 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 147-152 Predictors of smoking initiation among schoolchildren in Tunisia: a 4 years cohort study *Harrabi I1, Chahed H1; Maatoug J1, Gaha J1, Essoussi S2, Ghannem H1, 1. Service of Epidemiology and Biostatistics University Hospital Farhat Hached, Sousse, Tunisia Code Number: hs09034 Abstract Objective: To identify predictors of smoking initiation among non smoking Tunisian school children; and
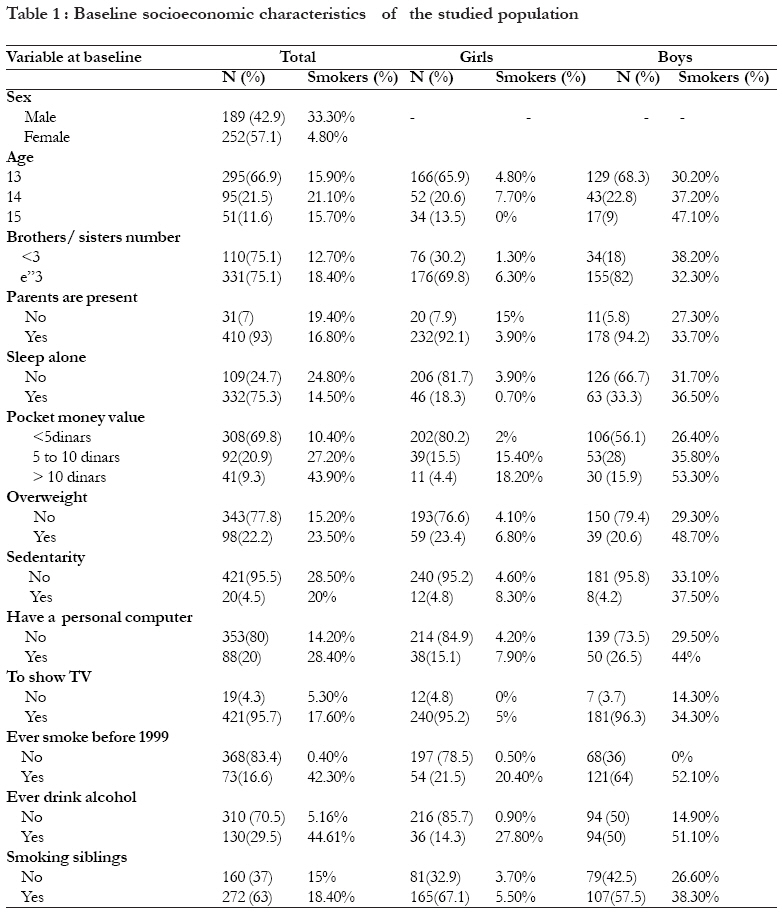
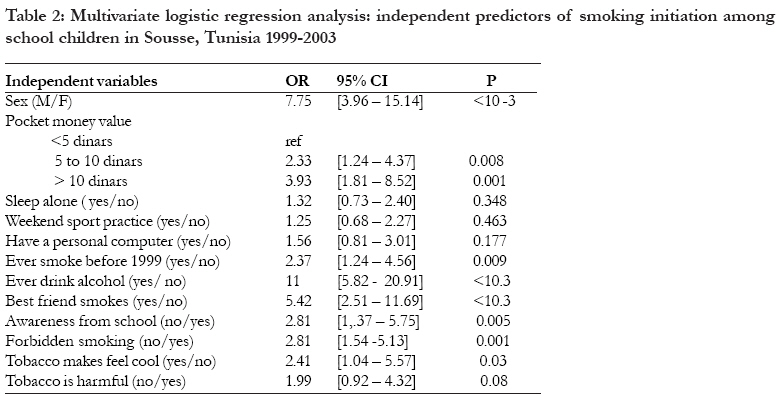
to propose efficient antismoking strategies in order to prevent smoking initiation. Key words: Epidemiology, smoking initiation, adolescent, follow- up study Introduction Smoking is one of the leading public health problems worldwide1. According to the world health organisation, tobacco use, known as the first cause of preventable death and associated to cancer, cardiovascular and lung diseases2; caused 4 million deaths in the year 2000. This figure is expected to rise to 10 millions by the year 2030, as tobacco use spreads (particularly in the developing countries) 3,4. In fact, according to the FAO report, total cigarette consumption increased in developing countries by 3.7 percent per annum, a rate almost ten times higher than that of developed countries. Moreover, world cigarette production increased from 3 million tonnes in 1970 to 5.6 million tonnes in 2000 due to increasing production in developing countries. However, in developed countries, cigarette production shows only a small increase from 2 million tonnes in 1971 to 2.5 million tonnes in 19915 . In 1996, Peto et al estimated that unless current trends changed, some 30-40% of the 2.3 billion children and teenagers in the world would become smokers in early adult life and about 250 million of these future smokers will die because of smoking6. Effective measures, adopted in developed countries to limit the spread of smoking, have proved to make a difference by reducing, or at least slowing the increase in tobacco use: Prevalence of smoking adults has decreased7. However the smoking rate among teenagers remains high without any sign of decrease8,9,10. Manufacturers have benefited from the globalization of trade, creating big increases in domestic tobacco consumption and imports of tobacco products in many developing nations3. Worldwide, the tobacco industry spends tens of billions of dollars a year on marketing. The global tobacco industry now exploits the developing world by lobbying tactics perfected in the developed world including pressuring governments to block marketing restrictions and tax increases11. In Tunisia, tobacco use is a well established behaviour. In fact, smoking prevalence among adults was estimated at 30.4% in 1996, 55.6% among men versus 5.2% among women12. Adolescent smoking prevalence was estimated at 12.1% (21.3% among boys versus 3.3% among girls) (13); age of initiation was estimated at 15 years old14. Unfortunately, no prospective study was conducted to analyse the evolution of Tunisian teens' smoking behaviour, attitudes and knowledge. These study objectives were to identify factors that lead Tunisian school children to start smoking and to propose efficient antismoking strategies in order to prevent smoking initiation and to build tobacco control coalitions. MethodsPopulation and study design It is a cohort study surveying, prospectively for 4 years, 453 students attending schools in Sousse city. Baseline data were obtained as a part of a randomised investigation about the cardiovascular diseases risk factors among 13-15 year old pupils attending schools in Sousse city (Tunisia) in 1999. The total initial number of students was 789. After four years (2003), the questionnaire was filled in by pupils present in their classrooms at that day. Among those who completed the questionnaire in 2003, there were 453 pupils who had already completed the questionnaire in 1999. There was no statistical difference between the baseline population characteristics and the cohort population reviewed in 2003. Non smokers were pupils who didn't smoke even a cigarette during the last year. Those who had smoked at least some puffs were considered as smokers. Our interest was in those who were not smokers in 1999. They represented 441 pupils. Data collection Data were collected anonymously by a self administrated questionnaire during a class session with the collaboration of teachers and parents. This survey assessed: socioeconomic characteristics, smokers in the pupil's household and at school, alcohol consumption, past experimentation with tobacco before 1999, attitude toward smoking, knowledge about harmful effects of tobacco.None of the pupils explicitly refused to participate in this survey. Statistical analysis Data were analysed using the SPSS software. The÷ 2 statistic or t tests were used as appropriate. Statistical significance was determined at the p< 0.05 level throughout. A univariate and multivariate logistic regression models were used to identify baseline predictor variables for smoking status over the four years follow up. The dependent variable was to be smokers in 2003. Results Demographic data: Our study population was composed of 441 pupils aged between 13 and 15 years old (57.1% were girls, 42.9% were boys). All of them were initially not smokers in 1999. 75.1% had more than three brothers and sisters. The majority (93%) were living in an intact nuclear family where both parents were present. Less than 40% of these pupils had both working parents. More than 75% had an individual bedroom. 4.5% were sedentary; 95.7% watched TV daily whereas only 20% had a PC at home. Before 1999, 16.6% have already tried to smoke; 29.5% have already started drinking alcohol.63% of these students had at least one of their siblings who smoked as shown in table 1. Smoking status In 2003, smokers prevalence was 17% (4.8% of girls, 33.3% of boys; p< 10-3). The mean of tobacco consumption was 2. 51 (+/- 0. 99 SD) cigarette per day. Over 69, 9% of these adolescents who started smoking in 2003, declared that they would remain smokers in the following 5 years (72.1% of smoking boys, 58.3% of smoking girls; p= 0. 34). Regular smokers represented 22.7% (16.7% of girls, 61.3% of boys; p= 0.005). Predictors of smoking initiation Based on the univariate analysis, thirteen potential predictors of smoking initiation were retained for multivariate analysis. In Table 2, we reported the independent factors that remained significantly associated with smoking initiation in multivariate analysis. Predictors of smoking were: sex, pocket money value, previous experience with alcohol and tobacco, having a smoking best friend, lack of sensitization from the part of school, believing that smoking makes one feel cool and that tobacco shouldn't be forbidden in public places. Neither family nor teacher smoking nor mass media influence was significantly associated with smoking initiation adjusted on age and gender. This was the first reported study in the Tunisian context that tried to describe the smoking initiation process in a sample of Tunisian pupils. We found that sex, pocket money value, alcohol use, past experience with tobacco, having a best friend smoker, lack of sensitization from school, thinking that smoking made one feel cool and that tobacco should be forbidden in public places, were highly associated with smoking initiation in our study. Some limitations of this study should be considered. First, short intervals between waves should be employed in longitudinal studies on adolescent behaviours such as tobacco initiation15. Second, all measurements were self reported meaning that information bias could have occurred. Some studies suggest that adolescents who smoke appear to deny this, even when biochemical measures classify them as smokers. We have remade such insufficiency in our study by optimised measurement conditions and ensuring anonymity. Smoking initiation occurs habitually during adolescence16,17. It becomes an established behaviour as initiation age is earlier18,19. Several predictors identified in others studies conducted in developed countries, seemed to enhance the likelihood of initiating smoking in these countries15,17,19,20,21,22. Predictive factors of smoking initiation, identified in the current report, have been reported and well documented in previous studies such as alcohol consumption7, having a best friend smoker21,23,24,29 and lack of sensitization from school19. In fact, alcohol consumption was usually associated with smoking initiation7,19. However numerous studies suggested that tobacco use usually preceded alcohol consumption25 and that nicotine may facilitate the addictive effects of other substances such as alcohol26. Furthermore, peers who exhibited risk behaviour such as drinking and smoking were likely to influence each another to engage in that behaviour: initiating smoking accelerated more rapidly among pupils whose best friend smoked because throughout adolescence, youngsters experience feelings of uncertainty about self-image and see themselves very much in the eyes of their peers. Therefore associating with friends will be easier when one's behaviours are congruent with others. These findings suggest providing young peoples with skills to resist peers prompts to adopt health risk behaviour such as tobacco and alcohol consumption by encouraging teens to avoid high risk peers and environments. On the other hand, our study tried to identify predictors of smoking initiation specific to our socioeconomic condition and our beliefs.Contrary to most studies conducted in developed countries, smoking initiation rate was higher among boys than girls. This difference is probably related to our Arabic social norms that accept such deviant behaviour from a boy and consider it as a sign of rebelliousness and of transition to adult life, whereas girls who smoke are considered as promiscuous and liberated ladies. Furthermore, pocket money value was identified as an important predictor of smoking. In fact rich pupils were more likely to start smoking because they had an easier financial access to tobacco. Finally, lack of awareness about hazard effect of smoking from school and believing that tobacco should not be forbidden in public places were also associated with a higher risk of smoking initiation. Through these findings, we conclude as in other studies that school is an important source of information about harmful effects of smoking19. Moreover, restriction of smoking in major public places shows teenagers that being non smoker is the normal and the referential adult attitude. Other variables such as having smokers in the family, teacher smoking, sensitization about hazard effect of smoking from the family or mass media were not shown to have a significant association with smoking initiation in our study. Conclusion In conclusion and through our findings, multilevel influences on youth smoking behavior had been identified. Thus, anti-tobacco interventions should address the problem at all levels: the individual, the family, the social environment and through legislation policies. Intervention programs should target young children to avoid experiencing the first cigarette during pre-adolescence19,29. According to Nebot M et al, intention to smoke in the future increased significantly the risk of later smoking initiation30. Thus providing young people with skills to resist smoking can be efficiently achieved through a multidisciplinary management including community and school based intervention highlighted by mass media campaigns. Several studies had shown, prospectively, a durable reduction of smoking and more sensitization about hazard effect of smoking while such strategy was adopted27,28. Moreover Adolescents' current smoking and future smoking expectations are linked to marketing exposure even in limited settings, suggesting the need for comprehensive controls to eliminate the function of marketing in promoting adolescent. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09034t2.jpg] [hs09034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}