 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Hepatotoxicity from first line antiretroviral therapy: an experience from a resource limited setting *Kalyesubula R1, Kagimu M1, Opio KC1, Kiguba R2, Semitala CF1, Schlech WF3, Katabira ET1 1Department of Medicine, Makerere University College of Health Sciences, Kampala, Uganda *Corresponding author: Robert Kalyesubula, Department of Medicine, Makerere University College of Health Sciences, School of Medicine, P. O. Box 7072, Kampala, Uganda, Tel : (+256)772442700, Email: rkalyes@yahoo.com Code Number: hs11002 AbstractBackground: Highly active antiretroviral therapy (HAART) has been associated with liver toxicity. The role of
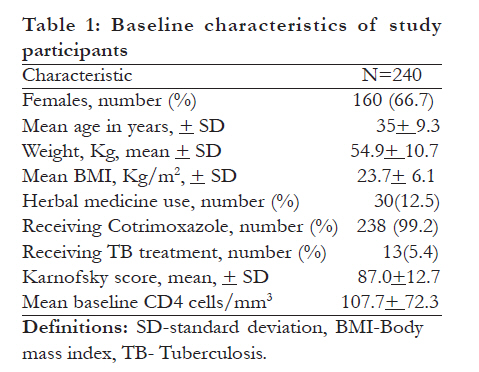
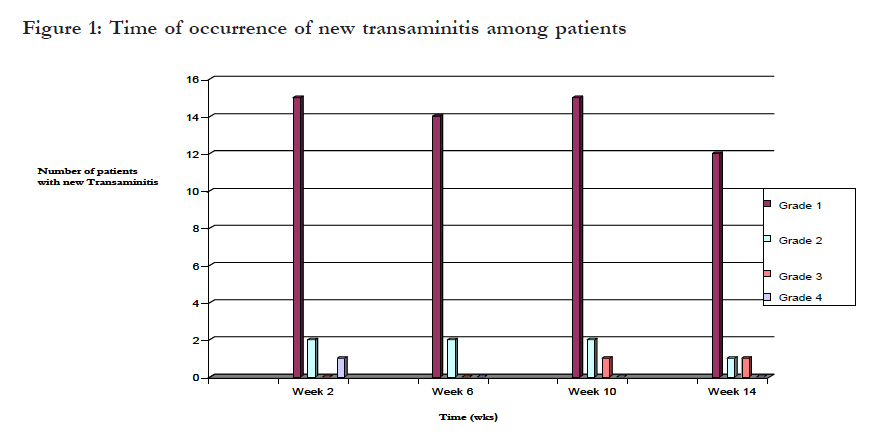
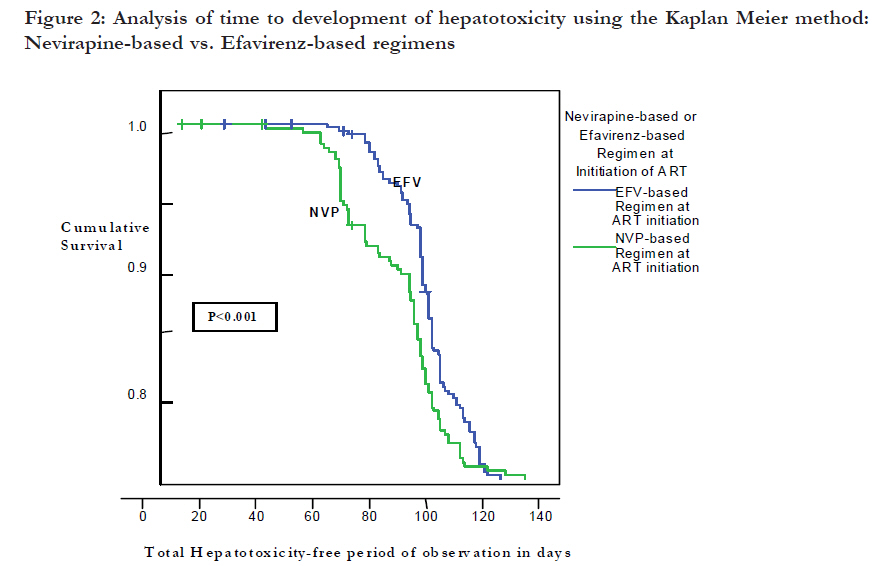
monitoring for liver toxicity has not been well studied in resource-limited settings (RLS). Keywords: HAART, Hepatotoxicity, Uganda Introduction Highly active antiretroviral therapy (HAART) has led to dramatic improvements in the survival of HIV-infected patients on treatment in resource-limited settings RLS1,2.However, antiretroviral drugs have been associated with both short- and long-term toxicities including hepatotoxicity, which may be life threatening3. The extent and risk factors for HAART related liver disease and the role of liver enzymes in monitoring this event have not been well studied in RLS. The current Uganda antiretroviral guidelines recommend monitoring of liver function tests (LFTs) every 6-12 months4. Based on clinical and laboratory findings, we determined the baseline prevalence and incidence of transaminitis as well as its related risk factors following HAART initiation and suggest the possible role of transaminases in monitoring liver toxicity in RLS.Methods Between October 2006 and May 2007, HAART naïve patients initiating any of the three first line HAART regimens [Stavudine (d4T)-Lamivudine (3TC) and nevirapine (NVP) prescribed as Triomune®); Zidovudine (AZT)-3TC and Efavirenz (EFV) or d4T-3TC-EFV] were recruited from two specialized out-patient HIV clinics[Mulago AIDS Clinic and the Infectious Disease Clinic (IDC) ] at the School of Medicine, Makerere University College of Health Sciences, Mulago National Referral Hospital in Kampala, Uganda.Patients were included in the study if they were: ³18 years, had documented HIV-1 infection, HAART naïve, willing to be followed up for at least 3 months and provided written informed consent. We obtained information on the demographic characteristics; history of use of alcohol; prophylaxis for opportunistic infections; concomitant use of other drugs within 4 weeks prior to enrolment; history of pre-existing liver disease; previous infection with viral hepatitis B or C; and use of herbal medicines. A clinical exam with particular emphasis on features of liver disease (e.g. jaundice and enlarged tender liver) was carried out and WHO HIV/AIDS stage was determined. Baseline laboratory evaluation including complete blood counts (Beckmann coulter counter), ALT (Biochemical analyzer Roche Integra c111), CD4 counts (Flow Cytometer), Hepatitis B surface antigen (HBsAg) and Hepatitis C antibody test [using the Cypress® Diagnostics; Langdorpsesteenweg 160 3201 Langdorp, Belgium HBsAg and HCVAb dipstick test kits respectively] were done. Hepatotoxicity as measured by the levels of ALT elevations was graded according to the AIDS Clinical Trial Group criteria (ACTG, 1996). Significant hepatotoxicity was defined as an ALT elevation of grade 2-4 in patients who had normal liver enzymes at baseline (using 40 IU of ALT as the upper limit of normal). During the follow-up period acute hepatitis was defined as development of one or more of the following signs and symptoms; right upper quadrant abdominal pain, jaundice and/or hepatomegaly not explained by any other cause in the presence of elevated transaminase. Patients found to have grade 2-4 transaminitis at baseline were excluded from further follow up. Patients were followed up on the, 2nd, 6th, 10th and 14th weeks after starting HAART as part of the routine care provided by the two clinics. On each of these visits a repeat clinical evaluation and blood for transaminase measurements was obtained. In addition assessment for adherence to HAART using self-report and pill counts was done. Patients who missed an appointment were contacted by phone if available and all efforts were undertaken to find out the reason as to why they missed. For the patients without phones who missed their visits; direct visits to their homes were made using the information provided in the first interview. A patient was considered lost to follow up if they missed two or more of their scheduled clinic follow-up appointments. The study was approved by the Faculty of Medicine Research and Ethics Committee of the School of Medicine, Makerere University College of Health Sciences and the Uganda National Council for Science and Technology. Statistical analysis We double entered data into EPI-Data version 3.1 and exported it to SPSS version 12.0 for analysis. Baseline and time dependent variables were assessed for all patients enrolled in the study and categorized based upon whether patients did or did not, complete the study. The incidence of hepatotoxicity within 3 months of HAART was determined as the number of new cases who developed new grade 2-4 ALT elevation at least once within three months after starting HAART. Time to hepatotoxicity was assessed by the Kaplan-Meier (KM) method and presented as person-months of follow-up for patients on different HAART regimens. We used the log rank test with p-value less than 0.05 as the level of significance to assess differences between the KM curves. A sub-analysis of the patients who developed hepatotoxicity was done to identify the proportion that developed symptomatic hepatotoxicity defined as the development of grade 2-4 ALT elevations with one or more of the following signs and symptoms; right upper quadrant abdominal pain, jaundice and/or hepatomegaly6. Bivariate analysis was done using odds ratios with 95% confidence intervals to compare factors in patients with hepatotoxicity to those without hepatotoxicity. We employed the Pearson Chi-squared tests or Fisher's Exact tests for categorical variables. Multivariate analysis of risk factors for hepatotoxicity in patients with transaminitis was done using Cox-regression analysis. ResultsPatient Enrolment Three hundred and sixteen patients were screened for the study. Of these, 240 (160 patients from Mulago AIDS Clinic and 80 patients from the Infectious Disease Clinic (IDC) met the inclusion criteria and were enrolled into the study. Two-hundred and two (84%) of those who started HAART completed the follow up period of 14 weeks. Baseline characteristics of the study participants enrolled to start ARTTwo hundred and forty (240) patients were enrolled to start HAART. The majority were on Septrin (Cotrimoxazole) prophylaxis and 66% were women (table 1). Thirty-eight patients did not complete the 14 weeks follow-up period of the study. The reasons for this included death, withdrawal of consent, transfer to other treatment centres and loss to follow up. However, there were no significant differences in patients who completed and those who did not complete the follow up period (table 2). None of the patients died from liver related problems during the study period. The baseline prevalence and incidence of transaminitis after 3 months of HAART The majority of patients (98.3%; 236/240) had no significant transaminitis at baseline. Of those with transaminitis at baseline; 4.6% (11/240) had grade 1 and 1.7% (4/240) had grade 2 elevations of ALT. Significant ALT transaminase elevations occurred in 4.2% (10/236) of the patients by 14 weeks on HAART with an incidence rate of 5.2 per 10,000 person months. Most of the patients had moderate grade 2 transaminitis (3.0%; 7/236). Grade 4 transaminitis occurred in only one patient (0.4%) who was taking Triomune®, in addition to anti-tuberculous therapy with isoniazid and ethambutol. The exact time of occurrence of transaminitis was unpredictable.All other grades of transaminitis were observed at nearly the same rate for each of the subsequent follow up weeks (figure 1). HIV/HBV and HIV/HCV co-infection was found in 7(3.3%) patients and 6(2.8%) patients respectively. Four of 56 (7.1%) patients with grade 1 transaminitis had hepatitis B while 3(5.3%) had hepatitis C. None of the patients who developed significant grade 2-4 transaminitis had co-infection with either HBV or HCV. Patients on nevirapine-based regimens developed grade 1-4 transaminitis at an earlier time than those on efavirenz-based regimen (Log Rank test = 12.1, p< 0.001) but there was no significant differences in the incidence of toxicity between the two regimens (figure 2). There was also no significant difference between the AZT and D4T based backbone therapies. Proportion of patients with new transaminitis who developed symptoms and signs of clinical hepatotoxicity A total of 66 patients developed new transaminitis. The most frequently observed sign and/or symptom was nausea 26(39.4%) followed by vomiting 22(33.3%), right upper quadrant pain 13(19.7%), hepatomegaly 11(16.7%), and jaundice 5 [(7.6%) average total bilirubin of 5.6 mg/dl with an upper limit of normal being at 1.5 mg/dl]. Jaundice was the main differentiating physical sign between patients with no transaminitis in comparison to those with moderate to severe transaminitis. Patients with grade 2-4 transaminitis were 15.5(95% CI: 5.3-35.1) times more likely to present with jaundice compared to those with no transaminitis. Other symptoms and signs were not significantly different between the two groups. Characteristics of patients who developed Grade 2-4 transaminitis Ten patients presented with grade 2-4 transaminitis with a median age of 33.0(IQR; 30-40.2) years. Eight (80%) were females. The median CD4 count was 80.5 (IQR-16.7-127.7) cells/mm3 with 4 (40%) patients having CD4 counts less than 50cells/mm3. The majority of the patients 7(70%) were in WHO stage III and IV. The mean BMI of the patients was 21.9 (SD-4.0) with 2 (20%) of them having a BMI of less than 18Kg/m2. Three of ten patients (30%) developed severe transaminitis of grade 3-4, with two of grade 3 and one with grade 4. The patient who developed grade 4 transaminitis was a female who was on Triomune®, isoniazid and ethambutol for the continuation phase of TB treatment with baseline ALT of 68 U/L and a cd4 count of 68cells/mm3. There was no death directly attributed to HAART associated hepatotoxicity. Trend of ALT among patients with grade 2-4 transaminitisThe median ALT elevation in the 10 patients reached a peak at 6 weeks of HAART and later returned to normal. The median peak level ALT was 77 IU/L (IQR, 69-104). The median time to reduction of ALT levels to grade 1 or less was 2.9 weeks (IQR, 1.23.8). Two patients with grade 3 and one with grade 4 transaminitis discontinued antiretroviral therapy as recommended by the ACTG guidelines. The remaining 7 patients with grade 2 elevations continued with HAART and their liver enzymes returned to normal during the follow up period. Comparison of characteristics of patients who developed grade 2-4 transaminitis with those who did not The baseline characteristics among the patients followed up for 14 weeks categorized by whether they did or did not develop grade 2-4 transaminitis. Anti tuberculosis treatment was the only significant differentiating characteristic between these two groups. Patients on concurrent HAART and antituberculous drugs were 16.0 (95% CI; 2.4-104.2, P<0.01) times more likely to have grade 2-4 transamintis. DiscussionBackground prevalence of transaminitis In this study the background prevalence of significant transaminitis (grade 2-4) among patients initiating HAART was low (1.7%). This differs from a similar study that reported baseline grade 2-4 transaminitis of up to 23% in a South African cohort6. The difference could be due to the lower prevalence of risk factors for liver disease like hepatitis B and C in our patients. In addition, most of our patients were receiving cotrimoxazole prophylaxis and prompt treatment for opportunistic infections; these infections may cause transaminitis if not well managed7. Several studies8,9 have described baseline liver enzyme elevations as a risk factor for severe hepatotoxicity in patients on HAART but few patients had baseline transaminitis in our study. However, the patient with grade 4 LEE had some elevation of ALT at baseline.The incidence of transaminitis within 3 months of HAART The incidence of significant (grade 2-4) transaminitis among the patients on HAART was low (4.2%). This low incidence is similar to that in a cohort of 97 patients who were initiated on a nevirapine-based regimen in Kampala (2.2%)(10) and in a 5-year cohort study in Botswana(1.1%)11. A recent study by Ocama et al has shown the similar findings with grade 3 LEE of 1.46% in 546 HIV positive patients attending the IDI Clinic12. The low incidence in our study could be due to the low prevalence of other risk factors for hepatotoxicity in our study population. In contrast, a randomised trial in South Africa found a high incidence of transaminitis (17%) among patients on a nevirapine-based regimen3. This difference might be accounted for by differences in baseline CD4 levels which were lower in our study. In addition 53% of our patients were on efavirenz-based regimens while the patients in South Africa were mainly on nevirapine-based regimens, which have been shown to cause early hepatotoxicity13,14 with increased frequency at higher baseline CD4 counts. Our study showed that the exact time of occurrence of significant transaminitis was unpredictable. Routine transaminases are unlikely to predict development of hepatotoxicity under these circumstances. None of the 10 patients with significant transaminitis in our cohort had chronic hepatitis B or C infection. Several studies9,13,15 have demonstrated that hepatitis B and C are risk factors for hepatotoxicity in HIV co-infected patients on HAART. In our study we used dipstick test kits for these viruses, which are less sensitive than EIA (enzyme immuno-assays) or tests to directly detect the virus. Seremba et al showed that rapid strip assays (RSAs) and even EIA may miss a sizeable number of patients with Hepatitis B or Hepatitis C in Ugandan patients16,17. Thus we may have underestimated the prevalence of these viruses in our study population. However, previous epidemiologic studies have shown a low prevalence of both HIV/HBV or HIV/HCV co-infections in Africa18 and Uganda in particular12. In the afore-mentioned study neither Hepatitis B surface antigen nor the HAART regimen influenced the LEE. Proportion of patients with new transaminitis who developed symptoms and signs of clinical hepatotoxicity The only sign that was statistically significantly related to transaminitis was jaundice. This occurred 15 times more in patients with grade 2-4 compared to those without transaminitis. This observation suggests that clinicians in resource-limited settings should routinely look for jaundice as a marker of significant transaminitis in patients on HAART. Once jaundice is detected, the measurement of transaminases should be done to assess the severity of hepatotoxicity. This is supported by studies that have found jaundice to be a good predictor of severity of liver disease19 and is in line with the current WHO recommendations20. This is also in line with the good evidence from the recently concluded DART (Development of anti-retroviral therapy in Africa (DART) trial; which showed comparable outcomes between clinically and laboratory monitored patients on HAART21,22. The main risk factor that differentiated patients with significant transaminitis (grade 2-4) from those without it was concurrent treatment for tuberculosis. A study from South Africa(6) showed that concurrent tuberculosis treatment with HAART is a great risk factor for hepatototoxicity with an increased risk of severe hepatotoxicity of 8.5 fold (95% CI, 2.7-27; P<0.001) and a study from Ethiopia23 also demonstrated that anti-tuberculous therapy was a risk factor for hepatotoxicity in HIV positive patients. This observation suggests that clinicians in resource-limited settings should routinely check for signs and symptoms of acute hepatitis in patients on concurrent HAART and anti-TB treatment. If any suggestive clinical features are noted then liver enzyme measurements should be done to assess the degree of hepatotoxicity.We found in our study that most of the transaminase elevations returned to normal despite continuation of HAART. This has also been noted in other studies10,24,25. This `normalization' of initial liver enzyme elevations despite continued therapy suggests that transaminase measurements should not be done frequently because, in most cases, the additional tests are unlikely to influence subsequent patient management. Moreover, indiscriminate use of these tests confers additional costs to already constrained health systems in RLS. Study limitations The limited period of follow up, the use of ALT as the only transaminitis marker and the small number of patients recruited in our study may have underestimated the incidence of possible HAART associated hepatotoxicity. The study only provides data on possible hepatotoxicity within the first months of HAART. In addition, only 10 patients had grade 2-4 transaminitis which limited our analysis for risk factors. None of the patients were on a protease inhibitor- based regimen so this study cannot address hepatotoxicity in patients taking those drugs as part of HAART. Bigger and longer follow up studies are needed to verify this finding in RLS. However, we still believe the information from this study can guide Clinicians caring for patients on HAART who develop LEE.Conclusions The incidence of severe hepatotoxicity within three months of first line antiretroviral therapy was low, suggesting that frequent measurement of transaminases in the first three months may not be necessary in all patients initiating HAART in RLS. Bigger and longer follow up studies are needed to verify this finding.Frequent measurement of transaminases may be more important in following patients on HAART and concurrent TB treatment as well as those with jaundice to avoid missing hepatotoxicity. Acknowledgements This work was supported by Grant Number U2RTW006879 (COHRE Training Programme Uganda) with support from the Fogarty International Center together with Makerere-Mbarara Teaching Hospital Joint AIDS Program -MJAP and the Infectious Disease Institute-IDI. The content is solely the responsibility of the authors and does not necessarily represent the official views of Fogarty International Center or the National Institutes of Health. We thank, the COHRE Team in Uganda and the study participants for their involvement and support during the study.References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11003t3.jpg] [hs11003t2.jpg] [hs11003t1.jpg] [hs11003f2.jpg] [hs11003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}