 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, Special Issue 2, Oct, 2009, pp. S72-S80 Perceptions about human rights, sexual and reproductive health services by internally displaced persons in northern Uganda Orach CG1, Musoba N2, Byamukama N3, Mutambi R4, Aporomon JF1, Luyombo A5, Rostedt A6 1. Makerere University School of Public Health (MUSPH) Code Number: hs09050 Abstract Background About 1.6 million internally displaced persons (IDPs) from northern Uganda have been living in
encampments since the late 1980s. In conflict settings such as northern Uganda women are disproportionately affected compared to
men. This study explores women and men IDPs` perceptions of their access to information about rights, access to health
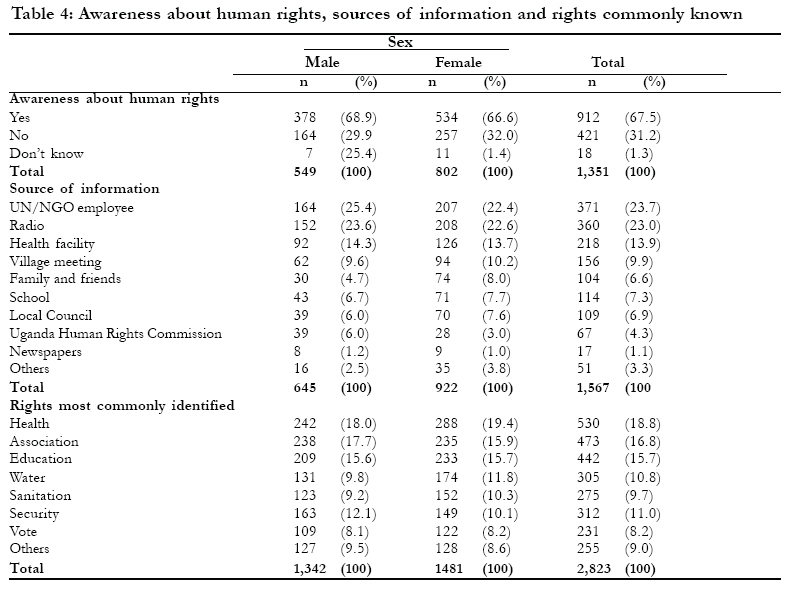
services and gender-based violence. Introduction Two decades of a protracted civil war between the Lord's Resistance Army (LRA) rebels and the government armed forces has led to the displacement of an estimated 1.6 million persons from northern and eastern Uganda. Most of the displaced originate from the Acholi sub-region which includes the districts of Gulu, Amuru, Kitgum and Pader that have borne the brunt of the war. During 2005 most of the populations of Pader and Kitgum districts were displaced (95% or 279,000 and 93% or 267,000 respectively). Three years later, most of the population in the districts of the Acholi sub-region still live in encampments.1-4 Across diverse types of crisis settings, the health of women and girls, men and boys is affected differently. Social, cultural and biological factors increase the risks faced by women and girls.5, 6 Women often face increased risk of violence and may be unable to access assistance and/or make their needs known. They are often not included in community consultation and decision-making processes and as a result, their health needs are often not met. Those delivering health care in crisis must take account of the different needs, recognise potential barriers and ensure that women and men can access health services equally. Women and men must participate equally in the planning, management and delivery of health services in humanitarian action, and women must be part of the decision-making and implementation processes at all levels. Uganda is a state party to various international and regional human rights instruments providing for the right to the highest attainable standard of health the right to health. The right to health is one of the fundamental human rights and there are many important linkages between the right to health and other human rights such as the right to food and the right to education. The United Nation (UN) Guiding Principles on Internal Displacement state: "at the minimum, regardless of the circumstances, and without discrimination, competent authorities shall provide internally displaced persons with and ensure safe access to essential food and potable water; basic shelter and housing; appropriate clothing; and essential medical services and sanitation." The right to health can be understood as a right to the enjoyment of a variety of facilities, goods, services and conditions necessary for the realization of the highest attainable standard of health. The right to health includes health services, goods and facilities to be available, accessible, acceptable and of good quality.7 It is interpreted as an inclusive right extending not only to timely and appropriate health care but also to the underlying determinants of health, such as access to safe and potable water and adequate sanitation, an adequate supply of safe food, nutrition and housing, occupational health, environmental conditions, and access to health-related education and information, including on sexual and reproductive health. A human rights-based approach to health emphasises that health interventions should further the realisation of the right to health and be guided by human rights standards and principles, including the principles of participation, accountability, non-discrimination, empowerment and local ownership. Health interventions should support the capacity of duty bearers (including state i.e. central and local governments and non-state actors i.e. international humanitarian agencies and civil society organizations) to meet their obligations and of rights-holders (i.e. community members including men and women, adults and children) to claim their rights. Health programmes can promote or violate human rights in the ways they are designed and implemented. Services must be designed to meet the needs of women and men equally.8 If community members are not aware of their rights and empowered to demand their rights, they will not be able to hold providers and authorities accountable. If interventions are formulated without the active and informed participation of those affected, they are unlikely to be effective and empowering. If health providers do not pay conscious attention to non-discrimination and gender issues, it is likely that services will not meet the needs of women and men equally. If health providers and authorities are not aware of human rights standards they are unlikely to ensure that human rights are respected in the health care setting. If community members are not given an opportunity to influence health interventions by sharing their views on the availability, accessibility, acceptability and quality of services, we may find disempowered communities instead of strong local ownership. In this study we explored the perceptions of internally displaced persons towards human rights and sexual and reproductive health services. Methods The study was carried out in Kitgum and Pader districts in northern Uganda. In 2007, there were an estimated 629, 617 internally displaced persons i.e. 310,111 IDPs in Kitgum and 319,506 in Pader districts respectively.9 The districts had a total of 67 IDP camps i.e. 24 camps in Kitgum and 43 in Pader respectively. This was a cross-sectional study comprised both of rights holders (i.e. internally displaced community members including adults and adolescents) and duty bearers responsible for services provision at the central and local district levels (including individuals and institutions such as ministry of health and local district health services providers and humanitarian relief i.e. UN agencies, international NGOs and community based organisations (CBOs)). We sampled 15 of 24 IDP camps (62.5%) in Kitgum district using purposive and random sampling techniques. The camps were stratified by parishes, population size, and security considerations and randomly selected. In Pader we selected 20 of 43 (46.5%) camps into the study. Administratively, a camp is sub-divided into blocks and zones. A block constituted a study cluster. We selected households based on the modified WHO Expanded Programme of Immunization cluster sampling technique.10 The centre of the cluster was identified. A bottle was spun to determine the initial direction of movement. A random starting household was identified by listing all households from the centre to the end of the cluster and a random starting household was chosen, and the next selected for interview was the nearest to the one where the interviewed had been conducted. In a household, either a male or female adult head of household was interviewed. We selected male or female respondents in the proportion of 40% to 60% respectively. However, after every third household, an adolescent aged between 14 and 19 years was identified and interviewed. A total of 51 respondents (adult/adolescent) were interviewed per cluster in Kitgum and 40 in Pader district. In total 1,383 individuals comprising 720 (52%) of respondents in Pader and 663 (48%) in Kitgum district were interviewed. We held 27 in-depth key informant interviews and conducted 52 focus group discussions. The key informants included camp commandants, and Local Council 1, 2 and 3 Chairpersons, in charge of health units including health centre II and III. In addition, leaders of community-based organisations (CBOs) were interviewed. At the district level, civic authorities including local council (LC V) chairpersons, resident district commissioners, chief administrative officers; and in the health sector, the district health team members such as the district health officer (DHO), medical superintendent, medical officers, the person in charge of the nurse training school (the matron), district health visitor, and personnel responsible for health centre IV were interviewed. Finally, we interviewed various humanitarian relief workers from agencies including United Nations High Commission for Human Rights (UNHCHR), United Nations Children's Fund (UNICEF), World Health Organization (WHO), and Non-Governmental Organisations as shown (in Table 1) below. The 27 in-depth key informant interviews were held with 14 staff from international and local humanitarian agencies (UN/NGO/CBOs), 8 with district health staff, and 5 with community and district civic leaders. We conducted a total of 52 focus group discussions (FGDs) (Table 2). The FGDs consisted of adult, adolescent, and community leader groups. Women and men were divided in both adult and adolescent FGDs. There were eight to ten persons per group. The discussions took about one hour each. The FGDs were taped recorded. More than half of the FGDs (28 of 52, or 52.8%), were carried out with adults (men and women), 16 of 52 (30.8%) with adolescents (males and females), and 7 of 52 (13.5%) with community leaders. We trained data collectors for three days. The study instruments (questionnaire, focus group, and key informant guides) were translated into the local language Luo/Acholi and back into English. The data collection tools were pre-tested. The quantitative data were captured, cleaned, and edited. The completed questionnaires were checked by the principal investigator daily for accuracy, completeness and consistency before the data collectors left the IDP study sites/camps. Quantitative data were checked for completeness, sorted, coded and captured using EPI data version 3.02 packages. The data were analyzed using SPSS version 12.00 software package. Qualitative data were analyzed manually. Content analysis was based on condensation and abstraction of main themes. Results As shown in Table 3, more than a quarter of the respondents 25.9% (25.7% males and 26.4% females) were between the ages of 14-19. Most adult respondents 61.4% (57.3% males and 64.2% females) were in the age group 20-49 years. 24.2% of respondents (9.1% males and a significantly higher proportion of females, 37.4%) had no formal education while 56.8% of respondents had attained at least primary level education. Most respondents 75.2% (73.9% males and 76.4% females) have lived in encampments for a period ranging between one and ten years. Two thirds (67.5%) of the respondents (males 69% and 67% females) mentioned that they are aware about human rights (see Table 4). The main sources of information are UN/NGOs 24%, radio 23% and health facility 14%. Of all the rights identified, the right to health was the most known (18.7%) followed by the right to freedom of association (16.8%) and the right to education (15.7%). The least known and or appreciated were security (11.0%) and voting (8.2%). Most (78%) respondents (79.5% in Kitgum and 76.5% in Pader) live within 5 km of a health facility (see Table 5). The main reasons for choice of a health facility are proximity to health facility 29.6% (males 29.1% and females 30.1%), availability of free treatment 22.7% (males 21.5% and females 23.9%); availability of drugs 17.2% (17.4% males and females 17.0%) and good quality services 11.4% (12.3% males and females 10.4%). Most respondents 87.3% (85.6% females and 88.9% males) mentioned a health facility as the choice for delivery, either for themselves or their wives (see Table 6). The main barriers women face in accessing health care services include lack of money 36.4% (34.9% male and reported by a higher proportion 37.9% female); lack of information 24.3% (25.3% males and 23.2% females) and lack of decision power mentioned by 17.5% (17.7% males and 17.3% females). However, as shown in table 6 above, several barriers to accessibility of health services were identified in government health facilities. These include generally late opening of health facilities (opening hours generally ranged from 10.00 am to 1.00 pm). In addition, there are few staff members. Sometimes there are only 2 personnel in a facility. Furthermore the supply of drugs was also reportedly inadequate. One key Informant mentioned Two thirds (64.9%) of the female respondents considered waiting time to be very long in the facilities. Overall, two thirds of both males and females attribute the long waiting time to the presence of many patients The health workers always tell us "Come tomorrow" So many people often go to get treatment in other health facilities - government or private like Meeting Point (a private clinic). Male Youth FGD. Paloga Camp, Kitgum DistrictMost respondents 72.7% (68.4% males and a higher proportion 77% of females) consider gender based violence to be common in the camps (see Table 7). The three most common interventions for management of gender based violence include treatment for physical injuries 33.9% (33.3% males and 34.5% females); testing and treatment for STIs 22.4% (22% of males and 22.8% females); and counselling 18.9% (19.4% males and 18.4% females). Discussion The high level of awareness about human rights issues in the emergency settings may be attributed to the involvement of UN agencies and NGOs. The presence and involvement of various UN agencies including WHO, UNHCHR, UNHCR, and UNICEF and a host of international NGOs in the emergency settings working in health, education and other social sectors is notable. The humanitarian agencies conducted several sensitisation workshops focussing on health and human rights issues in various communities. In addition the various organisations have sponsored several radio programmes to communicate various messages on health and human rights in the districts and entire sub region affected by the conflicts. Rights holders (communities) in emergencies are usually vulnerable to human rights abuses/violations and health problems, due to a host of environmental, political, socio-economic factors, as well as exposure to educational messages and education level. Duty bearers including host governments and humanitarian agencies have the mandate, duty, and role to protect and provide health care to displaced populations11. Efforts by stakeholders to empower communities through provision of economic and educational opportunities and provision of information about health and human rights issues are of paramount importance. The involvement of UN agencies and NGOs can contribute towards strengthening capacities of national and local government and health systems to put in place an effective response and equitable access to health care services. Moreover the use of radio programmes to disseminate information is critical towards empowering rights holders to seek appropriate health care interventions and demand their rights from duty bearers. Access to health care by internally displaced women in camps is hampered mainly by lack of money, information and decision power. Efforts to improve the plight and welfare of women in emergencies implies establishing interventions that broadly encompass entire communities and reach out to women in particular because they often have more limited access to information and services as compared to men in society. Specific medium to long term measures/strategies towards empowering women to access health care services and to know their rights should include setting up income generating activities targeting women groups and promoting girls' education in primary schools including providing information about sexual and reproductive health rights. Previous studies by Orach and De Brouwere showed that in similarly affected conflict settings of the West Nile region, improved access to health care led to better met reproductive health (obstetric needs) for refugees than for the host population.12 This suggests that strategies to improve health care services accessibility in such settings ought to ensure strengthening the capacity of public health facilities; establishing a functional referral system for health emergencies (such as for emergency medical, surgical and obstetric care); availability of human resources for health, especially a skilled attendant at birth; as well as essential drugs and supplies. The support of humanitarian organisations including the UN, WHO, and international NGOs to support the local health system to carry out effective health care services remain vital. Gender based violence was reported to be common in the settings. This finding is not surprising. Several studies indicate that displaced populations are vulnerable to gender based violence owing to socio-economic and political reasons5, 13. Several medical interventions are being implemented towards the management of GBV survivors in the settings including treatment of injuries, testing and treatment for HIV/AIDS and other STIs; as well as non-medical interventions such as counselling services. Evidence from socio-cultural ethnographic studies have shown that societies where violence against women is low are characterized by strong sanctions against interpersonal violence, equality in decision making including about resources in families, and existence of community support for victims14. Therefore, increasing equality in decision-making including resources within families and community support for victims will reduce violence against women in the camps. Therefore there is need to train health personnel and equip health facilities to provide comprehensive medical, psychological and counselling services for the management of GBV survivors in the settings. The health care system in these conflict affected districts is weak. There are few health facilities, little skilled manpower, and referral services are poor particularly in the camps. Major medical, surgical and obstetric interventions are provided by private not-for-profit (PNFP) hospitals i.e. Kalongo in Pader and St Joseph in Kitgum district with only one public hospital. It is therefore imperative for duty bearers- government and relief agencies (UN and NGOs) to support and subsidise these PNFP health facilities and to strengthen the capacity of public health facilities to render effective health services. The capacities of the districts and sub-districts health systems need to be strengthened especially during the post emergency period, and more so as the population is currently returning to their original homesteads. Referrals services ought to be improved through availability of ambulance services as well as radio communication systems to link first line and referral facilities. Furthermore, there is need to provide incentives for the recruitment of more skilled health care providers who should be supported and motivated to work in such disadvantaged conflict affected settings. Conclusion and recommendations Our study suggests that most displaced populations are aware of human rights issues mainly through humanitarian relief agencies and the media in the settings. However, there is need to support and empower IDPs to demand for their rights through further sensitisation. Although geographic access to health services is high (due to facilities in the camps), this is expected to drastically reduce when the population is resettled in their homes in due course. Therefore there is need to establish mechanisms for effective health services delivery in the post emergency period (resettlement phase) including outreach services, strengthening referral system and establishing new first line health facilities. Capacities of first line health facilities including health centre level (II, IIIs and HCIV) ought to be strengthened. Referrals for medical, surgical and emergency obstetric care (EmOC) in the settings should be improved through availability of ambulance vehicles and other bicycle ambulances and radio or telecommunication networks. Gender based violence is perceived to be common in the settings. There is need for duty bearers including both central and local governments and the international humanitarian agencies i.e. UN and NGOs to strengthen community preventive and response mechanisms comprising health and social services interventions including medical, psychosocial and counselling services for survivors of gender based violence. More health personnel should be trained and health facilities equipped to undertake effective management of survivors for physical injuries, laboratory testing and treatment of STDs and counselling. Preventive measures against gender based violence need to be strengthened through improved community empowerment, legal enforcement mechanisms and community social networks in the camps and extended into the communities where the IDPs will settle. Acknowledgements The authors are grateful to WHO staff in Kampala including Dr Olu Olusayho, Nasan Natseri and Dr Michael Lukwiya for the support in the development of the study protocol and data analysis. Similarly we thank Dr Francis Oriokot and Mr David Opio of Kitgum WHO sub-office, and Mr Innocent Komakech and Mr Fred Olobo of WHO field office in Pader for their help with logistical arrangements towards data collection. The authors are grateful to EQUINET and the Uganda Health Equity Network for capacity support towards the publication of the paper. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09050t4.jpg] [hs09050t1.jpg] [hs09050t7.jpg] [hs09050t6.jpg] [hs09050t3.jpg] [hs09050t2.jpg] [hs09050t5.jpg] [hs09050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}