 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 137-142 Rapid screening for co-infection of HIV and HCV in pregnant women in Benin City, Edo State, Nigeria Duru MU1,2, Aluyi HSA1,3, *Anukam KC3,4 1. Department of Microbiology, Faculty of Science, University of Benin Code Number: hs09032 Abstract Background: Human Immunodeficiency virus (HIV) and Hepatitis C virus (HCV) are both major global health
concerns as they cause high mortality and morbidity in the developing countries. However, while data exists for the co-infection
in other countries, little or no information can be found with regard to the sero-prevalence of HIV and HCV co-infection
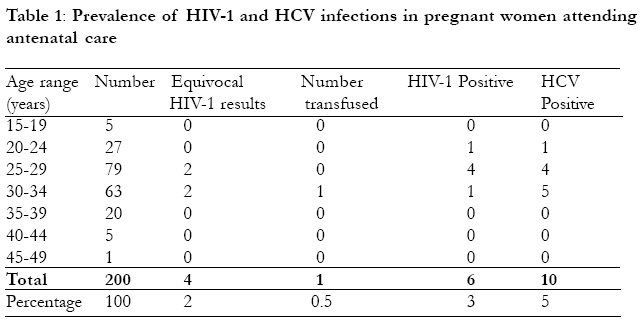
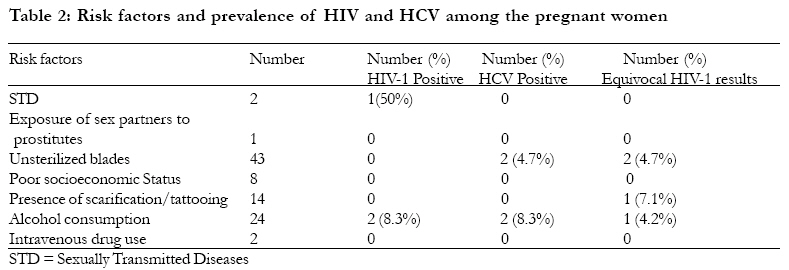
in Nigeria, albeit in pregnant women attending antenatal care clinics in Benin City, Nigeria. Key words: HIV, HCV, co-infection, prevalence, pregnant women Introduction Epidemiological studies have demonstrated that Human immunodeficiency virus (HIV) and Hepatitis C virus (HCV) co-infection is becoming increasingly recognized world wide because of the similarities in the mode of transmission 1. A recent Austrian study that used polymerase chain reaction technique showed that 10% of HCV infected mothers who were HCV RNA positive during pregnancy were HIV-1 infected2. In respect of vertical transmission of HIV from infected mothers to the child, Robert and Yeung3 showed that HCV co-infection increases the rate by 4 to 5 fold. Factors responsible for increased risk of vertical transmission include among others, concomitant HIV infection with HCV and a high maternal viral load4. The prevalence of each of these infections has been documented among pregnant women in Africa, Europe and America. In the Democratic Republic of Congo, HCV among pregnant women was found to be 4.3%5, in Egypt it has been shown to be 19%6. The prevalence of HCV infection among pregnant women in Europe is generally below 2%7. The World Health organization estimated in 1997 that about 3% of the world has been infected, with Africa having a prevalence rate as high as 10%, in the USA 1.8% and in Japan 0.8%8. The sero-prevalence of HIV among pregnant women in the developed countries is usually lower than that of developing countries. In Australia, seroprevalence of HIV in antenatal women is 0.23 per 10009. In Amsterdam it is 0.26%10. In Zambia, the prevalence of HIV in pregnant women is 29% 11, while in Rwanda, it stood at 16%12. More disturbingly, the prevalence of HIV among pregnant women in Botswana remains at 45%, while in Nigeria, the most populous country in Africa, the HIV prevalence among pregnant women is 5.6% as at 2004 sentinel report13. However, while prevalence of either HIV or HCV has been chronicled among pregnant women in different parts of the world, little information exist for the prevalence of HIV and HCV co-infection among pregnant women in Nigeria. Therefore we hypothesize that HIV and HCV co-infection may be present in pregnant women seeking antenatal care in Benin City. The objectives of this study were to determine the sero-prevalence of HIV and HCV co-infection and to examine the risk factors that may lead to acquisition of both infections in pregnant women attending antenatal care clinic in Benin City, Nigeria. Materials and Methods Study design and Subjects Two hundred pregnant women (15-49 years) attending antenatal care clinic at Faith Medical Centre Benin City between April 2003 and March 2004 were enrolled in the study. The subjects were verbally informed of the study and consent was granted. Closed ended structured questionnaires were used to obtain personal data such as age, marital status and possible risk factors to route of transmission of HIV and HCV. For the risk factors, participants were asked to indicate whether they have had any history of previous blood transfusion, tattooing/scarification marks, history of sexual exposure to multiple sex partners, past history of sexually transmitted diseases, intravenous drug abuse. The socio-economic status was determined by asking the women to indicate the range of their house-hold annual income. Women indicating less than hundred thousand Naira (N100, 000.00) per annum, were taken as `poor' economic status. Respondents stating between 100,000.00 and N250,000.00 represented `average' and those indicating N250,000.00 and above represented `above average'. The Human Ethics Review Board at the study site gave approval for the study. All testing was voluntary and included pre- and post counseling by trained HIV counselors. Patient's selection and Collection of samples: Demographic data were collected using a non-probability convenient sampling technique. For emphasis, convenience sampling is a technique often used in face-to-face interview as in this study. A convenience sample is when the interviewer simply approaches any pregnant women seeking antenatal care at Faith Mediplex and asking her to participate in the study. Clinical nurse practitioner was designated for approaching potential volunteers and seeking their consent during clinic days. Blood samples (5ml) were collected into a plain container from each respondent. The blood samples were allowed to clot and then spun in a bucket centrifuge at 10,000xg for 10 minutes. The serum was stored at 4oC and prior to each test, the sample was allowed to attain room temperature of between 26oC and 28oC. Anti-HCV detection test: Clinotech anti-HCV (Clinotech diagnostics, Richmond, Canada) and Acon anti-HCV (Acon Laboratories, San Diego, California, USA) detection test kits were used in accordance with the manufacturer's instructions. The anti-HCV is based on the principle of double antigen sandwich immunoassay, in which purified recombinant antigens are employed sufficiently to identify anti-HCV with high specificity and sensitivity. Detection of Antibodies against HIV The Hexagon HIV kit (Human, Weisbaden, Germany) and HIV rapid test strips (Acon Laboratories, San Diego, California, USA) which is a third generation test based on immuno-chromatogenic technique was used to test for both HIV-1 and HIV-2. The procedures were followed in accordance with the manufacturer's instructions. Statistical method A sample size of 200 pregnant women within the study period was found to be statistically robust, as Faith Mediplex is a Christian evangelical hospital that record up to 2000 pregnant women in a year. Therefore at 80% statistical power with 0.05 alpha error (95% confidence level), 200 women from this population was found to be statistically representative. Nonparametric statistical method, Chi-Square (÷2) was employed to test the association of the risk factors to HCV and HIV and P value less than 0.05 was taken to be significance. Results The non-probability convenient sampling techniques employed for this study yielded 800 pregnant women attending antenatal care clinic that were approached, of which 200 voluntarily agreed to participate. The result of the rapid screening showed that seventy nine (39.5%) of the respondents belonged to the age group 25-29 years, followed by 63 (31.5%) in the age group of 30-34 years. Age group 20-24 had 27 (13.5%) women, while 35-39 years had 20 (10%). Age groups 15-19 and 40-44 had 5 (2.5%) pregnant women each. The women in the age group 45-49 had the lowest (0.5%) rate of pregnancy (Table 1). On history of blood transfusion, 14 (7%) respondents admitted having received blood transfusion at a certain time in their lives. Two (1%) pregnant women (30-34 age group) had history of drug abuse. Two women have had STD previously, one belonging to the age group 20-24 years, while the other in the age group 25-29 tested positive for HIV-1. Fifty six (28%) respondents admitted having had occasion when unsterilized blades were used on their bodies. A total of 26 (13%) women reported alcohol consumption, while 15 (7.5%) admitted presence of scarification marks/tattooing on their bodies. One (0.5%) pregnant respondent admitted having been exposed to a female prostitute. On the economic status of the women based on the earnings per annum of the house-hold, 8 (4%) indicated they were poor as they indicated earning less than N100,000.00 per annum and 173 (86.5%) stated being on the average economic side of living, while 19 (9.5%) admitted being above average in terms of their house-hold earning per annum. Table 2 shows incidence of HIV and HCV in the study sample. The rapid screening for HIV indicated that six (3%) women were HIV-1 positive. Four HIV-1 positive occurred in the age group 25-29 years showing 5.1% prevalence. Age groups, 20-24 and 30-34 had one woman positive for HIV-1 and this represented 3.7% and 1.6% seroprevalence of HIV respectively. None of the six HIV-1 positive pregnant women had been transfused previously. There were 4 (2%) equivocal (indeterminate) HIV results, two occurring in the age groups 25-29 and 30-34 years. One of the equivocal HIV results has been transfused previously. Equivocal HIV result is an unsure result, in that the same sample was positive for one of the kits and negative in another test kit and vice versa. There was no HIV-2 positive result in this study. Ten (5%) women were positive for HCV as obtained with the rapid screening test kit, with the highest number of 5 (7.9%) occurring in the age group 30-34 years. Two women that were positive for HIV-1 were equally infected (co-infected) with HCV infection. This represents 33% co-infection with HIV-1. In terms of the various occupational groups among the pregnant women, unemployed women had HIV-1 prevalence of 4.3%, while public servants had 12.5% prevalence. On HCV prevalence, traders (business) had 2.7%. Unemployed, fashion designers and public servants had 3.5%, 27.2%, and 28% respectively. Other risk factors as shown in Table 2, in relation to HIV prevalence were found in women (50%) with a history of STD for the past six months, and alcohol intake (8.3%). Alcohol intake and use of unsterilized blades had 8.3% and 4.7% prevalence respectively in HCV positive pregnant women. There was a 33% HIV-1 positive in HCV positive pregnant women. There was no significant association between HCV positivity and HIV at P value 0.05 (÷2=0.52, P=0.4704). Discussion This is probably the first study on the prevalence of HCV and HIV-1 co-infection among pregnant women attending antenatal care clinic in Benin City Nigeria. Although not statistically significant, a 33% co-infection was noted in this study and it should be noted with astuteness that the kits used were not confirmatory. The percentage was high when compared with the United Kingdom14 and Austrian studies2, having 1.7% and 10% co-infection respectively. The reason for this may have been due to the fact that confirmatory test such as nucleic acid test for HCV RNA or Recombinant immunoblot assay (RIBA) was not used to confirm all reactive samples following rapid screening. Studies conducted earlier, depending on the risk group (not pregnant) being described, have reported 50 to 90% of HIV-1 positive individuals being co-infected with HCV15. The co-infection of HIV-1 and HCV noted in this study is very important for several reasons, bearing in mind that there is a possibility of mother-to-child and female-to-male transmission of HCV. The management of the two infections is quite different and some studies have established that HIV co-infection accelerates the progression of HCV infection and vice-versa16,17. In this study where all the women `supposedly' have a stable relationship with their partners, sexual intercourse may be the main means of transmission as some reports have shown that sexual intercourse may transmit HCV18. One report has established that even casual contact among members of the same household19 can transmit HCV. The 5% prevalence of HCV in the pregnant women sampled did not show any association for previous blood transfusion, although only one HCV positive woman had a history of blood transfusion. This value was lower compared with the previous work of Halim and Ajayi20 that reported a12.3% HCV prevalence among volunteer blood donors in Nigeria. As regards risk of transfusion-transmitted hepatitis C virus, two separate studies have found that 3% and 0.5% of blood transfused in a tertiary hospital in Benin City, and Portharcourt, Nigeria were infected with HCV 25, 26.The 3% prevalence of HIV among the pregnant women studied could be very significant. In Nigeria, with about 25% of the African population, a recent national HIV prevalence sentinel survey by the Federal Ministry of health showed that the number of people living with HIV/AIDS in 2003 was between 3.2 and 3.8 million13. According to the report, the age group 20-24 years had the highest national prevalence of 5.6 per cent, and the HIV prevalence for women aged 15-24 years remains 5.2 per cent. Recently, the United Nations AIDS program (UNAIDS) estimated that around 22 million people around the world have died from AIDS, and about 40 million more are currently infected with the virus. Sub-Saharan Africa has been hit hardest by the pandemic: about 83% (18.26 million) of AIDS deaths and 71% (28.4million) of HIV infections have occurred in some war-ravaged, poverty stricken part of the continent. In some African nations, over 30% of the adult population is HIV-positive21. With the co-infection of HIV and HCV, the impact on the female population could be grim, where over 7,000 women become infected each day21. In sub-Saharan Africa, around one quarter of females under the age of 30 have HIV and an estimated half billion are at risk of acquiring the virus through sexual contact21. Efforts to provide condoms, develop a vaccine, use spermicides or anti-retrovirals, have failed to stem the epidemic. HIV-HCV co-infection is a problem of considerable proportion as 1 in 10, of those infected with HIV globally are also infected with HCV 22. Nowicki et al.23, showed that HCV RNA can be detected in almost 30% of HCV-HIV-1 co-infected women and that viral diversity does exist between local HCV and plasma HCV extracted from HCV-HIV-1 co-infected women. In a similar study in Burkina Faso 24 utilizing the HCV-RNA nucleic assay, only 1.3% of pregnant women attending antenatal care clinic were co-infected contrary to our finding. Conclusion In conclusion, in this scenario, routine screening for HIV and HCV for all antenatal patients should be included in the clinical practice guidelines for clinicians in Nigeria as 33% of co-infection was noted among HIV positive pregnant women. However further studies are needed to decipher the prevalence of co-infection of HIV-HCV among pregnant by using molecular techniques such as polymerase chain reaction (PCR) or nucleic acid methods for confirmation of the two infections. Although the risk factors were not statistically significant to HIV/HCV co-infection as shown in this study, however, public health education is highly needed to highlight the dangers of co-infections of HIV and HCV. Early diagnosis of the co-infections may lead to prompt intervention management towards reducing the vertical transmission of both infections. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09032t2.jpg] [hs09032t1.jpg] |
| |||||||||

{kind=link}
{kind=link}