care providers, as opposed to buying drugs/medicines from drug-shops or general merchandise shops [42 (47.2%) versus 47 (52.8%)] compared to respective decisions for non-orphans in the same area [16 (28.6%) versus 40 (71.41%)] (Crude OR 2.23; 95% CI: 1.03-4.86; ÷2 = 4.82; p = 0.040). Number of days taken before taking action on an orphan and a non-orphan's sickness In Makulubita sub-county alone, there was a significantly bigger number of caregivers that took fewer days (1-2) to seek healthcare for non-orphans as opposed to taking 3-4 days [151 (82.9%) versus 31 (17.1%)] compared to respective decisions for orphans in the same area [14 (19.7%) versus 57 (80.3%)] (Crude OR 19.83; 95% CI: 9.36-42.70; ÷2 = 87.3; p = 0.000). Similarly, a significant bigger number of caregivers took fewer days (1-2) to seek healthcare for non-orphans as opposed to taking many days (5 and above) [151 (90.9%) versus 15 (9.1%)] compared to respective decisions for orphans in the area [14 (48.3%) versus 15 (51.7%)] (Crude OR 10.79; 95% CI: 4.01-29.42; ÷2 = 31.36; p = 0.000). However, when orphans fell sick, caregivers in the control sub-county as opposed to Makulubita had a significantly higher tendency to seek healthcare faster (1-2 days) compared to later (3-4 days) as reflected in the respective proportions [88 (87.3%) versus 14 (13.7%)] and [24 (29.6%) versus 57 (70.4%)] (Crude OR 58.65; 95% CI: 6.74-33.65; ÷2 = 58.65; p = 0.000). The explanation for these differences was not clear. It is possible that the questions which elicited this data were not discriminatory enough. Perhaps, the span of 1 to 5 days as the spectrum within which to seek healthcare was too close to be differentiated by study participants. Reasons for the action taken when an orphan or a non-orphan fell sick Respondents in the two sub-counties were asked for the reason that triggered their decision to seek healthcare for a sick orphan or a non-orphan. It is vital to note that a significantly smaller number of caregivers for orphans in the control sub-county as opposed to Makulubita opted for the healthcare action of their choice because it was perceived to be cheap at the time compared to being convenient as reflected in the respective proportions [49 (38.3%) versus 79 (61.7%)] and [22 (24.4%) versus 68 (75.6%)] (Crude OR 1.92; 95% CI: 1.01-3.65; ÷2 = 3.99; p = 0.045). On the other hand, a significantly higher number of caregivers for orphans in Makulubita sub-county as opposed to the control sub-county opted for the healthcare action of their choice because it was perceived to be cheap at the time compared to having no money at all as reflected in the respective proportions [79 (62.7%) versus 49 (38.3%)] and [16 (33.6%) versus 39 (64.4%)] (Crude OR 2.92; 95% CI: 1.36-6.31; ÷2 = 8.18; p = 0.005). In the control sub-county alone, most caregivers for both non-orphans and orphans opted for the healthcare action of their choice because it was perceived to be cheap at the time compared to the extent to which health workers were perceived to be `understanding' as reflected in the respective proportions [67 (97.7%) versus 2 (2.3%)] for non-orphans and [116 (83.1%) versus 10 (16.9%)] for orphans (Crude OR 6.84; 95% CI: 1.32-47.35; ÷2 = 5.83; p = 0.016). Concerning the final outcome of the action taken for orphan and non-orphan's sickness, there were no significant differences in the two sub-counties. However, a significantly higher number of caregivers for orphans in Makulubita sub-county as opposed to the control sub-county reported having completely healed compared to those that were still sick but getting better as reflected in the respective proportions [78 (69.1%) versus 35 (30.9%)] and [84 (56%) versus 66 (44%)] (Crude OR 1.75; 95% CI: 1.02-3.02; ÷2 = 4.01; p = 0.043). Discussion In this study, we set out to compare healthcare dynamics between orphans and non-orphans in two sub-counties of Luwero district. Our findings are presented against a background of a package of AFXB's interventions consisting of developing IGAs (like poultry and piggery projects) for destitute families; providing beneficiaries with basic medical care for the treatment of AIDS-related opportunistic infections; providing beneficiaries with psychosocial support to help them cope with illness and to deal with stigma and discrimination; helping beneficiaries to develop professional skills through vocational training; providing educational support for children to pursue their education at primary and secondary levels; advocating for children's rights in the project's areas of operation; sensitizing beneficiaries about issues pertaining to HIV prevention, children's rights, nutrition, sanitation and environmental promotion; empowering youth by imparting HIV-related information and encouraging them to become peer-educators; actively contributing to the fight against HIV and AIDS; and creating support groups through which beneficiaries would be encouraged to help each other and manage collective activities17, 18. Over a period of two weeks preceding the study, no major significant differences were found in healthcare dynamics, particularly in morbidity and health seeking behaviour between orphans and non-orphans in the NGO-supported and control sub-counties. This is consistent with past literature 19, 20. It seems that even when the African extended family system is slowly but surely getting perforated 21, it is still managing to take care of orphans. Whether among the cases or controls, there was no blatant expression of fear, stigmatization, and discrimination in the way orphans were being looked after, a finding that contrast with research from Malawi that reported orphan abuse and discrimination in some homes 22. It is possible that orphan abuse and discrimination are a perception by orphans who misconstrue being parented by caregivers as exploitative. The reality maybe that orphans and non-orphans in rural communities are parented in a similar way. However, there were subtle differences in healthcare dynamics in different strata of study participants notably; common illnesses suffered from, action taken when a child, whether orphan or non-orphan would fall sick, days preceding action on the child's sickness, reason for the action taken and outcome of the action taken. On these parameters, the differences between orphans and non-orphans in Makulubita sub-county were even more subtle compared to Kamira sub-county, attesting to a probable positive role of the NGO in Makulubita. For instance, compared to fevers which were the commonest illness; bouts of diarrhoeal diseases and skin infections looked to have been fewer in Makulubita sub-county, where there was NGO support. However, the confidence intervals were too wide suggesting the need to be cautious in drawing incisive conclusions from such findings. The result could have been accidental given the small sample of orphans that had suffered from the two illnesses. Over all however, the nature of the subtle differences could have been an indication that the orphan problem is beginning to slowly but surely overwhelm the traditionally strong African extended family structures as has been suggested 23, 24. The role of NGO support in closing the welfare gaps in orphan care cannot be underestimated and has been reported elsewhere to be very important 25. Our findings suggest that when orphans fell sick in Makulubita sub-county where the NGO was supporting home-based orphan support programmes like IGAs, basic medical care, psychosocial support, vocational training; educational support, and promotion of children's rights; there was a higher likelihood of consulting village clinics instead of home-based herbal medication. This may be explained by uptake of educational massages concerning equity, compassion and support in looking after children, notwithstanding their status, that was often preached by the NGOs in her areas of operation. Secondly, the NGO support was likely to have provided health education about care for both orphaned and non-orphaned children. On the other hand, a significant majority of caregivers for orphans compared to those for non-orphans in Kamira, the control sub-county tended to take orphans under their care to village clinics as opposed to hospitals and health centres, implying an extent of discrimination in decision-making about source of healthcare. Orphans in the control sub-county which had no orphan-supporting NGO were less likely to be seen by health workers in hospitals and government health centres whose competencies are in most cases better. Furthermore, caregivers in Makulubita sub-county took fewer days to seek healthcare for non-orphans and orphans, an indication that the massage in the NGO's interventions about early response to ill-health for all children had been internalised. A significantly higher number of caregivers for orphans in the Makulubita sub-county as opposed to the control sub-county reported that orphans had completely recovered from illness that they suffered from two weeks before this study compared to those that were still sick. This research had its weaknesses which include; relatively small samples and use of self-report measures. The information on healthcare dynamics of orphans and non-orphans was for instance self-reported by caregivers and may thus have been compromised by recall bias. However, this study is still important because it examined an NGO intervention that attempts to foster even-handedness in childcare, between orphans and non-orphaned children. Future research could help a lot by conducting larger randomized trials and looking at more outcome measures. Secondly, this was a cross-sectional study which only suggests the likelihood of relationships between the studied variables. There are possibilities of threats to validity and reliability of the study findings because specific questions to investigate all the differences between orphans in the two sub-counties were not included in the research instrument. However, one probable explanation is the role of the NGO in Maukulubita sub-county. The strength of the study is that the focus was on specific dynamics of health care as indicators of wellbeing. On the contrary, many studies have examined orphanhood by primarily focusing on educational outcomes. In conclusion, the study has shown a lack of systematic difference in health outcomes between orphans and non-orphans, with a few exceptions. Secondly, the support rendered by the NGO in Makulubita sub-county stands out to be critical in cultivating even-handedness, compassion and non-discrimination in orphan care. It is rational to conclude that the insignificant differences between orphans and non-orphans in Makulubita sub-county maybe attributed to the work of AFXB. Secondly, the extended family system was found to still be managing to care for orphans, as elsewhere in Africa. However, the extended family was beginning to display cracks in support which has been reported elsewhere21, 26. Acknowledgements This study was funded by USAID though the Applied Research on Child Health (ARCH) Project of Boston University Centre for International Health, Massachusetts, USA. It was done in collaboration with Association Francois-Xavier Bagnoud (AFXB), a Switzerlandbased international NGO with a presence in Uganda. We thank the children, parents/caregivers, community guides and research assistants all of whom participated in this research to make it successful. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09019t1.jpg] [hs09019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}