 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 71-74 Post partum haemorrhage in a teaching hospital in Nigeria: a 5-year experience *Ajenifuja KO, Adepiti CA, Ogunniyi SO Department of Obstetrics and Gynaecology, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife.
Osun, state Nigeria Code Number: hs10013 Abstract Objectives: The aim was to determine the incidence, causes and the maternal mortality associated with
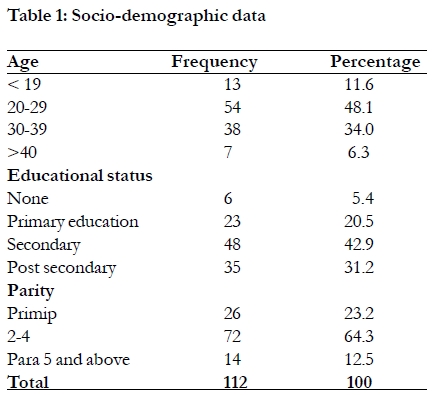
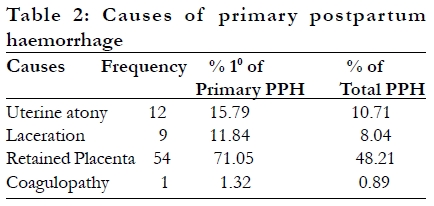
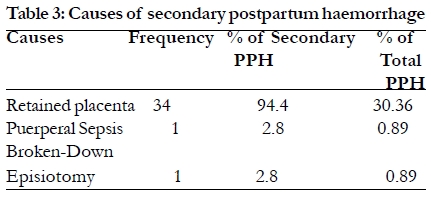
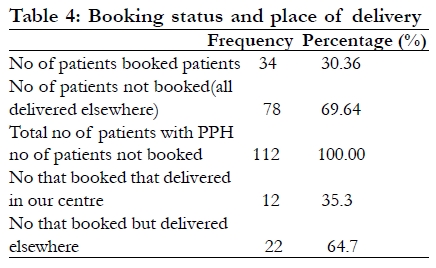
postpartum haemorrhage in a tertiary centre in Nigeria. Introduction World wide about half a million women die as results of complications of pregnancy and child birth childbirth1. Overwhelming proportions of these deaths occur in developing countries of the world where facilities are poorly developed and due to lack of trained attendants at delivery. Majority of these deaths occur within few hours of delivery and in most cases are due to postpartum hemorrhage 2, 3. Postpartum haemorrhage is a major cause of maternal morbidity and mortality worldwide with the highest incidence in developing countries. According to the World Health Organization obstetrics haemorrhage causes 127,000 deaths annually world wide and is the leading cause of maternal mortality 4. While in Africa, due to increased prevalence risk factors such as grand-multiparity, no routine use of prophylaxis against obstetrics haemorrhage coupled with poorly developed obstetrics services, obstetrics haemorrhage is responsible for 30% of the total maternal deaths.5 Postpartum haemorrhage is the excessive loss of blood per vaginam after the delivery of the baby and up to forty-two days postpartum. It can either be primary or secondary 4, 5 Primary postpartum haemorrhage is the loss of more than 500ml of blood within the first twenty-four hours of delivery or loss of any amount that is enough to cause haemodynamic instability in the mother or loss of more than 10% of the total blood volume. It is the most common form of post partum haemorrhage.4, 5, 6.It has been reported that approximately 3% of vaginal deliveries is complicated by severe primary postpartum haemorrhage 7. Secondary postpartum haemorrhage, on the other hand is defined as bleeding in excess of normal lochia after twenty-four hours and up to six weeks postpartum. In both cases the true blood loss is often underestimated due to the difficulty with visual quantification 8, 9,10. The risk of dying from postpartum haemorrhage depend not only the amount and rate of blood loss but also the health status of the woman 8. Methods Objective: The aim was to determine the incidence, causes and the maternal mortality associated with postpartum haemorrhage in a tertiary centre in Nigeria Method: The case notes of all the patients that were managed for postpartum haemorrhage after vaginal delivery in the Ife unit of the Teaching Hospitals Complex between 2002 and 2006 were retrieved. Socio-demographic data as well as data on booking status, types of postpartum haemorrhage, causes of postpartum haemorhage, morbidity, mortality from were retrieved and entered into a proforma specially prepared for it. Means and frequencies were calculated using the SPSS11 version. For the purpose of the study only women who had vaginal delivery and whose blood losses was 500mls or more were considered. Blood losses in our centre are estimated by visual quantification, measurement in graduated containers and estimating loses in the gauze packs. The exclusion criterion is women who had caesarean delivery. Results In the period under review, a total of 6672 vaginal deliveries were conducted, out of which 112 women were managed for post partum haemorrhage (PPH). The mean age of the patients was 31 years (18-47 years). About 20% of the women was primipara while the majority of the women (64%) were multiparous women. Most of the women were literate with close to 75% having at least secondary school education. About 90% of the patients were subsistence farmers or house wives as shown in Table 1. Post partum haemorrhage represents 1.68% of total vaginal deliveries in that period. Primary post partum haemorrhage (PPPH) constituted 67.87% while secondary postpartum haemorrhage constituted 32.14%. PPH occurred in 12% of booked patients while 88% occurred in unbooked and booked patients that delivered outside that hospital. The commonest cause of postpartum haemorrhage, in this study was retained placenta and it accounted for 78.57% of all cases of postpartum haemorrhage seen in our centre during the period under review, this was followed uterine atony in only 10.71% as indicated in Table 2 and Table 3. However, 88% of PPH occurred amongst patients that delivered outside the hospital (un-booked patients and booked patients that delivered elsewhere as shown in Table 4). The injuries were in form of laceration of the vulva, perineum, vagina, cervix or uterus (rupture) constituted 11.84% of cases. There was only one patient managed for Disseminated Intravascular Coagulopathy (DIC). Apart from the basic interventions offered, 2 (1.79) had hysterectomy when attempts at stopping the haemorrhage failed, while 51(45.5%) of the cases had blood transfusion. There were 6 maternal deaths. Discussion The exact incidence of PPH is difficult to determine due to the difficulty in accurately measuring the blood loses, most studies quote figures ranging from 5 to 12% of vaginal deliveries 11, 12. In this study, however, the incidence of post partum haemorrhage was 1.68% of total vaginal deliveries; this relatively low value may be due to the fact that ours is a tertiary centre where active management of the third stage of labour is routinely done with the use of oxytocics. The use of oxytocics has been associated with a decrease in the incidence of PPH by about 60% 13. Most of the patients in this review were those referred from other centres such as traditional birth attendants, faith clinics; primary health centres manned by poorly trained Community Health Workers (CHW) and womn who delivered in their homes. Patients that booked in our centre but chose to deliver elsewhere were not spared as they constituted majority of booked patients that had PPH. This was not surprising as expectant management of the third stage of labour is practiced in many traditional institutions due to lack of knowledge and unavailability of oxytocics agents. Unlike other studies 14, 15, also that reported uterine atony as the commonest cause of postpartum haemorrhage, in this study retained placenta was the commonest cause and it accounted for over half of the cases. Uterine atony was the second most common cause seen in our centre. Reason for this observation may because majority of cases seen were patients that had their delivery outside the hospital where the third stage was poorly managed. The high incidence of retained products of conception is closely related to the poor management of the third stage of labour. The current concept in the management of the third stage of labour is active management 20, 21,. This consists of interventions designed to facilitate the delivery of the placenta and prevent uterine atony by increasing uterine contractions and thus prevent postpartum haemorrhage 20, 21. The components include administration of uterotonic agents, controlled cord traction and uterine massage after the delivery of the placenta 20. Most of the deliveries complicated with postpartum haemorrhage seen in this study were conducted by unskilled attendants that have little or no knowledge of active management of the third stage of labour. The number of patients with genital tract lacerations in this study was less when compared with studies from other parts of the Nigeria 16, 17, 18. Since deaths from PPH are potentially preventable, its management should therefore start with the identification of these risk factors 6, 7, 18, 19, though it is known that postpartum haemorrhage can occur in the absence of these risk factors 5, 7, 15, 18. The next most important line of management is relief of the precipating factors, prompt and adequate replacement of intravascular blood volume. The proportion of women with secondary post partum haemorrhage appears higher, this might be due to delay in seeking care as most of the patients in this study were unbooked patients that whose delivery did not take place at our centre. Postpartum haemorrhage accounted for 6.67% of maternal mortality in this study whereas on the worldwide basis postpartum haemorrhage is implicated in 25% of maternal mortality especially from the developing countries 1,1. This low figure was probably due to the prompt and appropriate intervention given to the patients in order to prevent mortality due to haemorrhage in a tertiary setting such as ours with ready availability of emergency obstetric services. Apart from the mortality, PPH is associated with maternal morbidities such as increased risk of blood transfusion with it attendants complications, renal failure due to hypovolaemia, disseminated intravascular coagulopathy, failure of lactation and infertility. Over a half of the patients in this study had blood transfusion. Conclusion Post partum haemorrhage constitutes a significant cause of maternal morbidity and mortality. Most of the deliveries complicated with postpartum haemorrhage seen in this study were conducted by unskilled attendants that have little or no knowledge of active management of the third stage of labour. In order to reduce the morbidity and mortality from postpartum haemorrhage, every attendant at delivery needs to have knowledge, skills and critical judgment required to carry out active management of the third stage of labour and have access to appropriate supplies and equipment. Women should be encouraged to make use of existing health facilities by booking and receiving ante natal care. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10013t4.jpg] [hs10013t1.jpg] [hs10013t3.jpg] [hs10013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}