 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 312-319 Opportunities and barriers for implementation of integrated TB and HIV care in lower level health units: experiences from a rural western Ugandan district *Nansera D1, Bajunirwe F1, Kabakyenga J1, Asiimwe PK J2, Mayanja-Kizza H3 1 Mbarara University of Science and Technology, Mbarara, Uganda Corresponding author: Denis Nansera, Department of Paediatrics and Child Health, Mbarara University/ Mbarara Regional Referral Hospital, P.O.Box 1410, Mbarara, Uganda, Telephone: +256 782-964-417, Email: dnansera@yahoo.co.uk Code Number: hs10060 Abstract Background: As countries with a high burden of TB
and HIV roll out integrated TB/HIV care, there is need to assess possibility
of lower level health units treating TB to provide integrated TB/HIV care.
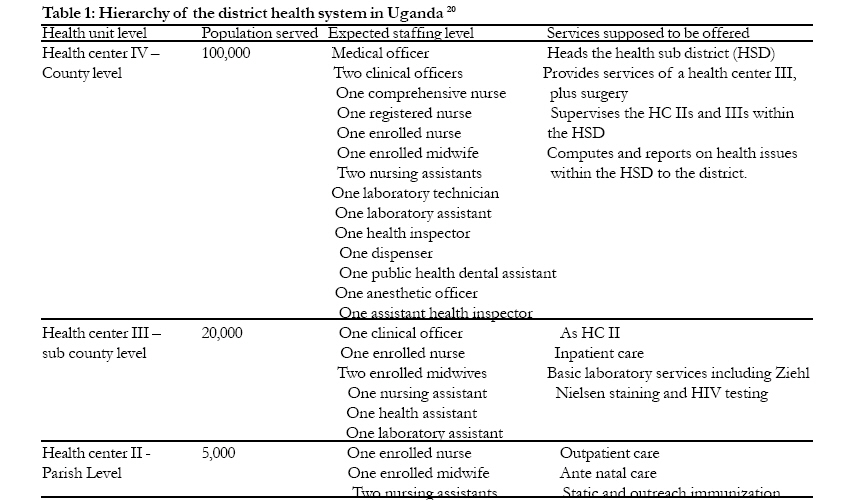
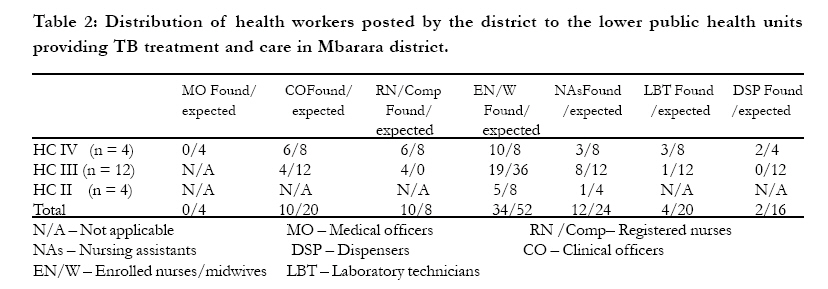
Key words Opportunities, barriers, lower health units, integrated TB/HIV care, Uganda Introduction There has been a worldwide increase in the number of TB cases especially in high HIV prevalence areas 1-3. It is against this background that the "The Global Plan to Stop TB" was launched 4. The initiative aims to halve death rates and prevalence of tuberculosis worldwide by 2015 and save over 14 million lives. One measure suggested to achieve this is strengthening collaborative TB and HIV activities in high HIV prevalence areas. Uganda has embarked on integrating TB and HIV prevention and care services as a way of improving treatment outcomes, intensifying case finding and contact tracing for both TB and HIV and maximize the use of available resources. A study was conducted to determine possible barriers and opportunities for provision of integrated TB/HIV care service in lower level health units offering TB treatment in Mbarara district, south western Uganda. We discuss the barriers and opportunities for provision of integrated TB-HIV care in lower level health units offering TB treatment. Methods Setting The study was conducted in 22 lower level health units offering TB treatment in Mbarara, a rural district in south western Uganda. The district has a population of 384,184 and 90% are peasant farmers. The regional annual population growth rate is 3.2 %5. The district health system is decentralized with health centers at parish, sub county and county level. The projected population served at the different levels, planned staffing norms and services offered at these levels are as shown in table 1. The district has four health sub-districts (HSD) which include Bugamba, Kashari, Rwampara and Mbarara Municipality. These are headed by Bugamba, Bwizibwera, Kinoni and Mbarara Municipality HC IVs respectively each at county level. The district has 23 HC IIs at parish level, 12 HC IIIs at sub county level, two private not for profit hospitals (PNFP), one faith based hospital and the regional referral hospital for western Uganda. The four hospitals are located in the Mbarara Municipality. The regional referral hospital is also the teaching hospital for Mbarara University Medical School and serves a population of above 1,000,000 people. It is the main TB diagnostic center in the region diagnosing close to 1,000 TB patients every year and serves as an HIV sentinel surveillance site for south western Uganda as well. The prevalence of HIV/AIDS in 2006 at this sentinel site6 was found to be 10%. The district has 6 centers accredited to provide antiretroviral drugs (ARVs) and these are located at the 3 hospitals and 3 of the 4 health center IVs. Study design This was a cross-sectional study with qualitative and quantitative methods of data collection. It was conducted between March 2008 and April 2008. The study was approved by Mbarara University Faculty of Medicine Ethics Review Committee and the Mbarara University Institutional Review Board (IRB). The study population included health workers (laboratory technicians, nurses, clinical officers, doctors and other health care providers) stationed in the 22 lower level health units offering TB treatment in Mbarara district. All health workers working in health center II, III and IV offering TB treatment were interviewed. In the two PNFP hospitals, we interviewed only those health workers directly involved with TB diagnosis and care. We did not perform any statistical sampling to obtain a sample. Data collection We collected two sets of information: health facility and health worker information. Information about the health facilities was collected through key informant interviews with the heads of the health units and through onsite observations in the laboratories, admission wards, the out-patient departments and areas where TB and HIV services are offered. The information collected to assess the health facility included; The health care facility level, the health workers posted at the unit, their cadre and whether the health unit was public or a private not for profit health facility. Available TB diagnostics, care and measures against acquiring TB among health workers in the health units, the availability of an algorithm to guide TB diagnosis among HIV patients, visiting the laboratory to determine the availability of facilities to perform Ziehl Nielsen staining and Mantoux tests and whether the health unit was performing chest radiography for TB diagnosis. Measures in place to reduce TB infection within health units were assessed through observations on use of masks, the ventilation of the clinical rooms and availability of safety cabinets in the laboratories. Available HIV diagnostics and care Availability of HIV diagnostics and care was assessed by determining the provision of HIV counseling and testing services, ability to offer cotrimoxazole for prophylaxis, insecticide treated nets and anti-retroviral therapy for TB/HIV co-infected patients. Practice in provision of integrated TB/HIV care This was determined by the ability of the health unit to provide HIV counseling and testing (HCT) to all TB patients, performing Ziehl Nielsen staining on sputum of HIV positive persons, whether TB/HIV co-infected persons were being offered TB and HIV care simultaneously in a single visit, and whether the unit was submitting an integrated TB/HIV monthly report to the National TB and Leprosy Program (NTLP) and AIDS Control Program (ACP). We also assessed integration by determining whether there was, follow up of TB patients and their contacts in the community and using Community Based Directly Observed Therapy Short course (CBDOTS) focal persons to send community contacts for both TB and HIV screening. Data collected to assess the level of knowledge about provision of TB and HIV care and possible barriers to provision of integrated TB/HIV care among health workers was collected using interviewer administered questionnaires. The information collected included knowledge about symptoms of TB disease among children and adults, knowledge about TB diagnosis in children and adults, order of getting sputum from a patient and concurrent use of rifampicin and nevirapine among the TB/HIV co-infected patients. Barriers/challenges to provision of integrated TB/HIV care To assess the barriers/challenges facing the provision of integrated TB/HIV care services, we asked the respondents whether under-staffing, high patient loads, lack of laboratory services, lack of care guidelines and insufficient knowledge and skills to offer integrated TB/HIV would affect provision of integrated TB and HIV care. We used open ended questions to obtain other barriers. Prior to administration of the questionnaire, we explained the study aims to the health workers and a written informed consent was obtained. We pre-tested the questionnaires on the medical ward of Mbarara Regional Referral Hospital and made relevant corrections to obtain the final version. We trained two research assistants in the administration and interpretation of the questions to ensure consistency in data collection. The interviews were conducted in private without interruption from other health workers. There were no incentives to those who responded to the questionnaires. Completed questionnaires were cross checked before departure from the data collection site to ensure completeness. Data analysis Quantitative data was entered into an Epi-Info version 3.3.2 database, cleaned and analyzed using the same Statistical soft ware. We used proportions to determine the deficits in staffing levels, health units screening for TB among HIV patients, screening for HIV among TB patients, offering simultaneous TB and HIV care for the TB-HIV co-infected patients in one clinic setting, conducting community follow up of TB patients using CBDOTS focal persons and those with measures in place to reduce acquisition of TB among health workers at their work places. We also determined the proportion of health workers who were knowledgeable about symptoms of TB, collection of sputum for Ziehl Nielsen staining, diagnosis of TB in children and concurrent use of TB drugs and some anti-retroviral drugs. Results Of the 22 lower level health units offering TB treatment assessed, 4 (18.0%) were HC IIs, 12 (55.0%) were HC IIIs, 4 (18.0%) were HC IV and 2 (9.0%) were private not for profit hospitals (PNFP). Overall, 88 health workers were interviewed. Of these 39 (44.0%) were enrolled nurses/midwives, 13 (14.0%) were nursing assistants, 13 (14.0%) were registered nurses, 12 (13.6%) were clinical officers, 5 (5.6%) were laboratory technicians, 3 were (3.4%) dispensers, 2 (2.3%) were medical officers and 1 (1.1%) was a radiographer. The public health facilities had only 50.0% of the expected health workers. None of the HC IVs had a medical officer posted by the district. (Table 2) The 2 medical officers interviewed were attached to a Presidential Emergency Plan For AIDS Relief (PEPFAR) funded HIV care program operating in two of the health IVs. Availability of TB diagnostics and measures against acquiring TB among health workers. None of the health units had an algorithm to guide the process of making a diagnosis of TB in HIV patients. Eleven (91.6%) of the HC IIIs lacked capacity to do Ziehl Nielsen staining. None of the health units had capacity to perform Mantoux tests and radiology services were only available in the two PNFP hospitals at a cost. Twelve health units (54.5%) were relying on proper air flow and ventilation to reduce TB spread from patients to health workers at the work place. All health units lacked face masks for both patients and health workers. None of the health unit performing Ziehl Nielsen staining had a safety cabinet. HIV care available Of the 18 health units mandated to offer laboratory services, 8 (44.4%) were not able to offer HIV counseling and testing services and all the 8 were HC IIIs. All the 22 health units were in position to offer cotrimoxazole for prophylaxis if it was supplied. Apart from the 2 HC IVs supported by a PEPFAR program, no other facility offered insecticide treated mosquito nets to HIV positive persons as part of the HIV basic care component for malaria prevention. The 2 PNFP hospitals and 3 of the HC IVs had been accredited to offer anti-retroviral therapy (ART). The HC IV that had not been accredited to offer ART was the farthest and hardest to reach from the regional referral hospital. One of the HC IV accredited to offer ART had not offered anti-retroviral drugs for close to 5 months prior to the assessment. This was attributed to under staffing, stock out of ARVs and other essential drugs and lack of functional laboratory services. One of the PEPFAR supported sites was offering onsite CD4+ counts and the other had a mechanism for delivering blood samples for CD4+ counts and other laboratory tests to the regional reference laboratory. Practice in provision of integrated TB and HIV care Only the 4 HC IVs, the 2 PNFP hospitals and 4 (33.3%) of the HC IIIs were testing for HIV among TB patients. Six (27.0%) of the 22 of the health units were performing on site Ziehl Nielsen staining for HIV patients presenting with cough. Apart from 3 HC IVs, two of which were supported by the PEPFAR program, and the 2 PNFP hospitals, no other health unit was able to offer TB and HIV care simultaneously in a single sitting for those with the dual infection. Eighteen health units (81.0%) were not able to do community follow up of TB patients and their contacts either using health unit staff or through CBDOTs focal person. Health centers III and II were regularly sending a combined report of TB and any HIV services offered to their supervising HC IV using the Uganda Ministry of Health Management Information System form. The HC IVs were aggregating these reports and forwarding them to the district as a combined TB/HIV report. The 2 PNFP hospitals were not regularly sending integrated reports to either the district or the ACP or NTLP. Knowledge about TB symptoms, diagnosis and use of TB drugs and ARVs All the 88 health workers knew the common symptoms of TB in adults. They knew that TB patients may present with a productive cough for more than 3 weeks, fever, night sweats and could lose weight and or appetite and at times present with haemoptysis. Eighty four (95.0%) and 72 (82.0%) of the health workers interviewed knew that TB would reduce children's growth and lead to loss of development milestones respectively. Overall 59 (67.0%) of the health workers believed sputum cannot be used for diagnosis of TB in children. They included 6 (50.0%) of the clinical officers, 6 (46.0%) of the registered nurses, 31(79.5%) of the enrolled nurse/midwives and 12 (92.3%) of the nursing assistants. The 3 dispensers and the radiographer also thought sputum examination had no role in diagnosis of TB in children. Fifty eight (65.9%) of the health workers did not know what the Mantoux test was and if it was a TB diagnostic test among children. Forty two (47.7%) health workers did not know the correct order of taking sputum for Ziehl Nielsen staining. Most of them were not requesting for an on-spot specimen but instead would request the patient to take the sputum mug home and bring the early morning sample. Only 36 (40.9%) of the health workers said it was not safe to use Nevirapine together with Rifampicin. Twelve (13.6%) said it was safe and 40 (45.5%) said they did not know whether it was safe or not. Attitudes and perceptions among health workers towards provision of integrated TB/HIV care Under-staffing, lack of knowledge and skills to offer integrated TB and HIV care, absence of guidelines to direct the provision of integrated TB and HIV care in a single sitting and lack of capacity to diagnose both TB and HIV were given as barriers to provision of integrated TB-HIV care. They remarked that these greatly affect the quality of care hence treatment outcomes. Most of the health workers thought that high patient loads were not a problem as long as there are enough health workers, enough supplies and they are equipped with knowledge and skills and mentored to offer integrated TB/HIV care. They acknowledged that where as the TB and HIV programs had trained most of them on the management of TB and HIV, they were more conversant with TB care since they were practicing it more often compared to HIV care. The health workers stated that HIV care is provided in a few selected health units. Even within these selected sites, HIV care is provided in specialized clinics not accessed by majority of the health workers, thereby keeping them out of practice as far as HIV care is concerned and denying them a chance to learn about HIV care. Discussion Our study has shown that under staffing, lack of capacity to diagnose HIV and TB, lack of guidelines to inform care options for TB/HIV co-infected patients and insufficient knowledge and skills among health workers towards provision of integrated TB/HIV care are the main barriers to provision of integrated TB/HIV services in lower level health facilities offering TB treatment in a rural Ugandan district. Although these barriers were identified in lower health units offering TB treatment in Mbarara district, they may be common to many other public health facilities in rural Uganda 8. The Health center IVs which are expected to operate as mini-hospitals and HIV care centers are the most affected. In addition to being understaffed, they lack vital cadres of health workers like medical officers and comprehensive nurses. This level of under-staffing and absence of critical cadres of health workers may work against the proposed strategy of using the existing human resource for provision of integrated TB/HIV care as suggested by WHO 4. Similar challenges with human resource have been cited in Zambia and Rwanda 9, 10 which are already piloting provision of integrated TB/HIV care. Experience from these pilot studies suggests that such staffing gaps compromise the quality of care, planning, monitoring and evaluation processes and implementation of interventions like task shifting and overtime payments which have been found to be effective in improving health services delivery in health facilities faced with understaffing 11. Similar to what has been observed in Zambia, Rwanda, and other sub Saharan countries 9, 10, 12 this study also identified lack of knowledge and skills among health care providers towards provision of integrated TB/HIV. This was more so in diagnosis of TB among children and concurrent use of TB and anti-retroviral drugs. Such knowledge gaps are likely to lead to delays in diagnosis of TB and institution of care. We believe this situation is even made worse by the lack of appropriate job aides and algorithms to guide decision making as was observed in the current study. The challenges towards provision of integrated TB/HIV care arising from understaffing and lack of knowledge and skills were further compounded by absence of critical services like capacity to diagnose tuberculosis among adults and children and provision of routine HIV counseling and testing. The inability to offer HIV testing was in part attributed to the fact that at the time of the study, provider initiated HIV counseling and testing (PITC) was just being rolled out in Uganda and within the region it was only being offered in the University teaching hospital 13. The HIV counseling and testing services in most of the units was offered as part of the prevention of mother to child transmission of HIV leaving out many patients including those with TB without getting an HIV test. Due to lack of laboratory technicians, most of the HC IIIs were not in position to perform Ziehl Nielsen staining. In terms of TB diagnosis, children were the most disadvantaged because none of the health facilities had capacity to perform a Mantoux test which is one of the tests suggested for diagnosis of TB among children 14,15. This lack of diagnostic capacity for both HIV and TB is similar to what has been observed in other African settings where provision of integrated TB/HIV care is being rolled out 9, 10, 12. . Nearly all health facilities lacked proper infection control measures within the TB treatment clinics and laboratories. The mainstay of prevention was air flow and ventilation. All the units lacked face masks for either the patients or the health workers. The few units performing Ziehl Nielsen staining lacked safety cabinets as well. Though the health workers did not consider lack of infection control measures as a challenge to provision of integrated TB/HIV care, there in need to put them in place and reduce the risk of acquiring TB within the health facilities. This study identified some opportunities on which provision of integrated TB /HIV care can be built. All the lower level health units offering TB treatment and care were in position to administer cotrimoxazole for prophylaxis when available. Such services can easily be improved to cover the entire HIV basic care package to include insecticide treated mosquito nets, safe water vessels, packages for prevention among positives and effective diagnosis and treatment of opportunistic infections especially at HC IIIs which are closer and more accessible to communities. This has been piloted and found to work in some programs in Uganda, Rwanda and Zambia with slight modifications to address the challenges of serving rural and urban populations 9, 10, 16. It was observed that all the health units offering TB treatment were within reach of the regional reference laboratory with capacity to run CD4+ counts and other TB and HIV care tests. Therefore mechanisms can easily be set up to maintain functional referral systems for either patients and/or specimens for laboratory services which cannot be offered for TB/HIV co-infected patients at lower level health facilities offering TB treatment. The health workers were also positive about provision of integrated TB/HIV care. Despite the challenges they were facing, they were offering some care, showed willingness to learn HIV care if offered an opportunity and did not envisage huge patient loads as a barrier to provision of integrated TB/HIV care so long as understaffing and lack of diagnostics and supplies were addressed. These positive attitudes are likely to yield positive results in the provision of integrated TB/HIV care as has been observed in well supported and funded programs in Uganda and other Sub Saharan settings 9, 10, 16, 17, 18. Our study had some limitations. We did not include an in-depth assessment of how the current structural infrastructure, delivery of supplies for health care, mentorship and support supervision programs, management and stewardship, vertical provision of TB and HIV services and communication gaps within the health units were imparting on provision of integrated TB/HIV care. The reasons for failure to attract health workers to work in Mbarara district as well as the perception of TB/HIV co-infected patients towards provision of integrated TB/HIV care were also not investigated. These were considered to be beyond the scope of the current study. Despite this, there was an opportunity for health workers to mention some of these as barriers to provision of integrated TB/HIV care through open ended questions. They mentioned some barriers like stock out of some essential drugs and the fact that HIV care was being offered in specialized clinics not accessed by majority of health workers denying them a chance to learn about HIV care as opposed to TB care which is offered by all health workers. Despite these limitations, our study gives an insight into the barriers which need to be addressed and opportunities onto which provision of integrated TB/HIV care can be built. The barriers point to a need for strengthening health systems and provision of integrated TB/HIV care in particular. The barriers and missed opportunity for provision of integrated TB/HIV care may compromise access to care for those with the dual infection. Accessing TB and HIV care in more than one place may lead to excessive movement by TB/HIV co-infected patients who have to receive TB and HIV care in different places and this may increase the risk of getting lost to follow up 12. As suggested by Simon J Tsiouris et al 19, the study findings pave way for programs supporting TB and HIV care in rural Uganda to plan and pilot implementation of TB/HIV collaborative activities within lower level health facilities offering TB treatment. It further highlights the fact that for lower level health units offering TB treatment in rural and resource-limited settings like Uganda to offer integrated TB/HIV care, the ministry of health needs to address the human resource needs, improve their diagnostic capacity for both TB and HIV, avail supplies for the HIV basic care package and other medical supplies and equip the health workers with knowledge and skills to offer integrated TB/HIV care. Conclusion For lower level health units offering TB treatment in rural and resource-limited settings like Uganda to offer integrated TB/HIV services at lower level health units currently offering TB stand alone services, there is need to address gaps in knowledge and skills among health workers, laboratory diagnostics, staffing levels, medical supplies and infrastructure. Acknowledgments This work was supported by a grant from the National Institutes of Health (ICOHRTA-AIDS/TB, Award Number U2RTW006879 from the Fogarty International Center NIH (EY1252601) We thank Professor Peter Mugyenyi, Dr Cissy Kityo, Miss Regina Namirembe and Mr Nelson Kakande of the COHRE secretariat at The Joint Clinical Research Center for their support. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10060t2.jpg] [hs10060t1.jpg] |
| |||||||||

{kind=link}
{kind=link}