 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
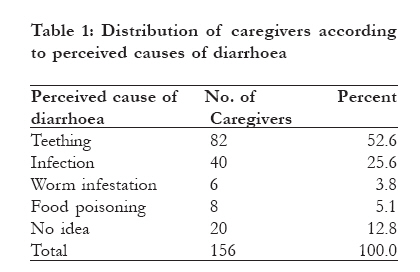
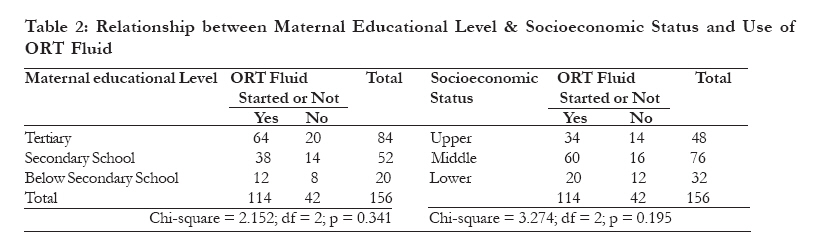
Pre-hospital management of diarrhoea among caregivers presenting at a tertiary health institution: implications for practice and health education *Emodi UO1,2, Emodi IJ1, Ikefuna AN1 1 Department of Pediatrics, University of Nigeria Teaching Hospital Enugu Nigeria Code Number: hs11007 Abstract Background: Diarrhoeal diseases cause significant childhood morbidity and mortality worldwide. The effectiveness of home management of diarrhoeal diseases is achievable only if caregivers have appropriate information despite varying recommendations on the strategies for diarrhoea therapy.Objectives: To evaluate caregivers' perception and use of ORT fluids for management of diarrhoea in under-five age children in the face of varying phases of recommendations, as an indicator of home treatment. Methods: Caregivers of U5 children presenting with acute watery diarrhoea to different Paediatrics clinics/wards of the University of Nigeria Teaching Hospital (U.N.T.H.), Enugu between October 2006 and February 2007 were interviewed with a structured questionnaire. Result: Caregivers of 156 under-five children who met the inclusion criteria were recruited. Access to ORT fluids was high with 73.1% of all children with diarrhoea being offered an ORT fluid at home. However, the method of preparation and administration of fluids was quite unsatisfactory. Previous experience with ORT fluids, higher educational or socioeconomic status did not correlate significantly with better performance. Conclusion: Despite high level of knowledge and acceptance of ORT among the study population actual practice was not satisfactory. Diverse practices by caregivers which represent the various phases of evolution in the types of fluids promoted for oral rehydration reflect some confusion that require urgent attention. Knowledge and skills of ORT need to be widely promoted on a continuing basis with the need for health workers to ensure that caregivers are taught and adhere to the correct recommendations on oral rehydration therapy. Key words: diarrhoea, ORT, home management Introduction Worldwide, diarrheal diseases are a leading cause of paediatric morbidity and mortality, with an estimated 1.8 million childhood deaths each year, accounting for 17 percent of childhood deaths.1-5 The pivotal role of oral rehydration therapy in the management of diarrhoeal diseases is well established.2 However, though global efforts to promote ORT in various forms resulted in an initial decrease in mortality from diarrhoeal illness when appropriately used, the gains are yet to be optimised especially in developing countries where diarrhoea plays the highest part in childhood morbidity and mortality. 6-8 A recent review suggests that barely 39% of children with diarrhoea in developing countries receive the recommended treatment with little progress made since 2000.9 The role of appropriate home management has been well recognised and recommended for almost all childhood illnesses in the community. It is a key strategy in management of childhood illnesses and forms a core component of the integrated management of childhood illnesses with a focus on helping caregivers to be able to recognise symptoms of common childhood illnesses and offer initial appropriate home remedies before presentation to a health facility. Thus, caregivers need to demonstrate ability to appropriately manage diarrhoea at home. Oral rehydration therapy (ORT) is the provision of oral fluids to replace fluids lost from the body. ORT encompasses two phases of treatment: 1) a rehydration phase, in which water and electrolytes are administered as oral rehydration solution to replace existing losses, and 2) a maintenance phase, which includes both replacement of ongoing fluid and electrolyte losses and adequate dietary intake.2 Recommendations for ORT use however, have evolved over time based on progress and changing knowledge of the scientific basis of diarrhoeal diseases and considerations of treatment feasibility. The mainstay of ORT has been the World Health Organisation oral rehydration salt (ORS) solution of which the standard pack is diluted with one (1) litre of water. However, alongside this other fluids have been promoted either as complementary, supplementary or substitutes depending on local circumstances of availability and acceptability. Another common solution for ORT is the salt sugar solution made by mixing 10 level spoons of granulated sugar with 1 level spoon of salt in 600 ml of water. The latter is often used where availability and/or cost limits the use of the standard WHO ORS. A recent addition that is yet to become widely implemented is the introduction of zinc-fortified ORS.9 Innovative delivery strategies to expand access to zinc and low-osmolarity oral rehydration salts are now being devised. Efforts are also being made at developing new flavours and packet sizes for oral rehydration salts9 Thus, presently there are ORS salts packs that should be mixed with varying amounts of water besides the standard pack meant to be mixed with 1L. The use of these different solutions which vary in both content and amount of fluids for oral rehydration is thought to have resulted in confusion amongst many caregivers leading to the practice of interchanging the recommended volume of water for instance, for SSS and that for ORS sachets. Recommendations on use of drugs in the management of acute diarrhoea should be followed strictly, since indiscriminate use of antibiotics results in development of resistance and may seriously detract from the standard recommendation on home management of acute childhood diarrhoea which includes oral rehydration solution, continued feeding during diarrhoeal episodes and zinc supplementation.10, 11 As a core component of evaluation of home management of childhood illnesses we evaluated the understanding and practice of home management of diarrhoeal illnesses among caregivers in our environment because of the anticipated effect of the various recommendations for ORT and also with the relatively recent introduction of hyposmolar ORS and zinc supplementation. We strongly believe this to be relevant in ensuring appropriate caregivers' knowledge base and right practices at home. Methods Participants consisted of mothers/caregivers with their under-five children presenting to different clinics and wards of the Paediatrics Department of U.N.T.H., Enugu between October 2006 and February 2007 which marks the late part of the rainy season and beginning of the dry season, corresponding to the peak of seasonal diarrhoeal illnesses. UNTH is the foremost tertiary health institution in Enugu state and in eastern Nigeria. It provides paediatrics care at all levels and attracts patients from both within and outside the state. People from all strata of society receive care at the Paediatric unit of UNTH which holds routine outpatient services, primary care and specialised clinics.Children presenting to the paediatric clinics of the hospital are managed in the Diarrhoea Therapy Unit (DTU) which is run as part of the paediatric emergency unit. Those not presenting in emergency states can be admitted into the wards and managed according to the underlying clinical problems. The activities of the DTU also include provision of health education to caregivers on the appropriate initial and basic steps in the management of diarrhoea at home prior to hospital visit. Practically, caregivers are shown how to accurately measure water from commonly available containers at home to reconstitute the ORS sachets. Information is also provided on recognition of common signs and symptoms that may suggest failure of home management and thus will necessitate hospital presentation. Patients included were those presenting with vomiting and acute watery diarrhoea with or without any other symptoms. Only patients without earlier consultations at any other health facility prior to presentation to our hospital were recruited into the study. Patients who had visited other health facility before presenting to UNTH were more likely to have received care by other health personnel which would have altered the care they received at home from their caregivers in the index diarrhoeal illnesses. Thus, we sought to capture only those that had been managed at home by the caregivers. All consecutive patients fulfilling the criteria were included irrespective of time of presentation to ensure that the sample was representative of all those who used the services of the hospital. There was no pre-determined sample size but study was conducted throughout the peak season for diarrhoeal disease among children presenting at the hospital. Altogether, one hundred and fifty six mother-child dyads were recruited into the study throughout the period of the study. Details of the study were explained to caregivers and only those who gave verbal consent were recruited at time of presentation to hospital. Informed verbal consent was considered adequate since the study was done within the framework of routine clinical care and did not involve any interventions beyond providing a post-evaluation health education. Information obtained using a structured questionnaire included: duration of illness, use of ORT solution at home, reason for or against using ORT, perceived cause of diarrhoea, method of preparation and timing of administration of ORT, previous experience with ORT. Caregivers who admitted to having administered an ORT fluid were asked the type of salt they had used and how they prepared the fluids. Volumes of water which caregivers quoted that they used to reconstitute the ORT fluids were cross-checked by asking them to give examples with common measures/containers in their homes. Typically, there are two major types of ORT fluids administered to children in Nigeria: The WHO ORS sachet which is mixed with 1L of water and the SSS consisting of a mixture of ten tablespoons of granulated sugar mixed with one tablespoon of salt mixed with 600mls of water. To ascertain accuracy of water used mothers were asked to describe common household containers that were used to measure the water used to prepare the fluids. Commonly accepted measures are: two bags of industrially purified 50-cl sachet water popularly called `pure-water'; water measured in three 35-cl capacity coca-cola bottles; water measured up to the first ring of a standard 1.5L industrially purified bottled water. On the other hand the commonly accepted measure of water for diluting the SSS has been two 30-cl coca-cola bottles of water or water measured from standard beer bottle. Those who had not used these commonly referable standards were asked to describe what they used to measure the water and these were crosschecked by interviewer. The containers used for practical demonstration of volumes of water to be used for preparation of the ORT fluids were also given to mothers so they can point out the level of water they had used. Since many of the mothers also brought along their prepared ORT fluids these were examined and the level of water used was assessed by interviewer. Also we enquired about use of antibiotics and medicines that were used to stop the diarrhoea (anti-motility preparations) at home. As not all mothers could remember the names of the medicines they had used those who brought along medicines they had used at home were asked to show same and these were examined by interviewers. The personal data and other determinants of socio-economic class were obtained. Participants were classified into either upper, middle or lower socio-economic classes according to the method proposed by Olusanya et al.12 Data are presented in tabular forms and analysis was done using the Statistical Package for Social Sciences (SPSS) version 12.5. Results Socio-demographic Characteristics:One hundred and fifty six caregivers met the inclusion criteria and were recruited. Majority of caregivers (84/156; 53.9%) had tertiary education while 52 (33.3%) had secondary school education and the remaining (20; 12.8%) had not completed secondary level education. Most caregivers (76/156 or 48.7%) were from the middle socioeconomic class (SEC) followed by those from the upper and lower classes (30.8% and 20.5% respectively). There were 88 (56.4%) male and 68 (43.6%) female children in the study. The majority were infants aged 0 - 11 months (106, 67.9%) followed by 12 - 24-month-olds (46, 29.5%); only a few children were 25 - 59 months old (4, 2.6%). Clinical Presentation and Caregivers' Perception Mean duration of illness before presentation was 4.5 days + 3.4 ranging from 1 14 days, while the commonest duration of illness prior to presentation was 3 days. There was no statistically significant difference between the mean duration of illness before presentation between those from upper (4.1 days), middle (4.5 days) or lower (4.2 days) socio-economic classes. Tooth eruption (teething) was considered to be a major cause of diarrhoea by 82 (52.6% of) caregivers. Other perceived causes are shown in Table 1. In relation to the maternal educational level, no difference was noticed with respect to perceived causes of diarrhoeal diseases. Home Management of Diarrhoea: A total of 114 out of 156 (73.1% of) participants had commenced their children on one form of rehydration fluid or the other before hospital presentation. About 30% of caregivers believed that ORT fluids could stop diarrhoea while 20% did not know that it helps to replace lost body fluids. Of 40 caregivers who did not commence ORT fluids before hospital visit 18 (45%) reported they had no previous experience with the use of any form of fluid. This was irrespective of the educational level and SEC. Other reasons for not commencing home fluids include ``not remembering to start ORT fluid though they claimed they were aware of its role in diarrhoeal illnesses'', `'not having enough time to prepare the fluid before hospital visit'', and `'not having ready-made ORS pack when they wanted to prepare it''. However, none thought that fluids could worsen the diarrhoea. The distribution of mothers who started ORT before presentation appears to have no statistically significant relationship with the maternal educational level and SEC (Table 2). Most children (92/114 or 80.7%) received the UNICEF oral rehydration salt (ORS) solution, while 22 (19.3%) got `salt-sugar-solution' (SSS). A significant number of children received fluids in which the salt was not properly mixed with right volume of water: 56/92 (60.9%) ORS mixtures were prepared with less than 1 litre of water while 6 out of the 22 SSS prepared by the caregivers were done with >600ml and 4 used <600ml of water for the recommended amount of salt and sugar. Overall, 66/114 i.e. 57.9% of the caregivers made and administered wrong mixtures of either the ORS or SSS solutions. Caregivers administered the solutions in different ways: 94/114 mothers used the solutions as the only fluids whether child passed watery/loose stools or not. Twenty (12.8%) of them gave fluids as per standard recommendation, i.e. after passage of loose or watery stools but also provided other home fluids including plain water in case the child did not like the taste of the ORT fluid. Maternal educational level did not seem to confer any advantage on being able to correctly mix the ORT fluids. Thus of 64 caregivers with tertiary level education half (32; 50%) made the fluids correctly while the other half did not; 12/38 of those with secondary school education reconstituted the fluids well and only 4/12 of those with less than secondary school education got correct mixtures of the ORT fluids (p = 0.154). Again the educational level of caregivers did not seem to have any relationship with being able to give the fluids in the recommended manner: as many as 50/64 with tertiary level of education, 32/38 of those with secondary level education and all 12 with less than secondary school education used the fluids as the only water offered to the child irrespective of the passage of diarrhoeal stools or not (p=0.177). There was no difference in method of preparation or administration of ORT fluids between mothers who had previously used any ORT fluid and those using it for the first time. Among 74 caregivers who had previous experience with ORT fluids only 34 prepared the fluids correctly in the index diarrhoeal episode, while 14/40 who had no past experience made correct preparations (p=0.259). Likewise only 12/74 of those with previous experience gave the fluids appropriately while 8/40 among those with no previous experience administered it appropriately (p=0.612). There was no statistically significant difference between both groups. Equally, the source of information on ORT fluids did not seem to affect the practice of the caregivers. Sources of information on the use of ORT fluids as reported by the caregivers were principally from nurses and other health care workers in health facilities (90/114; 78.9%), patent medicine vendors (10/114; 8.8%) and family members/neighbours/friends (14/114; 12.3%). Forty-eight of those who obtained their information from health facilities (nurses, 8 of those from patent medicine vendors and 10 of those from family/friends all made wrong mixtures of whichever ORT fluids that they had administered to their children. Most of the caregivers, 148/156 (94.8%) continued to offer feeds to their children up till time of presentation while 8 had stopped. Reasons for stopping were that: `'vomiting was too much'' (2/8), `'feeling that continued feeding might worsen the diarrhoea'' (4/8), and `'child refusing feeds'' (2/8). Sixteen (16) of the 80 children who were commenced on ORT fluids had stopped at the time of presentation with 4 stopping on day 1 of commencement, 2 each on days 2 and 3, and 4 each on days 4 and 6. Reasons for discontinuing ORT fluids were: failure of diarrhoea to stop (6/16), child was refusing the fluids (3/16), fluid administration seemed to worsen the volume of fluid loss (4/16), and child was too weak to accept the fluids (3/16). As many as 80 caregivers had commenced antibacterial medicines at home while 70 had given one form of anti-diarrhoeal medicines or the other prior to hospital presentation. Some gave both concomitantly. There was a direct relationship between degree of dehydration and number of days of illness before presentation with means of 3.8 days + 2.6 and 5.6 days +/- 4.6 for children with moderate and severe dehydration respectively, at presentation. Hydration status at presentation did not show any significant relationship to whether child received ORT fluids at home or not. However, among 44 patients who received properly reconstituted fluids none was severely dehydrated at presentation, as against 6/66 patients who got improperly made fluids. Discussion The present study demonstrates a reasonably high level of access to ORT fluids, with as many as 73.1% of caregivers reporting use of an ORT fluid at home before hospital presentation. This agrees with trends already documented from different countries and studies8 and according to a WHO report, even when measuring ORT use in each country according to the highest percentage of three indicators (Increased Fluid/Continued Feeding (IF/CF), ORS only, and ORS or SSS) the data show there is wide ORT coverage as well as increasing or stable trends within the majority of countries.13 However, the full benefits of ORT for acute gastroenteritis have not been realized, especially in countries with developed market economies that have lagged behind less-developed countries in their use of ORT.14-18 One reason for this low usage might be the ingrained use of intravenous (IV) therapy or the reduced appeal of a technologically simple solution.2, 14A worrisome observation of public health relevance is that many of the caregivers used incorrect amount of water to reconstitute the fluids. This is thought to be a result of the various phases through which the recommended home management fluids have passed. As such many caregivers did not know the difference between the recommended volume of water for preparing Salt Sugar Solution (i.e. 600mililitres) and Oral Rehydration Salt solution (i.e. 1000mililitres). Consequently children are offered fluids that are either hypotonic or hypertonic so that otherwise simple acute watery diarrhoea may be converted to hyponatremic or hypernatremic diarrhoea. Improperly mixed formula or oral rehydration solutions is recognised as one of the commonest causes of hypernatremia due to primary sodium excess.19 Conversely, administration of water in excess of solutes leading to water gain is cited as a cause of hyponatremia.19 Furthermore, many caregivers used the ORT fluid as the only fluid for their children irrespective of whether they passed any diarrhoeal stools or not. This practice has been identified by other researchers8 and is thought to be contributory to the prevailing high mortality rate from diarrhoeal illness despite the increased level of use of ORT.8, 20 The tendency is for many of such caregivers to forcefully administer the fluids and a child who dislikes the fluid may end up completely rejecting every other form of fluid offered to him/her. Replacing ordinary water completely with improperly reconstituted ORT fluids, as observed among our study population, may lead to giving children unnecessarily high solute loads when there is no loss via diarrhoeal stools. Despite the fact that ORT fluids remain the cornerstone of home management of diarrhoea it is recommended that caregivers should have other home fluids readily available in case their children do not like the taste of the ORT solutions.21 These are salient points which healthcare workers must consistently inquire from caregivers so as to ensure that the benefits of ORT are maximised because the ability of child caretakers to prepare a solution for oral rehydration correctly is very essential to a successful programme.20 Though some caregivers had used ORT fluids previously they did not perform better both in terms of the preparation and administration of the fluids when compared with those who were using it for the first time. And much more disturbing is the finding that there seemed to be no difference between the performance of those who obtained their information from the health facilities and outside. This underscores the basic problem which exists in terms of the accuracy of the information which these women had received and is a cause for concern because most of them had been in contact with health facilities at one point or the other. Again the likelihood of confusion arising from use of different types of ORT fluid may not be completely ruled out. The fact that among those who received properly reconstituted fluids (48/114) none was severely dehydrated at presentation, as against 6 patients among those who got improperly made fluids further supports the need for accuracy in preparation of ORT fluids. Though we could not assess the serum electrolyte status of our patients it is known that offering children improperly reconstituted fluids could lead to disturbances in their serum electrolytes including inducing possible hypo- or hypernatremia. Thus, it is recommended that a careful history should always be obtained as to the types and quantities of fluids which children with diarrhoea have received because a child with diarrhoea for several days who has ingested adequate water but little sodium may present with hyponatremia.19 The emphasis however, is that even in a setting where this test cannot be obtained for either reasons of cost or non-availability (and even prior to receiving the results when the laboratory tests can be done) detailed inquiry about ORT fluid preparation/use and attempt at correlating with the clinical features of the patient is very essential and may reveal some critical disturbances that underlie the clinical condition. We recognise some shortfalls of this present evaluation of home management of diarrhoea in our area of study. Firstly, we appreciate that a hospital based study is not very appropriate for assessing home management of diarrhoea. This was not our set goal but rather we sought to evaluate the home management of childhood diarrhoea among caregivers who eventually will present to a health facility. Our approach of limiting the recruitment to only those who had managed the children at home without any visit to other health facilities prior to presenting to us may have been a weak proxy to evaluating the practices of caregivers at home. The need for a more detailed community based survey cannot be over-emphasized but this could not be undertaken by the authors due to the constraints of time and cost. Even though this study did not show any difference in terms of performance between caregivers with different educational level it should be taken with caution. Higher maternal educational level is well recognised as a protective factor for childhood survival and confers the advantage of being able to understand and comply with life-saving health practices. Finally, it is possible that those who claimed to have received their information on ORT usage from health facilities may have had other sources of information leading to lack of comparative advantage. Information is often freely shared among caregivers and this practice may help reinforce the correct information or generate confusion. Conclusion Among our study population diarrhoea management in the home was grossly inadequate in terms of method of preparation and timing of administration of rehydration fluids. This poses some challenge to effective home management of diarrhoeal illnesses thus possibly undermining the efforts at reduction of infant and under-five mortality. We do not think that our findings may be peculiar to our environment and thus we believe that this may be crucial information to arm all caregivers involved in management of childhood illnesses. Health education for caregivers remains vital to the success of home management of diarrhoea. References
The following images related to this document are available:Photo images[hs11007t1.jpg] [hs11007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}