 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 179-185 A re-appraisal of Warfarin control in the treatment of Deep Vein Thrombosis and / or Pulmonary Embolism *Amiwero C1, Campbell IA2, Prescott RJ3 1-Federal Medical Centre, Department of Haematology and Blood Transfusion, Bida, Niger state, Nigeria. Code Number: hs09040 Abstract Background: Warfarin is commonly used for management of deep vein thrombosis (DVT) and
pulmonary embolism (PE), controlling therapy by means of the International Normalized Ratio (INR). Running head: Warfarin Control in treatment of DVT/PE Key words: Deep vein thrombosis; Haemorrhage; International normalized ratio; Pulmonary embolism; Thromboembolism; Warfarin. Introduction Deep vein thrombosis (DVT) and / or pulmonary embolism (PE) are the two major manifestations of venous thromboembolism. The incidence of DVT in the United Kingdom is one to two people per 1,000 per year1. Over the past decade, there has been an extraordinary increase in the use of warfarin in the UK: about 470,000 patients were estimated to have received an oral anticoagulant in 2001 with the figure expected to rise because of the increasing older population1. In the year 2004, an estimated 2 million N. Americans developed DVT, with more than 600,000 also experiencing PE2. Warfarin is the oral anticoagulant prescribed to this steadily increasing number of patients to control and prevent thromboembolic disorders. However, its complex doseresponse relationship and the narrow therapeutic range, coupled with the potentially life threatening effects of both under dosing and overdosing, necessitate close monitoring of the actual degree of anticoagulation, especially to balance the risk of excessive bleeding3. The incidence of bleeding following warfarin therapy varies from country to country. In the United Kingdom, the annual rate of fatal bleeds was reported as 0.6 per 100 patients4. The overall incidence of first time idiopathic bleeding was 15.2 per 100 patient-years. The incidence of fatal and/or hospitalized and referral was 3.5 and 2.6 per 100 patient-years respectively4. The annual rate of major bleeding ranges from 0.9 to 2.7 percent whilst the median annual rate of fatal bleeding ranges from 0.07 to 0.7 percent in the United States5. The target levels of warfarin therapy are disease specific. A target therapeutic INR of 2.0 and 3.0 has long been considered as the safest range for DVT/PE. Achieving this range necessitates frequent monitoring and dose adjustment to prevent fatal consequences of haemorrhages and recurrent venous thrombosis/pulmonary embolism from either over or under anticoagulation. Based on this narrow therapeutic range, values below 2.0 and above 3.0 are considered risks for thrombosis and bleeding respectively6, 7. Wilson et al.8, in a randomized trial, classified INR values as "High Risk" when the values were <1.5 or >5.0 although the justification for this choice was not stated. Previous studies have tried to examine the relationship between different anticoagulant intensity and complications of bleeding and / or recurrent thromboembolism1, 9, 10, 11. However, direct application of the results of these studies is limited by the populations on which they were conducted, groups of patients with conditions other than DVT/PE. Between September 1999 and December 2002, the Research Committee of the British Thoracic Society (BTS) conducted a randomized, controlled trial looking at the outcomes (fatal and non fatal) in patients with DVT/PE who were treated with warfarin for either 3 months or 6 months, following initial heparin. The major efficacy outcome variable in the trial was failure of resolution during treatment and / or recurrent thromboembolism during or after treatment, with major and minor haemorrhages among these subjects being the main adverse events. The trial did not show a statistically significant difference between the two periods of anticoagulation with respect to the major efficacy outcome variable, but haemorrhages were more common in the 6 months' group. Although INR levels were recorded, these were not analyzed in detail in relation to outcome12. In view of the above findings, this nested case-control study, was focused on subjects who developed the complications of failure of resolution and / or recurrent thromboembolism or of haemorrhages, with the aim of identifying differences in the pattern of INR levels between thrombotic cases and controls and between haemorrhagic cases and controls.
Methods In the BTS trial, 746 patients were randomised to 3 months' or 6 months' treatment with warfarin, having met the following inclusion/exclusion criteria:
Inclusion criteria Aged 18 years or more, suspected or proven DVT and / or PE, whom the clinician intended to anticoagulate.
Exclusion criteria PE deemed so severe by the clinician as to require thrombolysis or pulmonary embolectomy. Neoplasia diagnosed and/or requiring treatment within the previous three years. Pregnancy. PE in the preceding three years. Known polycythaemia, thrombocythaemia, antithrombin III deficiency. Lupus anticoagulant, homozygous Factor V Leiden, Protein C or Protein S deficiency or other similar predisposing haematological disorders. Any condition which would result in prolonged or continuous immobility or confinement to bed e.g. advanced multiple sclerosis/or orthopaedic problems of the lower limbs. Previous allergy to heparin or warfarin. Requirement for long-term anticoagulant therapy Inability to give informed consent, Clinicians were asked to start warfarin on day one of the scheduled five days of heparin treatment, usually with low molecular weight heparin Data for the BTS trial were collected via standardized clinical research forms completed prior to randomization and at 3, 6 and 12 months post randomization. The forms contained questions about demographic characteristics, some clinical details e.g. diagnosis, investigations, date of starting warfarin, haemorrhagic or thrombotic complications, and INR results. INRs were used to monitor anticoagulation with warfarin according to a standardised protocol which was circulated to the participating physicians. The aim was to achieve INRs between 2 and 3.5. This case-control study, however, is focused on warfarin control based on the pattern of the INR in patients either discovered to have developed haemorrhage or to have failure of resolution while on treatment and / or recurrent thromboembolism during or after treatment, together with matched controls. It is important to state here that only INR measurements before a complication were utilised in the analysis In the study design, two, nested, case-control designs were used. One case-control study involved those with failure of resolution and / or recurrent thromboembolism whilst the other involved those with haemorrhages. The sample size was determined by the number of complications observed in the trial and power calculations were not relevant. The adequacy or limitation of the sample sizes is demonstrated by the width of the confidence intervals that are reported.
Study population and data extraction To achieve matching of cases and controls, the study database was sorted by age, sex, underlying cause and the randomised duration of warfarin. Cases were identified and matched to an adjoining control with the above variables. The INR data of the cases and controls were then manually extracted from the corresponding clinical research forms. Some subjects were found to have INR data missing. Cases without INR data were dropped from further consideration, together with their matched controls. Controls without INR data were replaced with the next available subject from the sorted database.
Statistical Analysis As the INR data were positively skewed, a logarithmic transformation was used to normalise the data. The data were summarised by the use of descriptive statistics to describe all subjects with regard to age, sex, diagnosis and the underlying cause and to obtain confidence intervals where appropriate for the continuous variables e.g. percentages of INR within and out of range and the geometric mean and the standard deviation of an individual's INR values. The continuous variables were compared between cases and controls using paired t-test or the non-parametric Wilcoxon signed rank sum test, as appropriate. All data analysis was carried out using the Statistical Package for the Social Sciences Version 14 (SPSS v. 14).
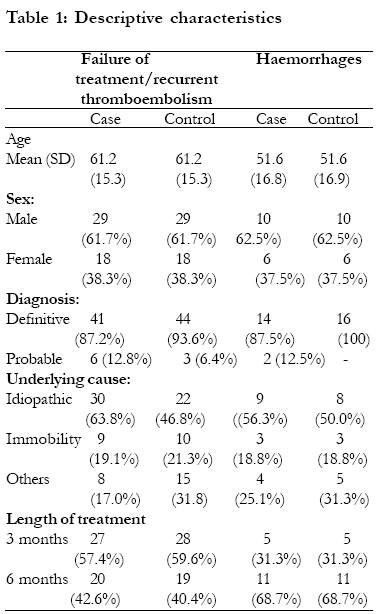
Results A total of 80 cases, along with their paired controls, was identified, consisting of twenty subjects with haemorrhages and sixty subjects with failure of treatment and / or recurrent thromboembolism. Missing INR data reduced this to 63 cases and 63 matched controls, of whom 16 patients had haemorrhagic complications and 47 patients had failed to resolve on treatment or had recurrent thromboembolism. The characteristics of the study subjects are summarized in table 1. The average age of cases with failure of resolution/recurrent thromboembolism was 61.2 (SD15.3) years whilst in cases with haemorrhages the average age was 51.6 (SD 16.8) years. The sex distribution was similar in both sub-studies, 62% being male. The geometric mean INR of subjects with failure of resolution and/or recurrent thromboembolism was 2.20 (95% C L, 2.10 to 2.29), vs. 2.30 (95% CL, 2.18 to 2.43) in the controls; ratio 0.96, 95% C.L 0.90 to 1.01, P = 0.12. In the subjects with haemorrhagic complications, the geometric mean INR was 2.14 (95% CL, 1.95 to 2.36), vs. 2.31 (95% CL, 2.12 to 2.52) in the controls; ratio 0.93, 95% C.L 0.82 to 1.05, P = 0.22. For both haemorrhage and recurrences, the ratio of the geometric means of cases and controls was therefore not statistically significant.
Percentage in therapeutic range In the analysis comparing the level of warfarin control in terms of the percentage of INRs within the usual therapeutic range of 2-3 in subjects with failure of resolution and / or recurrent thromboembolism, there was no statistically significant difference between cases and controls: the mean percent in range in cases was 56.5% (95% C.L. 50.3% to 62.8%), vs. 56.1% (95% C.L. 49.7% to 62.6%) in the controls; (P = 0.93). Similarly, the percentage of INRs above the therapeutic range was 12.8% (95% C.L. 8.8% to 16.9%) in cases, vs. 16.8% (95% C.L. 12.1% to 21.6%) in the controls; (P = 0.09). However, the percentage of INRs within range differs between cases with haemorrhage and their control group: the mean percent within range among cases was 43.0% (95% C.L. 33.3% to 52.7%), vs. 61.5% (95% C.L. 52.8% to 70.2%) in the controls; (P = 0.01). There was no significant difference between the two groups in the analysis of mean percentages of INR values above the range; cases 10.5% (95% C.L.3.6 to 17.3), vs. 12.1% (95% C.L. 4.8 to 19.4) in the controls; (P = 0.74). Correspondingly an excess of those with INR levels below the therapeutic range was seen in patients with haemorrhages (46.6% [95% C.L. 33.8% to 59.4%] compared to controls (26.4% [95% C.L. 17.7% to 35.3%]; P = 0.03).
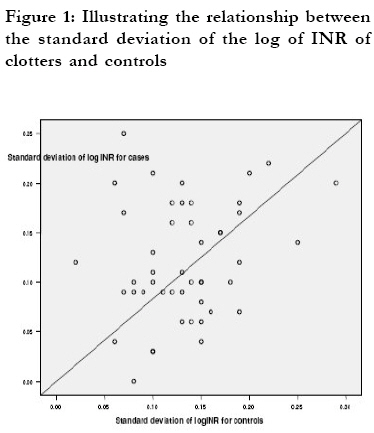
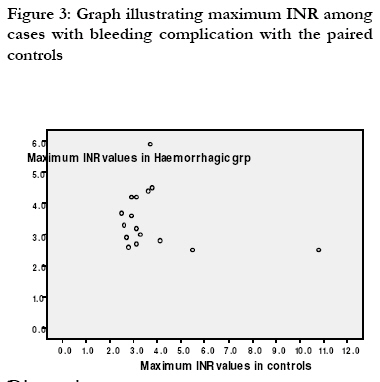
Pattern of standard deviation among cases and controls The difference in the mean standard deviation of log INR values among the subjects with failure of resolution/recurrent thromboembolism and controls was not statistically significant (0.12 [95% C.L. 0.10 to 0.14] vs. 0.13 [95% C.L. 0.12 to 0.15]; P = 0.25) as shown in Figure 1 below. The difference in the mean standard deviation of log INR values among the haemorrhagic subjects and controls was also not statistically significant (0.12 [95% C.L. 0.09 to 0.14] vs. 0.12 [95% C.L. 0.09 to 0.15]; P = 0.95) as shown in Figure 2. Maximum INR values among subjects with haemorrhages and paired controls The maximum INRs were similar in both groups as shown in Figure 3. However, more of the control subjects (12.5%) had INR values > 4.5 compared to the haemorrhagic group (6.3%), although this difference between the two groups was not statistically significant by the Wilcoxon signed rank sum test (P = 0.45). Discussion International Normalized Ratio has long been used to control the intensity of warfarin therapy for various thromboembolic conditions including DVT and / or PE. Traditionally, INR values in the range of 2.0-3.0 are considered as the optimum therapeutic range for the prevention of haemorrhage, failure of resolution and recurrent thromboembolism during oral anticoagulation management of DVT and / or PE. According to Wilson et al.8, INR values consistently below 1.5 are a risk factor for the re-occurrence of thromboembolism whilst INR values above 5.0 are a risk for haemorrhages7. In support of this report is the earlier finding by Berwaerts et al.11, of the danger associated with values of INR above 4.5, especially in terms of haemorrhagic complications, although they emphasised the fact that sub-therapeutic INR values cannot be considered to be entirely safe in protecting against intracranial haemorrhages. In this study, High Risk INRs were not generally observed either among cases with failure of resolution and / or recurrent thromboembolism or haemorrhagic complications. Unequivocally most of the subjects in this study had INR values within the standard therapeutic range of 2.0-3.0. The geometric means of subjects with failure of resolution / recurrent thromboembolism was 2.2 vs. 2.3 in the controls and 2.1 vs. 2.3 for those with haemorrhages and controls respectively. The geometric means for cases did not differ significantly from the control groups although the values in both sets of controls were higher than in the cases. Haemorrhagic complications occurring within the therapeutic range are not uncommon, especially among patients with other co-morbidities e.g. gastrointestinal lesions, urinary tract infections, thrombocytopaenias, anaemia, renal insufficiency etc. This fact, combined with the finding of higher INR values among the controls, suggests that higher INRs were unlikely to have been responsible for the occurrence of haemorrhages in this study. A similar case-control study conducted by Fang et al.9, found that most cases (62%) of intracranial haemorrhages among patients with atrial fibrillation occurred at INR below 3.0 although the results did support the finding of previous studies that an increase of intracranial haemorrhages was associated with higher INR values. In the current study, only one case of subarachnoid haemorrhage was found among the DVT and/or PE subjects. Other types of haemorrhages ranged from menorrhagia to gastrointestinal bleeding. In terms of the level of warfarin control, the mean percentage of INRs within range was not different between thrombotic patients and controls: 56.5% vs. 56.1% (P = 0.93). This finding is different from the expected one of better anticoagulation among the controls as opposed to those with thrombotic complications. However, expected results were seen among the haemorrhagic group and paired controls in the sense that warfarin control was relatively better in the control group when compared to the haemorrhagic cases, (61.5% vs. 43.0%),this difference between the two groups being statistically significant (P = 0.01). If there were to be an increased bleeding risk at higher INR levels, one would expect more of the observations from cases to be above the therapeutic range but the reverse was observed. The percentage value above the range was higher in the controls (12.1%) than those with haemorrhagic complications (10.5%), leaving an excess of INR readings below the therapeutic range in those with haemorrhage. Further to this, the results of the maximal INR values among haemorrhagic cases and controls were similar although, again more of the control subjects had INR values above 4.5. It is important to note here that in one particular subject among the control group, INR values ranging from 4.6 to 10.8 were recorded. In terms of the standard deviation of the INR values, there was no statistically significant difference between cases and controls. The overall results in this study raise the possibility that it may be possible to raise the target range for INR without an excessive risk of accompanying haemorrhage. However, this finding is in contrast to the report of an observational study of Barclay and Vega et al 10, who found that the risk of major bleeding decreased from 3.6 per 100 patient-years in patients with high intensity warfarin treatment to 2.7 per 100 patient-years in patients with low intensity warfarin treatment. This observation, however, was made among patients with atrial fibrillation who are more at risk of bleeding complications than those with DVT and / or PE. This study is limited by a number of factors: the small sample size, especially among the haemorrhagic groups of subjects. A total number of eighty cases along with their paired controls were identified and they consisted of twenty subjects with haemorrhages and sixty subjects with failure of treatment and / or recurrent thromboembolism. During subsequent compilation, some cases and controls were discovered to have missing INR values. Cases with missing INR values were dropped from the analysis, while controls with missing INR values were replaced with the next matched. At the end of the above processes, the initial sample number of eighty cases and paired controls had reduced to sixty three cases / paired controls. The small sample size makes it difficult to make a firm conclusion from the findings in this study. We note though that the 95% confidence limits for the ratio of mean INRs in haemorrhagic cases and controls rules out INR levels being more than 5% higher in those with haemorrhage. Also, lack of information regarding the dose of warfarin, administered concomitant drugs and co-morbid conditions, limits the possibility of allowing for confounders. However, this study was on information collected by the Research Committee of the BTS in their prospective, randomized trial in which data were recorded in a standard way at set intervals. Such information can be adjudged to be of good quality. The inclusion / exclusion criteria in the BTS study allowed the recruitment of a broad range of patients drawn from all over the UK and managed within the National Health Service. The exclusion criteria were confined to those for whom treatment for 3 or 6 months with warfarin was unlikely to be efficacious or safe. The findings of this study will therefore apply to a substantial proportion of patients presenting with DVT and/or PE. Care has to be taken not to extrapolate these findings to the categories of patients who have been excluded, with those with recent neoplasia being the most important such group.We note that the geometric means in this study were in the lower part of the therapeutic range of 2.0-3.0 even though the BTS therapeutic guideline in the trial was 2.0 to 3.5. Therefore the findings support the idea of raising the upper limit of the present narrow therapeutic range of 2.0-3.0 to at least 3.5, if not higher. A corresponding rise in the lower limit to 2.5 might also be considered so that levels of anticoagulation that may be more effective in treating and preventing the recurrence of thromboembolism are achieved in practice.
Conclusion The pattern of INR values examined among DVT and / or PE subjects with complications of failure of resolution/recurrent thromboembolism and haemorrhages, revealed that the overall geometric means, as well as the percentage of INR above the range, were higher among the control groups compared to the cases. This suggests that raising the upper limit of the therapeutic range of 3.0 to 3.5, as in the BTS study and also raising the lower limit to 2.5 might possibly be an option for the treatment of DVT/PE, which would not incur an excessive risk of accompanying haemorrhage. This suggestion thus allows for a more liberal but yet concise use of warfarin therapy. Close monitoring remains essential for those subjects with co-existing morbidities, who are the group most likely to bleed at any therapeutic INR range. Further randomized control trials are needed to refine the optimal therapeutic range for INR level in the treatment of venous thromboembolism.
Acknowledgement We thank the Research Committee of the British Thoracic Society for allowing us to study results from the patients in their trial. We are grateful to Mrs Diane Wyatt for assisting with extracting and anonymising the necessary records of the patients included in our study.
References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09040t1.jpg] [hs09040f1.jpg] [hs09040f3.jpg] [hs09040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}