 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Case-fatality of adult tetanus at Jimma University Teaching Hospital, Southwest Ethiopia *Amare A1, Yami A2 1Addis Ababa University, Medical Faculty, Department of Neurology, Addis Ababa, Ethiopia Code Number: hs11006 Abstract Background: Tetanus remains a major health problem in Ethiopia like in most other developing countries. Key words: Tetanus, case-fatality, complication, vaccination, Africa Introduction Even though the incidence and case-fatality of tetanus decreased markedly in developed countries1-6, it remains a major health problem in developing countries especially in sub-Saharan Africa7. Tetanus became a rare disease in the developed countries as a result of immunization and it occurs mainly in elderly due to decline in protective antibodies2, 8. In developing countries tetanus is common in the young due to lack of effective immunization program and appropriate treatment of injuries7. Tetanus is associated with high case-fatality rate which ranges from 6% to 72% depending on the availability of well equipped intensive care unit (ICU)3, 4, 6, 9-26. The availability of ICU was found to improve mortality from tetanus 9. Hadgu et al in 1975 in Addis Ababa studied tetanus patients from three different hospitals and found case-fatality of 36%26. Habte- Gabr et al in 1978 in Gondar ,Northwest Ethiopia found case-fatality of 55% in patients > 10 years old23. Hodes et al in 1990 analysed tetanus patients from Addis Ababa and reported case-fatality of 27 %25. Ramos et al in 2008 evaluated tetanus patients from rural area in Ethiopia and found a case-fatality of 20%24. In Jimma (located in southwest Ethiopia), like in most developing countries in the world, tetanus is endemic and remains an important health problem especially among the rural farming folks. In this study our objectives were to assess the clinical presentation, complications and treatment outcome of adult tetanus patients who presented to Jimma University Teaching Hospital (JUTH) which is 400-bedded referral hospital. Methods In this retrospective study of clinical records of tetanus patients (age >13years) who were admitted to JUTH from July 1996 to August 2009 were included. The study was started after getting ethical approval from Jimma University. Clinical records were searched manually .The individual case notes were then retrieved and studied. Confidentiality was assured by assigning each patient record a code number. Pretested datasheet was used to collect demographic and clinical data by the investigators. Tetanus was classified into generalized, cephalic and localized types. The severity of tetanus was classified into mild, moderate and severe 27. The diagnosis of dysautonomia was made when two or more of the following were fulfilled 28:
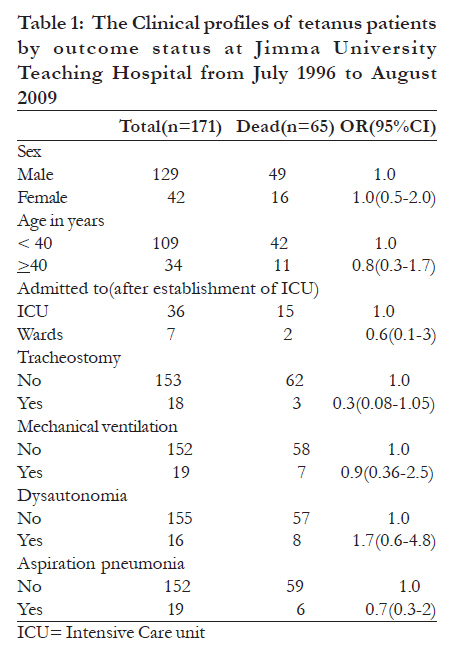
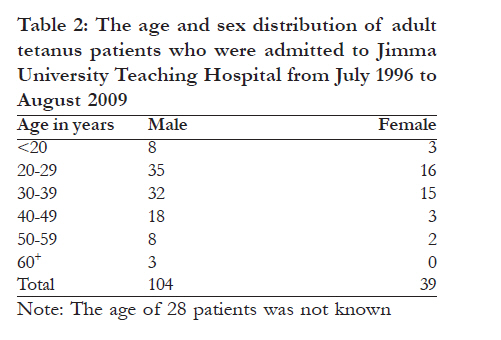
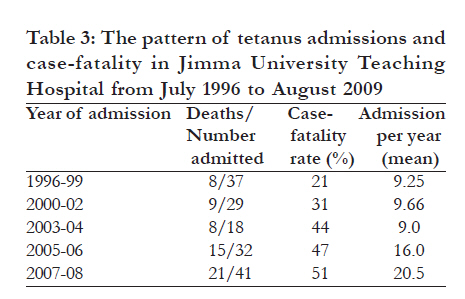
The data were analyzed using SPSS 13.0 for Windows (SPSS, Chicago IL, U.S.A). Odds ratios and significance levels were calculated along with 95% confidence intervals. The independent sample t-test was used to compare means. Results Data from 171 patients with tetanus were analyzed (129 males, 42 females, mean age 33 years). The mean age of males and females was 34 and 31 years, respectively (P-value>0.05) (Table 1 and 2). Before the establishment of the ICU, 90 patients were admitted to the hospital and after the establishment of ICU in May 2005, 81 were admitted. Of the 81 patients who were admitted after ICU establishment, 37 were managed in the ICU and 7 in the wards. We could not find out site of admission of 37 patients. The seasonal admissions were: June to August (n=45), September to November (n=41), December to February (n=36) and March to May (n=46).The mean hospital stay for patients discharged cured was 21.5 ±12 days and for deceased 6.5±6.7days. Twenty two patients (13%) had history of trauma [Information about history of recent trauma was not available in majority of our patients.] None of our patients had history of immunization for tetanus. The data about clinical type of tetanus was available in 48(28 %) cases only and 47 had generalized and one patient cephalic tetanus. Severity of tetanus was documented in 46(27%) patients and 43 had severe tetanus while 3 had moderate tetanus. No one had mild tetanus. The incubation period and period of onset was known in 24(14%) and 34(20%) patients, respectively. The mean incubation period and period of onset was 8±3.8days and 2.3±1.3days, respectively. Assessment of arterial oxygen saturation using pulse oximetry was done in 28 patients and it was < 90 % in 7 cases. Complications were documented in some patients: aspiration pneumonia (n=19), dysautonomia (n=16), respiratory failure (n=7), thrombophlebitis(n=7),bed sore(n=5), deep vein thrombosis(n=4), acute renal failure(n=1). Tracheostomy was done in 18(10.5%) patients and mechanical ventilation was used in 19(11 %) cases. Almost all patients were treated with tetanus antitoxine (human tetanus immune globulin was not available), diazepam, chlorpromazine and antibiotics. The case-fatality of tetanus was 38 %, with no difference between sexes. There was no significant difference between the mortality rates of patients aged < 40 years and e" 40 years. The case-fatality of patients with incubation period of more than 10 days and below 7 days was similar (33% versus 30%). The case-fatality of patients with period of onset of > 3 days and < 3 days was 27% and 39%, respectively (OR=1.7, 95%CI=0.4-8). The pattern of tetanus admission over the years and case-fatality is shown in Table 3. The annual tetanus admission increased from 9 to 20.5 over the study period. The case-fatality of tetanus showed increment progressively from 21% to 51 % over the years. After the establishment of ICU in 2005, there was no drop in case-fatality compared to the previous years (47% versus 44 %). The case-fatality of tetanus patients admitted to the ICU and wards after the establishment of ICU was similar. The mortality rate of patients with tracheostomy and mechanical ventilation was 16.7% (3/18) and 36.8 %( 7/19), respectively. Majority of the deaths occurred in the first few days: 38 % died in the first 3days while 84 % died in the first 10 days. Of the 106 patients discharged cured, 25(24 %) received tetanus toxoid at discharge. Discussion The majority of our patients were males (75%) and 92% were≤ 50 years old which is similar to other studies done in developing countries14-25. The male predominance could be explained by the fact that men tend to spend more time outdoor in farming activities and other types of field work. The fact that majority were young might reflect the Ethiopian demographics29 that 94% of the population was ≤ 59 year old in 2005. In contrast to our cases tetanus occurs mainly in older patients in developed countries 3-6.There was no seasonal variation in the occurrence of tetanus in our study in contrary to other studies1, 6, 23, 25. The mean annual tetanus admission increased from 9 to 20.5 over the study period. These might be due to the increased health posts, health centers, hospitals and health care workers in the area which improved awareness about tetanus. There was also improvement in infrastructures which made transportation of patients easier. None of our patients had history of vaccination for tetanus. Tracheostomy and mechanical ventilation was done in limited number of patients: 10.5% and 11 %, respectively. This is in contrast to other study done in Pakistan 12 where mechanical ventilation was used in 44% of cases. In a study done in India 28 tracheostomy and mechanical ventilation was done in 74% and 45%, respectively. In similar study from Malaysia 13 tracheostomy and mechanical ventilation was utilized in 100% and 86%, respectively. The case-fatality of tetanus was 38% in our cases which is similar to studies done in Italy, Brazil, Nigeria, India and Ethiopia which ranges from 33% to 39%4, 11, 16, 17, 26, 28. In contrast to our study both lower and higher case-fatality rates were reported in other studies. Lower case-fatality rates were reported from Japan (6 %), United States(18%), Venezuela (15%), Pakistan(25%), Malaysia(18 %),Indonesia and Nigeria(26 %), and Ethiopia (20% and 27%) 3,6,9,12-14,22,24,25. Higher case-fatality rates were reported from Turkey (58%), Tanzania (73%) , Nigeria(43% to 70%) and Ethiopia(55%)10,15,18-21,23. The case-fatality rate of tetanus was similar in male and female patients which is contrary to another study 16 which showed higher case-fatality for female patients. A few studies found higher mortality in old people11, 16, 18-20,22 , but we did not find differences in case fatality over age. The mean hospital stay of deceased patients was 6.5±6.7 days and majority of deaths occurred in the first few days: 38 % died in the first 3 days while 84 % died in the first 10 days. Tetanus patients who were treated conservatively(tracheostomy ,non-paralyzing muscle relaxants and sedation) died as a consequence of early acute respiratory failure while patients treated in ICU( maintenance of airway, ventilatory support, sedation ,relaxant) the main cause of death was unexpected cardiac arrest probably related to overactivity of the autonomic system9. Even though the cause of death was not documented in majority of our patients, the fact that most deaths occurred in the first few days may indicate that the main probable cause of death was early acute respiratory failure due to inadequate respiratory support. The case-fatality of patients with and without tracheostomy was 17 % and 41 %, respectively, which is marginally significant (Table 1). This may indicate that infrequent tracheostomy might have caused more deaths. The case-fatality of tetanus increased from 21% to 51% progressively over the study period. This might be explained by the improved awareness, health care services and means of transportation which might have increased severely ill tetanus patients to attend the referral hospital. This progressive increment in case-fatality was not improved after the introduction of ICU in 2005. These might be explained by the infrequent tracheostomy and mechanical ventilation done in our patients (10.5%and 11%, respectively).In contrast to our study, establishment of ICU decreased case-fatality of tetanus from 44% to 15% 9. Of the 106 patients discharged cured only 24% received tetanus toxoid prior to discharge which is higher compared to a previous study from Ethiopia 25 which was only 8 %. The limitation of this study was detailed medical history, physical examination, investigations, and treatment was not documented properly that it was not possible to get adequate information to assess clinical type and severity of tetanus and complications in majority of patients. Further analysis to identify more predictors of mortality was not done. This indicates that improvement in documentation and keeping of medical records is needed. Conclusion Majority of our patients were young males and none of them had history of vaccination for tetanus. The case-fatality was high and tracheostomy and mechanical ventilation was used in few patients. The mean annual admission and case-fatality rate increased over the study period. Establishment of ICU did not improve mortality. Most deaths occurred in the first few days indicating that our patients did not get adequate respiratory support. Tetanus is associated with high mortality and morbidity that can be fully prevented by vaccination. If it occurs patient should be treated in well equipped ICU with respiratory support and treatment of complications. Acknowledgment The authors are grateful to Jimma University Research Publication Office that funded the research. Our thanks also go to all staffs that were involved in the management of these patients. All authors report no conflict of interest. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11006t3.jpg] [hs11006t1.jpg] [hs11006t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}