 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Acceptability of counselling and testing for HIV infection in women in labour at the University College Hospital, Ibadan, Nigeria *Bello FA1, Ogunbode OO1, Adesina OA1, Olayemi O1, Awonuga OM2, Adewole IF1 1Department of Obstetrics & Gynaecology, University of Ibadan, Ibadan, Nigeria Code Number: hs11005 AbstractBackground: Many patients are referred to labour ward as emergencies, and therefore do not benefit from the
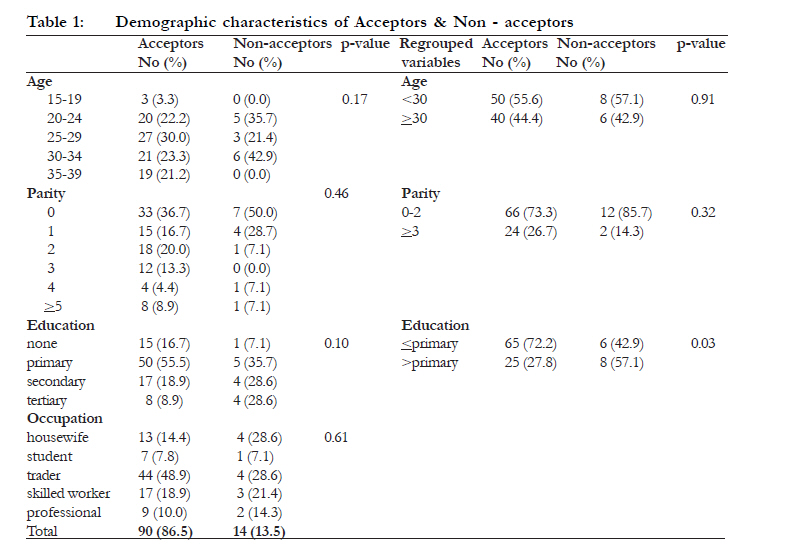
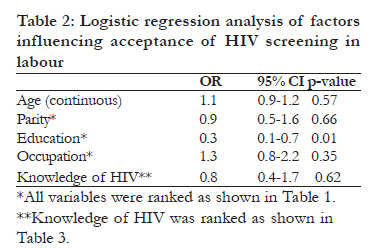
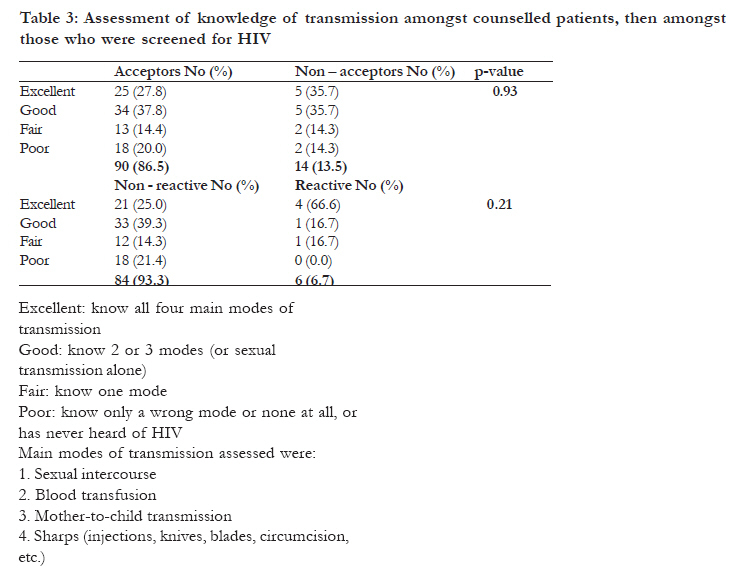
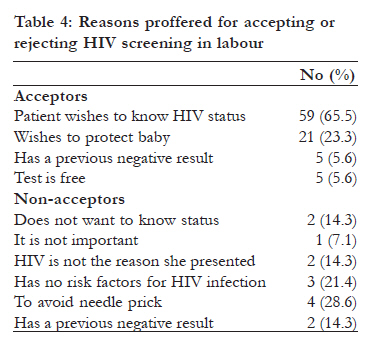
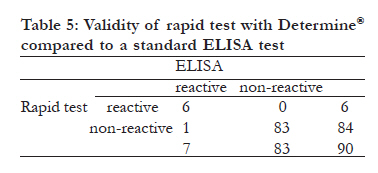
antenatal HIV counselling and testing and treatment offered to registered patients. Key words: HIV infection, rapid screening, labour Introduction Human immunodeficiency virus (HIV) infection has evolved from being a mysterious untreatable, invariably lethal illness affecting male homosexuals to a disease affecting mostly women of reproductive age and largely responsive to an array of therapies. Apart from the vulnerability of women themselves, it is also important for the newbornmore than 90% of infections in children is acquired through mother-to-child transmission (MTCT)1. Knowledge of the pregnant woman's HIV status will enable her to benefit from treatment for herself and interventions for prevention of MTCT (PMTCT). It also helps in public health surveillance, monitoring the effectiveness of intervention strategies and guiding research needs amongst others. An important consideration in screening in labour is the ethics of obtaining consent. Most women with unknown HIV status in labour represent a particularly vulnerable group in a particularly vulnerable situationthey often have not received any antenatal care, do not have an established relationship with the health care provider or system, are in the physically and emotionally demanding situation of labour, with their focus on anticipated delivery and pain alleviation. The circumstances of labour amplify the difficulties of pre and post-test counselling2. A woman may feel obliged to accept testing, despite her misgivings, because of the heightened emotional state in labour, and for fear of victimization or withdrawal of the emergency care that she presented for, in the first place. The Mother-Infant Rapid Intervention at Delivery (MIRIAD) study carried out by the Centers for Disease Control and Prevention (CDC) in the US sought to determine the feasibility and acceptance of informed consent for rapid testing and to evaluate the process in order to develop an effective and efficient method for approaching women in labour3. Eighty-four percent of their respondents consented to testing. At the University College Hospital Ibadan, all pregnant women are offered "opt-out" HIV screening (universal counselling and routine testing, except if patient declines)4,5,6 at their first antenatal visit. A significant proportion of women presenting in labour (being a referral centre) are not registeredonly 37% of Nigerian women attend antenatal care, as reported by the Demographic and Health Survey7and present as emergency cases and as such do not benefit from PMTCT servicesthus the importance of this study. The study aimed to assess the acceptability and suitability of offering voluntary and confidential counselling and testing (VCCT) to this obstetric population presenting in labourthis includes comparing their acceptance to that of the registered obstetric population which were screened during antenatal clinic; evaluating their attitude; and assessing the validity of the rapid kit. Methods It was a cross-sectional study, involving a total sampling method of consecutive unregistered pregnant women presenting for delivery at the labour ward of the University College Hospital, Ibadan from December 2005 to February 2006. The study setting was the labour ward of a government-owned tertiary referral centre that served most of South-Western Nigeria. Most patients presenting at this labour ward had received antenatal care in this hospital; yet a significant number of parturients were unregisteredsome having been referred from peripheral centres while some were self-referrals; having attempted delivery unsuccessfully at home or with traditional birth attendants or at a religious healing home (`mission home' in the local parlance). Most of them were not aware of their HIV serostatus. The minimum sample size was calculated as 73, using Cochran's formula for cross-sectional studies8. Five percent (0.05) was used as prevalence in the calculation (the prevalence of HIV in Nigeria9 at the time of the study). Deliberate oversampling was done to account for possible attrition. Based on the average number of unregistered patients admitted into labour ward daily, it was adjudged that about 2 months would suffice; therefore the study was carried out over 3 months. Ethical approval was obtained from the UI/UCH Institutional Review Board (protocol number UI/IRC/05/0104). Universal counselling was offered with the option of opt-out from testing. Written informed consent was obtained. A point-of-care (that is, carried out in labour ward by the investigator) rapid HIV test was performed for consenting patients using Determine HIV-1/2 (Abbott Diagnostics, North Chicago, Illinois, USA). Counselling and testing were carried out by a trained HIV counsellor who had a background in clinical nursing, but at the time was in full employment as a professional HIV counsellor. A blood sample was also taken for an ELISA test. A data sheet was filled out by the counsellor for each recruited patient after the counselling session, based on the responses made and information from their medical records. The data sheets contained the patient's biodata and information on their knowledge of HIV (modes of transmission, prevention and treatment), their willingness to be tested at the time, and open-ended questions on why they were accepting or declining testing. Counselling sessions lasted an average of 10 minutes; they were kept short in view of the peculiarities of labour. All patients tested were offered post-test counselling after the rapid test. Repeat ("double") consent was taken on the lying-in ward from all tested patients, 24-48 hours after delivery and the post-test counselling reinforced. This was to ascertain whether they had felt coerced to accept testing while in labour. Women who had declined testing in labour were counselled again post-partum, to compare their willingness to do the test outside labour conditions. Patients with reactive results had a confirmatory test by Western blot, but were offered PMTCT services meanwhile (anti-retroviral drugs to mother and infant, counselling on infant feeding, etc). Confirmed HIV-positive participants were counselled and referred for other HIV-related services in the hospital. Statistics on acceptance of HIV screening amongst our registered patients were retrieved from the antenatal clinic records for comparison. Data was entered into a password-protected Microsoft Excel spreadsheet while the hard copies of the consent forms and data sheets were kept in APIN's secure store for clients' personal data. Only code numbers (instead of names or hospital numbers) were entered in the records and used to label the laboratory samples. Data was analyzed with STATA-8 statistical software. Analysis was by ÷-square tests and logistic regression (Level of statistical significance p<0.05). ResultsFour hundred and eighteen women presented in labour over the study period, of which 311 had been receiving antenatal care. Of the unregistered, 104 women were counselled for HIV testing (3 were eclamptic and unconscious; and were therefore not counselled). Ninety (86.5%) accepted to be tested (95% CI: 80.5-93.4), while fourteen (13.5%) declined. Ninety-five women (91.3%) were aware of HIV, while nine (8.7%) had never heard of it. Acceptance rate during antenatal counselling was 99% (95%CI: 98.5-99.5). Table 1 shows the demographic characteristics of acceptors versus non-acceptors. The mean age of the respondents was 28.3±5.5 years. The modal age group of the acceptors was 25-29 years (30.0%)the mean age being 28.5± 5.7 years, while the mean age of the non-acceptors was 27.5 ± 4.6 years. Most acceptors were primigravidae (36.7%); most had only primary level of education (55.6%) and most were traders (48.9%). When all the various demographic data were re-grouped, only educational status had statistical significance. Of the 90 women that were tested, only 6 (6.7%) were reactive to HIV, while 84 (93.3%) were non-reactive. There were no significant differences between the demographic characteristics of clients that were reactice or non-reactive to HIV screening, respectively. The significance of education was adjusted for against the other demographic variables by an `enter' logistic regression model. This showed that level of education had an inverse relationship with acceptance (OR: 0.3; 95% CI: 0.1-0.7; p=0.01), when adjusted for age, parity, occupation and knowledge of risk factors (Table 2). The reference subgroups are the first in these tables for each variable i.e., age-15-19 years; parity-0; education-none; occupation-housewife; excellent knowledge of HIV, respectively. Most respondents, i.e. 69 (66.3%) had adequate (`excellent' and `good' in Table 3) knowledge of the infection's modes of transmission. Of these knowledgeable respondents, 59 (85.5%) accepted HIV testing, while 10 (14.5%) declined. Only 21 (20.2%) of the respondents were aware that there is any treatment available for HIV infection. The respondents were encouraged to proffer their reasons for accepting or declining HIV screening. These responses are collated in Table 4. None of the 90 patients that accepted testing admitted to doing so because they were afraid of being denied care. Most of them, 59 (65.5%) did so because they were genuinely interested in knowing their HIV status and 21 (23.3%) of them did it to protect their baby. Most refusals of screening were on account of aversion to needle pricksaccounting for 4 (28.6%). Of the 84 women that were non-reactive to rapid HIV screening, only one was reactive to ELISA screening. This patient's status was indeterminate by Western blot, however. All the 6 that were reactive to rapid screening were reactive to ELISA as well. All these 6 were confirmed positive by Western blot. Compared to a conventional ELISA screening test, the specificity of the rapid screening was 100%, sensitivity 85.7%, positive predictive value 100% and negative predictive value 98.8% (Table 5). All the women who accepted testing in labour re-iterated their consent when counselled again in the post-partum period. None of the women who had earlier declined testing changed their minds in favour of post-partum testing. Discussion The prevalence of HIV amongst unregistered parturients at the University College Hospital, Ibadan was higher than the average National prevalence of 5.0%9 at the time. The acceptance rate was significantly lower than in the antenatal population. This could be explained by the very nature of their emergency presentation in the first place, which may have displaced these women's attention from HIV testing. The demographic distribution of the participants showed that the less educated were more likely to accept HIV testing after counselling. Most participants were aware of HIV, as expected, in view of mass media public awareness campaign. Knowledge of the modes of transmission was also quite good, despite the fact that most of the participants did not have more than basic primary educationagain, a pointer to the effects of enlightenment programmes. This knowledge did not appear to influence a woman's acceptance of screening for her HIV serostatus in this study. Most patients, however, were not aware of any treatment modalities for HIV infection. These informational issues were all addressed during the counselling sessions, thus further improving their knowledge. The attitude of women to testing was encouraging, most of them desired to know their serostatus so as to afford themselves and their babies the opportunity of treatment. No one appeared to have been coerced into testing as a result of the vulnerability of presenting unregistered in labour, which was confirmed by all the tested patients' re-affirmation of their consent in the post-partum period. Most of the refusals were due to the fear of needle-pricks. Ironically, these women invariably had venepunctures in labour ward for blood tests, intravenous access etc. This could easily have been countered by taking the blood sample at the same time with the routine investigations, after obtaining consentthis will be the likely scenario in a real-life care setting, as opposed to a study (following this study, rapid screening has since been offered routinely to unregistered parturients in labour, along with other blood tests and has been well-accepted). It appears the stress of labour was not pivotal to their refusal, as they maintained their stance, even post-partum. Rapid screening tests are highly specific and sensitive10,11 and are useful for point-of-care testing in labour12,13, so that parturients can benefit from intervention. Accoucheurs are easily and quickly trained in its userequiring less than a day10, thus cutting out the time wasted in sending the samples to a laboratory in this emergency situation, so that the mother has enough time to make informed choices on the available treatment options. Results can usually be obtained within 20 minutes or less12,13. Studies have shown the high validity of Determine, the rapid test kit used in this study10,11 compared to ELISA and Western blot test. This was corroborated by the results of this study. The only discordant result was indeterminate on Western blot. Point-of-care testing evidently made the whole process feasible. The testing-disclosure interval of 20 minutes enables intervention to be instituted early. This was followed by the ACOG14, CDC15 and Nigerian Federal Ministry of Health4 recommendations that antiretroviral prophylaxis is offered immediately on detection of a reactive test to rapid screening, without waiting for the confirmatory Western blot. The cross-sectional study design employed was useful in determining the prevalence of acceptability of HIV testing in labour as well as the prevalence of HIV infection (which justifies the intervention in the first place) and in examining the associations. However, it is limited in being short-term as the results may have been different if carried out over another period. The non-probability sampling method would also likely introduce a selection bias. We feel this bias may be reduced, as the selection did not exclude any subjects (except those unable to give consent) but rather selected all subjects over a given period. This sampling method may be suitable for a pilot study such as this; used to determine the feasibility of introducing a new service. It however was less likely to ascertain the validity of the rapid testing; which was not the main aim of the study. The derived results were only rough estimates and more accurate tests of validity have been carried out by Kanal et al.10 and Aidoo et al.11. Conclusion The slightly higher prevalence of HIV in the study population than among patients that received antenatal care showed the importance of offering HIV counselling, testing and intervention in labour. It appeared to be acceptable and feasible. It is recommended that rapid kits be available for use in labour wards, and that the short training required for its use be carried out for all accoucheurs. Point-of-care testing and immediate offer of anti-retroviral therapy to parturients will go a long way to prevent the mother-to-child transmission of HIV. Acknowledgement The study received funding and technical support from the AIDS Prevention Initiative in Nigeria (APIN), Ibadan. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11005t4.jpg] [hs11005t1.jpg] [hs11005t5.jpg] [hs11005t2.jpg] [hs11005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}