 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 130-136 CD4+ lymphocyte values and trends in individuals infected with Human Immunodeficiency Virus and/or co-infected with Hepatitis C Virus in The Gambia Mboto CI1, Davies-Russell A 2, Fielder M2, *Jewell AP3 1. Royal Victoria Hospital, Banjul, The Gambia Code Number: hs09031 AbstractObjectives: This study was undertaken to monitor the CD4+ lymphocyte count in individuals infected with
Human Immunodeficiency Virus (HIV) and/or co-infected with Hepatitis C Virus (HCV) and to compare this with the counts
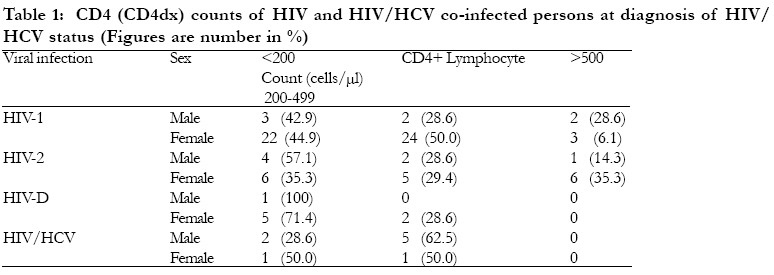
in normal individuals in The Gambia. Short title: CD4+ counts in HIV/HCV co-infection Keywords: HIV, HCV, co-infection, CD4+ lymphocyte, West Africa Introduction Measuring the CD4+ lymphocytes count remains the most effective means of evaluating of the clinical prognosis of patients infected with Human Immunodeficiency Virus (HIV)1. This measurement has been universally accepted as a uniform means for the clinical staging of patients infected with HIV and those progressing to AIDS2 and for the determination of the commencement of anti-retroviral therapy and for monitoring response to it3. Racial differences in the rate of CD4+ lymphocyte decline in HIV infected men have been reported4. Such differences have not been reported in HIV-2 or HIV2/HCV co-infected persons. Studies of the trends in the CD4+ lymphocyte count of HIV and HIV/HCV infected patients among different demographic groups can provide insight into the natural history of HIV1,5 and HIV/HCV co-infection6,7 and potentially influence the development of effective intervention programmes. However, few data are available on the CD4+ lymphocyte values of HIV infected or apparently healthy persons in most developing countries. In The Gambia, there is a paucity of information on CD4+ lymphocyte counts in the healthy Gambian population for establishing a normal reference value. The present study which forms part of work carried out on HIV and HCV co-infection in the Gambia was aimed at obtaining base-line data of CD4+ counts in apparently healthy individuals (pregnant women and blood donors) and those infected with HIV and/or Hepatitis C virus and to monitor trends in these groups. MethodsStudy population and sample collection A total of 1500 people age 11 months to 76 years referred for HIV serology at the Royal Victoria Teaching Hospital, Banjul, The Gambia between the months of July and December 2002 were counseled on a one to one basis. Following informed consent, 10 ml of venous blood was drawn from each participant. Samples from pregnant women were collected during their registration visit to the antenatal clinic irrespective of their trimester of pregnancy. 2 ml of each blood sample was dispensed into an EDTA container for CD4+ count. The remaining was centrifuged and the serum separated and frozen in two aliquots. One aliquot was preserved at 20oC for short-term use and the other at 70oC. No patient was aware of his HIV status prior to the visit to the hospital. Data on patient's demographic characteristics and behavioural factors were obtained in a one to one personal interview. HIV Serology Stored sera were screened every two weeks for HIV antibodies using Enzyme linked immunosorbent assay (ELISA) (8) kits Murex HIV1,2,0 (Murex Biotech, UK) following the manufacturers instruction. All samples reactive to Murex HIV-1.2, 0 were further tested using PEPTI-LAV 1-2 (Sanofi, France) for confirmation of the presence of antibodies to HIV and for differentiation into subtypes following the manufacturer's instructions. Samples reactive to Murex HIV 1, 2, 0 but un-reactive to PEPTI- LAV 1-2 were considered non-reactive. Those reactive to Murex HIV 1,2,0 and reactive to PEPTI LAV 1-2 either on the HIV-1 band or HIV-2 band or on both bands were confirmed to have antibodies against HIV. The test was repeated for all the samples reactive to Murex HIV 1, 2, 0. HCV serology Ortho HCV Version 3.0 Enzyme Immunoassay (EIA) Test Kit (Ortho Clinical Diagnostics, USA) was employed for the detection of anti-HCV. HCV Screening was carried out in batches on weekly basis or within 10 days of collection using refrigerated aliquots. The test procedures recommended by the manufacturers was adhered to. CD4 enumeration The CD4+ count of every sample collected was determined using the immunomagnetic cell isolation method (Dynal A. S., Oslo, Norway) within four hours of collection following the manufacturer's instruction. The CD4 count taken at the diagnosis of the individual HIV/HCV state was defined as CD4dx. The principle of the test is based on the coating of Dynalbeads with monoclonal antibodies, which serves as a solid phase for the direct isolation of CD4+ lymphocytes from blood. Accurate measurement is facilitated by the ability of Dynalbeads CD14 and Neodymium-iron-boron magnet (MPC-Q) to deplete monocytes, which may also express CD4+ antigen. Statistical analyses of data Chi-square and Fisher exact tests were employed to test the association between variables, while simple and multiple regression analysis were used to examine the influence of selected covariates on CD4+ lymphocyte counts. ResultsDemographic Characteristics of participants The participants were aged 11 months to 76 years and all had no previous knowledge of their HIV or HCV status. There overall mean age was 30.2 years; 31.9 years for the males and 28.7 years for females. Females accounted for 61.9 percent (928/1500) of the participants, while males accounted for 38.1 % (572/1500) of the participants. Over 70 percent (693/928) of the female participants were antenatal cases. Other participants include blood donors (30.7%, 460/1500), in and out patients with varying diagnoses (19.3%, 290/1500), people attending family planning clinic (1.9%, 28/1500) and medical examination for employment and educational purposes (1.9%, 29/1500). Identification of Case and control groups A total of 101 HIV infected patients were detected, of whom 9 were co-infected with HCV, and 22 patients were infected with HCV alone. The remainders were both HIV and HCV seronegative. A summary of the CD4 count of these patients in relation to their HIV and HCV status is presented in table 1 below. These patients formed the basis for the selection of the case and control groups. Category 1 (HIV seropositive subjects) This group was made up of all the anti-HIV seropositive persons. Nine were co-infected with HCV and were classified under a different category; four were lost to follow-up and one declined follow-up after post-test counseling. The remaining eighty-seven patients were listed for participation in this category. The details of the 87 patients were as follows: 72 females including 49 HIV-1 infected with an age range of 3 years to 47 years (mean age-26.5 years), 17 HIV-2 infected patients with an age range of 20- 26 years (mean age-28.6 years) and 6 infected with HIV-1 and HIV-2 (HIV-D) aged 16-36 years (mean age-24.9 years). Fifteen males included seven HIV-1 patients with an age range of 19-67 years (mean age-35.1), seven infected with HIV-2, ranging from 20-58 years in age (mean age 35.3 years and a 67 years old man infected with HIV-1 and HIV-2 (HIV-D). Category 2 (HIV and HCV coinfected persons) The second group were patients with HIV and HCV co-infection, seven men in the age range of 26 58 years (Mean age: 39.1 years) and two women aged 32 and 33 years (Mean age- 31.5 years). Six of the men had HIV-1/HCV co-infection and one HIV-2/HCV co-infection. Two women, one in her second trimester of pregnancy as per time of enrolment had HIV-1 and HCV co-infection and the other, a full-time housewife, had HIV-2/HCV co-infection. Category 3 (Negative control group) The third group consists of a total of 288 persons enrolled as a negative group. This group was made up of 222 women confirmed as HIV and HCV seronegative and selected on basis of age to match the 72 HIV positive women, 66 men confirmed as HIV and HCV seronegative selected on basis of age to match the 22 HIV positive men. Follow-up study Follow-up blood samples were collected every six months from all cases and control subjects who kept the appointment. Thus a total of three samples were collected from each participant in the months of June 2003, December 2003 and June 2004. Participants who did not keep the appointment within one month of the schedule date were excluded from further participation. Similarly participants with counts below 250 cells/µl were referred for antiretroviral therapy (ART) and excluded from the programme. The test procedures for the follow-up CD4 count, HIV and HCV tests were the same as previously enumerated. CD4+ lymphocyte count trends in HIV1 Infected patients The mean CD4+ lymphocyte count of males and females as per the diagnoses of their HIV status was 375 cells/µl and 291 cells/µl respectively. Only 4 out of the 7 men (57.1%) and 25(51.0%) women participated in the first round of the followup test six months later. The mean CD4+ lymphocyte count for the 4 male participants was 464 cells/µl and 339 cells/µl for the 25 females. During the second round of the follow-up test 12 months later only three males (42.9%) and 18(36.3%) females participated. The mean CD4+ count of these was 328 cells/ and 303 cells/ for male and females respectively. There was a 29.3% and 10.6% decline in the mean CD4+ count of the male and female participants over the 6-month interval. Similarly, the last round of the follow-up test had only 2 male and 10 female participants and their mean CD4+ count was 316 cells/µl and 285 cells/µl for male and females respectively. The cumulative decline in CD4+ of the participants who fully completed the programme was 43.2% and 44.4% for male versus female respectively. A highly significant (p<0.0001) was found between CD4dx and the declining CD4 trends when CD4dx was regressed against, the first, second and third CD4 counts however, no such association was found between CD4 counts and age or sex due in large part to the small number of participants who completed the programme. CD4+ trends in HIV 2 infected persons Unlike in HIV 1 infection the means CD4+dx count for HIV 2 infected females were comparatively higher than their male counterparts (354 cells/µl versus 287 cells/µl) at the time of diagnosis. The 3 males and 10 females who participated in the first round of the follow-up test after the withdrawal of participants with counts of below 250 cells/µl had a mean count of 345 cells/µl and 403 cells/µl respectively. The second round of the follow up test had one male and seven female's participants. The mean CD4+ count of the female participants was 400 cells/µl. The last round of follow-up test had a total of six participants made up of five females and a male. The mean CD4+ count of the females was 355 cells/µl. The rate of decline in CD4+ lymphocyte among HIV-2 infected males was slower than their HIV- 1 counterparts; however, this difference was not consistent among the females. There was a highly significant association between CD4dx and the decline in CD4 counts, however, this association was not found for age and sex due in large part to the small number of participants who completed the programme. CD4+ trends in HIV-D infected patients The mean CD4+ count of all the HIV-D infected persons as per the time of diagnosis of their HIV status was 232 cells/µl. The three participants in the first round of the follow-up test had a mean count of 242 cells/µl. The only participant in the second and final rounds of the follow-up tests had a count of 398 cells/µl and 258 cells/µl cells respectively, showing 35.2% decline in CD4+ count in an interval of 6 months. There was a highly significant association between CD4dx and the decline in CD4 counts, however, this association was not found for age and sex due in large part to the small number of participants who completed the programme. CD4+ trends in HIV/HCV co-infected persons The mean CD4+ count for the HIV/HCV participants as per the time of diagnosis of their status was 306 cells/µl while the HIV-2 /HCV participant had a mean count of 365 cells/µl . The first round of the follow-up had only 6 participants. This comprised of 4 HIV-1/HCV and two HIV-2/HCV participants with a mean count of 320 cells/µl and 297 cells/µl respectively. The second and final follow-up tests had only two male participants who were HIV-1/HCV infected their mean CD4+ count was 272 cells/µl and 171 cells/µl respectively sharing a decline of 37.1%. No HCV seroconversion was recorded among the participants throughout the follow-up period. CD4+ lymphocyte trend among HIV and HCV seronegative control subject The mean CD4 lymphocyte count of the 222 female participants as per the time of diagnosis of their HIV and HCV status was 496 cells/ µl. Their mean age was 28.6 years. The 220 participants who were tested during the first round of the follow-up test had a mean count of 503 cells/µl The second round had 216 participants who recorded a mean count of 499 cells/µl revealing a 0.8% decrease in count while the last round of the follow up test had only 214 participants with a mean CD4 count of 491 cells/µl showing a downward decline of 0.2%. This declining trend in CD4 was statistically significant. The 66 male control groups had a mean age of 35.8 as per the time of enrolment and a mean CD4+ count of 489 cells/ µl. The first follow-up test had 66 participants with a mean count of 492. The second and final follow-up test had 60 participants with a mean count of 509 and 513 cells/µl respectively. The counts showed a 3.5% and 0.8% increase in CD4+ count after 6 months and 12 months intervals. This trend in CD4 was not statistically significant. HIV-seroconversion Four cases of HIV seroconversion was recorded among the 288 negative control subjects. There were made up of 3 women and a man. These persons were excluded from further participation in the study. No HCV seroconversion was recorded among all the control participants throughout the duration of the follow-up test period. Discussion The finding of a comparatively higher number of females than males infected with HIV at a younger age than their male counterparts in this study is line with the epidemiology of HIV in most sub-Sahara Africa countries 9. This pattern has been attributed to the predominantly heterosexual mode of transmission of the virus in the region10,11 The mean CD4+ determined among the adult male and female HIV and HCV seronegative persons employed as control groups in this study is within the globally acceptable range12 ; however, this rate is comparatively below that reported for Caucasians. Several studies emanating from non- Caucasians population have reported similar lower CD4 count than reported for Caucasians 13. This finding makes the need for the employment of the CD4 of the Gambian population as a yardstick for the clinical staging and evaluation of her HIV/AIDS patients. The finding of a comparatively larger population of HIV 1 infected woman presented with a lower CD4+ count their male counterparts, while HIV-2 infected females had a higher count the males as per the time of diagnosis of their HIV status of in this study cannot be fully explained. Kilaru et al, 14 in a study conducted in Barbados found a comparatively higher proportion of women infected with HIV with a higher level of CD4 count as per the time of the diagnosis of their HIV status than their male counter parts. Generally, women are associated with higher CD4+ counts than their male counterparts and sex differences in the decline in CD4+ count has not been found to be influenced by gender, except during the close to the AIDS phase when the decline become enhanced in men15. Although in this study this difference was not significant statistically (p>0.05) it could be due to the stage of infection of the participants or other inherent factors such as environment, race among others that influences CD4 count16. The finding in this study of a persistent decline in the CD4 count of apparently healthy (HIV and HCV seronegative) women over the 18 months period is unclear. Although the rate of decline was quite low it was statistically significant and was not seen among the males. A possible explanation for this is that in addition to the numerous factors which may influence CD4 count17 most especially among women, the duration of the follow-up period was probably too short for a coherent conclusion to be made. Furthermore, more than 90% of the women employed as control group in this study were either pregnant women or lactating mothers. The contributing role of reproductive hormones such as chorionic gonadotropin (CG), estradiol and progesterone, and their physiological combinations which are expressed during pregnancy and postpartum period on CD4 count have not been evaluated in this study. Little or no data exist on the influence of reproductive hormones on CD4 count in apparently healthy women. The few available studies have focused on HIV-infected with varying findings18,19 . There is therefore need for a more elaborate longitidutinal study employing a cohort of pregnant and non-pregnant women to validify this finding. In this study, the rate of decline in CD4+ varied proportionally according to the type of HIV infection. Although this variation was not significantly associated with the type of HIV, the finding of persons with HIV and HCV coinfection with the highest level of decline within the 18 months period as compared to persons infected with HIV alone and HIV-D infected person with a higher decline than HIV1 or HIV-2 infected persons may be suggestive of the degree of severity associated with these infections20,21 . Some studies have advanced reasons for the accelerated HCV progression in HIV coinfected persons. One study showed HIV/HCV coinfected persons with CD4 count of less than 500 cells/µl had less immune response to HCV compared to persons with counts greater than 500 cells/µl, while individuals with count less than 200 cells/µl had worse response20. In this study no individual coinfected with HIV and HCV had a CD4 count above 500 cells/µl at diagnosis (CD4dx). CD4+ decline was progressively higher in HIV-1/HCV infected individual than in HIV-2/HCV infected person. Similarly the rate of decline was higher in coinfected individuals than in persons infected with HIV or HCV alone however; these differences did not reach statistical significance. The accelerated decline in CD4 count observed in these individuals as compared to those infected with HIV or HCV alone may therefore be line with these reports. This assertion is further supported by studies that provided evidence of less stimulation of CD8 HCV cells that target HCV thus contributing to quicker HCV progression in HIV infected individuals. This finding underscores the need for early diagnosis of people at risk of HIV/HCV coinfection and supports reports suggesting the commencement of therapy at a comparatively higher CD4 count than in coinfected persons. Conclusions and Recommendations This study revealed that more women than men were proportionately infected with HIV at a comparatively lower age than the men and that this sex and age differences was significant. The determined CD4 count of apparently healthy Gambian male and female's was 489 cells/µl and 496 cells/µl respectively. This rates, though lower than that reported for Caucasians is within the normal range. It also shows that the mean CD4+ count as per time of the diagnosis of the HIV status of the participants was 375 cells/µl and 291 cells/µl respectively for HIV 1 infected male and female participants and 354 cells/µl versus 287 cells/µl for male and female HIV 2 infected participants. While participants infected with HIV D had a mean count of 232 cells/µl, while HIV and HCV co-infected persons who were predominantly males had counts of 306 cells/µl as per the time of diagnosis of their status. The study reveals a more gradual decline in CD4+ among the females than the males. This study revealed that the CD4+ count of infected persons was directly proportional to the severity of type of HIV infections, while a significant progressive decline in CD4 count was observed among the female control group. This finding is unclear and calls for a longitudinal study involving a cohort of pregnant and non- pregnant women. These observations have important implications in clinical staging and management of HIV/AIDS in the Gambia. Acknowledgement CM is particularly grateful to Dr Sam Omar, Director of Medical Services Department of State for health for approval of this work, the head of the Pathology department Mr. Jaye for permitting the use of laboratory facilities, Messer Emmanuel Ogenekun, Batchilly, Faal, Jobarteh, Daniel Eyam, who gave generously their time and Dr Mark Egbe for some reagents and material support. This work was partly supported by the University of Calabar, Calabar-Nigeria research grant, and Community Health Organization financial aid. In addition, CM is grateful to the University of Calabar for the release to undertake this study. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09031t1.jpg] |
| |||||||||

{kind=link}