 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 3, Sept, 2009, pp. 201-205 Campylobacter spp among Children with acute diarrhea attending Mulago hospital in Kampala - Uganda *Mshana SE 1, 3, Joloba M 1, Kakooza A 2, Kaddu-Mulindwa D 1 1-Department of Medical Microbiology Makerere University College of Health Sciences, Kampala Uganda Code Number: hs09044 Abstract Background: Campylobacter infections occur worldwide. A recent study in Kampala, Uganda, found that 87% of
broiler chickens had Campylobacter jejuni; these are potential source of human
infection. Isolation rate in developing countries
is between 5-35%. This study aimed at finding prevalence of children with campylobacter
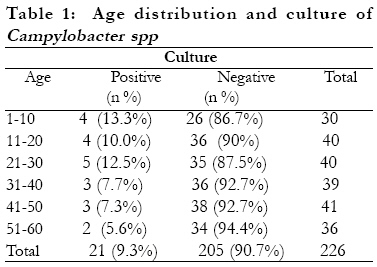
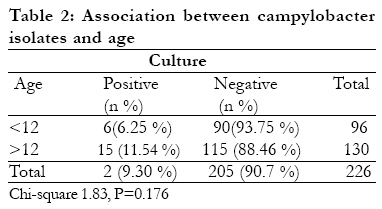
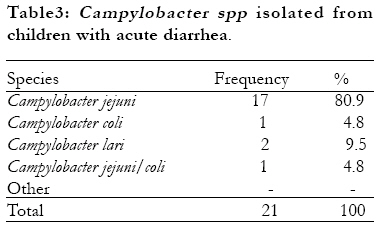
infection among children with acute diarrhea attending Mulago hospital. Keywords: Campylobacter spp, Prevalence, Acute diarrhea Introduction Campylobacter spp are frequent cause of enteritis infection in humans (1, 2). These organisms were first recognized as common human pathogen in 1970 and since that time their importance has increased and now they are considered to be one of the most frequent bacterial causes of enteritis (3, 4). The prevalence in developed countries range from 1-13% among children with acute diarrhea and 1.5% among children without diarrhea while in developing countries range from 5 - 35% (5, 6). Case community based studies in developing countries have provided an incidence estimate of 40,000 to 60,000 per 100,000 for children less than five years of age (3, 4) . Campylobacter is considered a potential etiological agent of bacterial enteritis both in children and young adults; it is the second in prevalence to Salmonella and nearly similar to Shigella (7, 8). The age group mainly affected by these organisms in developing countries is below 2 years of age. In developing countries, where campylobacter infection is hyperendemic, recurrent exposure to the organisms might lead to acquisition of humoral immunity, which can be demonstrated by progressive rise in specific IgA level with age (9). Thus even while the frequency of exposure is the same as in childhood, the rate of symptomatic infection is significantly lower (3). This might lead to isolation of the organism from healthy, asymptomatic persons, which is quite rare in developed countries (7). Poor hygiene and sanitation and close proximity to animals in developing countries all contribute easy and frequent acquisition of any enteric pathogen including Campylobacter spp and this is responsible for sporadic cases (10). Person to person transmission is uncommon (11). Overlap is reported between serotypes of C. jejuni found in human, poultry and cattle, indicating that foods of animal origin play a major role in transmitting C .jejuni to humans (12). Different animals have been found to be reservoirs of C. jejuni such as birds and rodents (13). The intestine of poultry are easily colonized with C. jejuni, a one-day-old chick can be colonized with as many as 35 organisms (14, 15) .In Uganda isolation rate in broiler is about 87% and in some farms 100% isolation rate has been found (16) . The aim of this study was to determine the proportion of Campylobacter spp infection among children with acute diarrhea and susceptibility pattern of these organisms in children with acute diarrhea. Material and Methods Study population: The study population included children from 1-60 months of age attending Mulago hospital with acute diarrhea. Diarrhea was considered if the child had passed three or more loose or watery stool in a 24 hrs period, prior to presentation. Study design: The study design was analytical cross sectional study from July to October 2005. Inclusion criteria: Children with acute diarrhea as defined by WHO. Children aged 1 month to 5 years (age limits are inclusive) with either bloody or non bloody diarrhea. Written signed consent from the parent/caretaker. Exclusion criteria: Children with an age of greater than 5 years or age below one month (age limits are exclusive), children with persistent diarrhea, no written or signed consent from parent/caretakers. Persistent diarrhea was defined as an episode that had exceeded two weeks (WHO). Sample size calculation: A formula of Kish and Lisle (1965) was used to calculate sample size. A proportion of 18% was used as p (5). Sampling method: A serial sampling method was used, about 7 -10 children were recruited every Monday, Wednesday and Friday until the sample size was reached. A simple questionnaire were filled for each patient, it included name, age, duration of diarrhea, antibiotic use and animals kept at home. Stool collection and analysis: Stool specimens were collected on the same day of enrollment using wide mouth screw cap sterile container (HIMedia laboratories Pvt. Limited, Mumbai, India). Specimens were sent to the laboratory for analysis on the same day; most of the specimens were analyzed within 3 hrs of collection. A loop full stool mucous part was picked and inoculated on blood free charcoal based selective media (CCDA) (BioMerieux, Paris, France) and Blood contained media selective for Campylobacter (BioMerieux, Paris, France) (17,18,19) . Incubation condition was at 37oC and 42oC for primary isolation in microaerophilic condition oxygen (5%), carbon dioxide (5-8%). Microaerophilic was achieved using Gas pack and 150 system anaerobic jars (BioMerieux, Paris, France). Plates were incubated for 48hrs in microaerophilic condition; typical colonies which are watery, spreading and convex were identified. The colonies with typical morphology were further identified using gram stain, catalase test, oxidase test, susceptibility to Nalidixic acid (30µg) (BioMerieux, Paris, France) and cephalothin (80µg) (BioMerieux, Paris, France) and Sodium hippurate hydrolysis (17, 18, 20). Disc susceptibility tests for ampicillin (10µg), erythromycin (15µg) and ciprofloxacin (5µg) (BioMerieux, Paris, France) were done using Muller- Hinton agar supplemented with 5% sheep blood. (HIMedia laboratories Pvt. Limited, Mumbai, India). Colonies from fresh culture were suspended in sterile distilled water and adjusted to 0.5 McFarland. Swab was dipped into suspension and was used to inoculate Muller Hinton Agar supplemented with 5% sheep blood. Incubation was done for 18-24hrs at 42oC. Streptococcus pneumoniae (ATCC 49619) was used for quality control of the media and discs. The inoculum was checked for contamination by inoculating the plate for pure culture. Interpretation was according to King and Huguette (21, 22). Data analysis: Data were entered in the computer, according to the codes given and analyzed using SPSS 10.0. The chi-square- test and Fisher exact tests were used to perform and establish any statistical difference. Results The study population was made up of 226 children with acute diarrhea of whom 130 (57%) were male and 96 (42.5%) were female. A total of 226 stool specimens were processed. Among 226 stool specimen cultured 21 (9.3%) were positive for Campylobacter spp in all age groups combined (95% confidence interval 5.5-13.1). The distribution of Campylobacter spp in various age groups is shown in table 1. The isolation rate was higher in the age group 1-10 which was 13.3% and least in age group 51-60 (5.6%) p=0.8. It was found that the proportion of children with positive culture in infants, children d"12 months, was 6.2% while those children above 12 months was 11.5%, chi square 1.83, p =0.176 seen in table 2. Three species of campylobacter were identified, (Campylobacter jejuni 17 (80.9%), Campylobacter lari 2 (9.5%) and Campylobacter coli 1 (4.8%)) among 21 isolates of campylobacter. In one isolate the discrimination between C. jejuni and C. coli was not possible because the isolate failed to grow on subsequent subcultures. The susceptibility pattern of the 20 isolates was determined by disc diffusion using standards set by King and Huguette. (21, 22) The rates of resistance to various antibiotics were erythromycin (0%), ampicillin (20%) and ciprofloxacin (5%). All resistance to ampicillin was of intermediate level. Discussion The study found the proportion of children with campylobacter infection among children with acute diarrhea to be 9.3%. This rate is comparable to the rate in developing countries ranges from 5-20 % (2). The rate in Uganda is comparable to the rate of Zimbabwe (9.3%), Egypt (9.0%) and Brazil (9.9%) (3). This rate is lower when compared to Tanzania (18%) and Kenya (11%) countries which boarder Uganda (5, 23). This can be explained by the fact that studies in Kenya and Tanzania were done in rural setting where people are living close proximity with animals hence facilitating transmission and use of antibiotics could have contributed to low isolation rate (p=0.04). In general the infection rate was high in children below two years (10.9%) compared to (8.5%) in those above two years. This has been found in other developing countries such as Nigeria, Tanzania, and Thailand (24). In this study the infection rate was decreasing with age as shown from the age of 2 years but the difference was not significant p=0.85. This can be explained by the fact that our study population was under five which can be equally affected. This has been found in developing countries in contrast to developed countries where even adults can have symptomatic infection with these organisms (6). Usually as the age increases, the level of antibody tends to increase; this is associated with future protection to infection. There was no difference between infection in infants and in children above 12 months of age, (p=0.176), this can be explained by the fact that our study population was in children 5 years and below, this age group is almost equally affected in developing countries (6) . Among 21 campylobacter isolates 17 (80.7%) were confirmed to be Campylobacter jejuni. This species is commonly associated with human infection due to Campylobacter spp and most of virulent factors explained to date are due to research in this specie. In this study all isolates were sensitive to erythromycin using disc susceptibility; thus differing from the study in Nigeria where 84 % were sensitive. This can be explained by the fact that resistance of campylobacter to macrolides, including erythromycin is resulting of inappropriate use these drugs in treating human infection rather than veterinary use. Resistance to erythromycin ranges from 0-16% has been seen in developing countries and is more common in Campylobacter coli than Campylobacter jejuni (3). In this study the use of erythromycin was very low; only 1.7% participants used it prior to visiting the hospital. The isolation rate of Campylobacter coli was also low in this study; this could partly explain why no isolate was found to be resistant to erythromycin (23). In this study 5% of campylobacter isolates were resistant to ciprofloxacin (5µg). This is very low compared to Thailand and Nigeria where resistance to ciprofloxacin increased from 0% to 84% (1991-1996) as result of inappropriate use of quinolones. Resistance to quinolones is contributed to by the indiscriminate use of drug before culture, use of quinolones accounted for 15% of resistant isolates during 1996-1998 (23). In this study, no child was treated with ciprofloxacin before culture and in one case (1.7%) nalidixic acid was used beforehand as treatment. Resistance to ampicillin was 20%. This was high compared to other antibiotics tested; this can be explained by high rate of using antibiotics related to ampicillin in the management of other correlated pediatric morbidities in the community. Campylobacter jejuni is prevalent in Kampala, Uganda, as in other developing countries. Erythromycin is still the drug of choice for campylobacter infection in Kampala- Uganda. A larger multicenter study should be undertaken so that the extent of campylobacter infection in our setting can be established. Acknowledgement We thank the staff of Microbiology Department and Pediatric Department for their cooperation. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09044t3.jpg] [hs09044t1.jpg] [hs09044t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}