 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Assessing cold chain status in a metro city of India: an intervention study *Mallik S1, Kumar Mandal PK2, Chatterjee C3, Ghosh P2, Manna N2, Chakrabarty D2, Bagchi SN4, Dasgupta S5 1Dept of Community Medicine, Midnapur Medical College, West
Midnapur, India| Code Number: hs11019 Abstract Background: Cold chain maintenance is an essential activity to maintain the potency of vaccines and to prevent
adverse events following immunization. One baseline study highlighted the unsatisfactory cold chain status in city of Kolkata
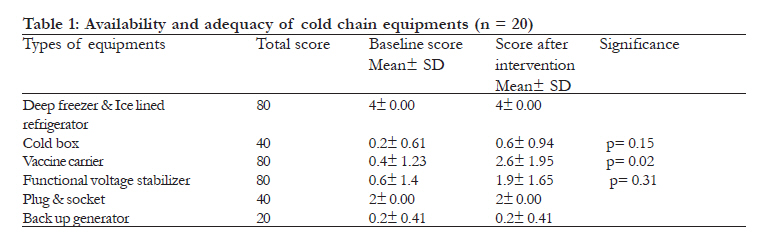
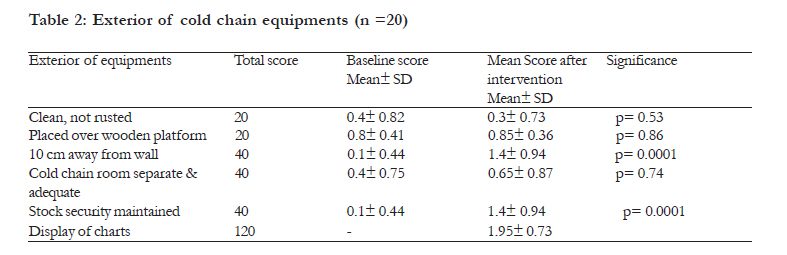
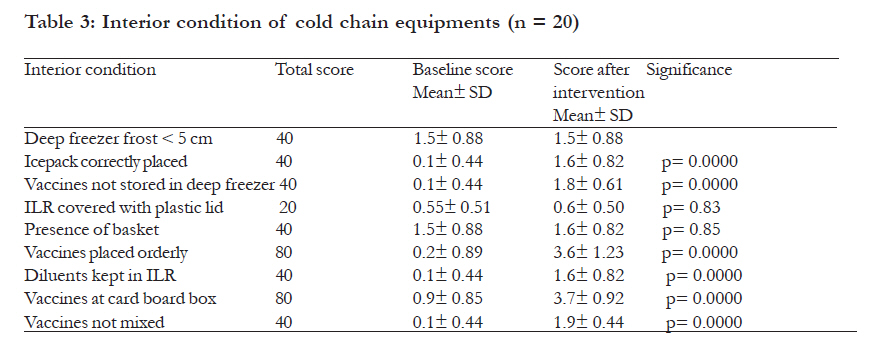
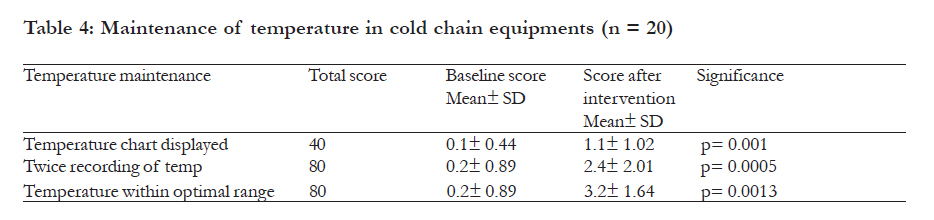
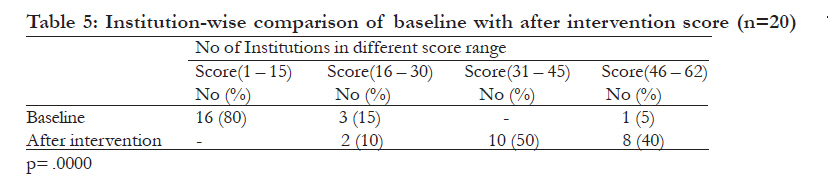
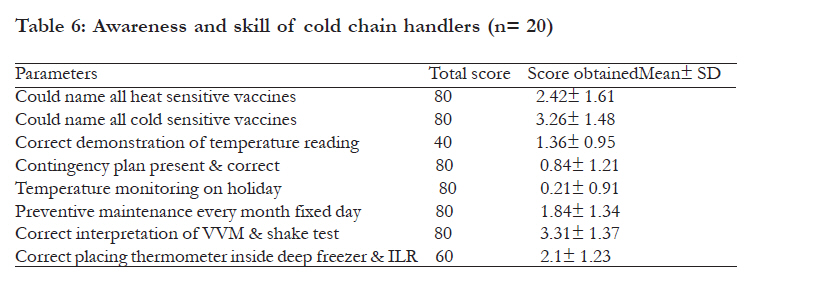
in India. Key words: Cold chain maintenance, cold chain equipment, intervention study Introduction Cold chain maintenance is a continuous and cohesive process of preserving vaccines to ensure their availability and to maintain potency. Cold chain maintenance1 is a term defined as the materials, equipment and procedures used to maintain temperatures between +2ºC to +8ºC while in transit throughout the distribution and storage process for vaccines from the manufacture point up to the beneficiary; where as cold chain also includes the people i.e. health workers2 engaged to maintain the equipment and temperature at peripheral levels. A cold chain break1 denotes a disruption in "cold chain maintenance", which could contribute to significant clinical outcomes, such as adverse reactions and/or missed opportunities to vaccinate. Prior cold chain evaluation studies2-4 had been reported as rapid assessments of the cold chain system in small sectors of urban India such as Bangalore, Delhi and Chandigarh, some cities of India. Researchers reported defects in the cold chain and the need to strengthen this mechanism to achieve successful polio eradication. Aggarwal et al3 in their assessment of the cold chain in New Delhi, reported 15% of vaccination clinics had a shortage of vaccine carriers. Goel et al4 reported unsatisfactory maintenance of the cold chain equipment in their evaluation of cold chain system in Chandigarh. Evaluation studies5-10 in UK, Georgia, Canada, Australia, Ethiopia and Madrid showed scarcity of maximum and minimum thermometers, thermometer reading to be outside the optimal range and low awareness of the cold chain handlers about its maintenance and ill effects of freezing on vaccines. A baseline survey of total cold chain status was conducted in early 2008 in the hospitals and institutions present in Kolkata Municipal area, a metro city of India. The survey revealed gross discrepancies in availability and distribution of cold chain equipment, innumerable cold chain points with improper utilization, lack of scientific knowledge regarding recent changes in cold chain guidelines as per the government of India (GOI) protocol11 and lack of monitoring and supervision. Based on the findings of the survey, one intervention was undertaken to centralize and reorganize the equipment to only 40 cold chain points, to facilitate expert monitoring and supervision. Simultaneously an in depth training on immunization and cold chain was conducted involving all the personnel directly accountable for immunization activity in these cold chain points. The present intervention study has been conducted with the objective to assess changes which occurred if any in the cold chain status following intervention. Another objective was to assess the awareness and skill of the cold chain handlers about basics of cold chain maintenance. Methods We carried out an institution based, intervention study in Kolkata, which is an important and well known city of India. The study period was from March, 2008 to April, 2009. A base line survey of cold chain equipment present in the centers, hospitals and institutions present in Kolkata Municipal area was done by the authors from March- April 2008. The intervention consisted of centralization and reorganization of the equipment to only 40 cold chain points and an in depth training on the immunization and cold chain conducted in July- August 2008 involving all the medical officers, cold chain handlers and public health nurses. Training content was formulated based on Immunisation handbook, government of India11 and was imparted using power point presentation with detailed discussion, and hands on training followed by field visits. Skill development training was also conducted for the designated cold chain handlers for each cold chain point regarding cold chain temperature monitoring including interpretation of Vaccine Vial Monitor (VVM), shake test; preventive maintenance; emergency contingency plan. After the training and reorganization of these cold chain points (after intervention), the status of cold chain system was re-evaluated in the month of March- April 2009. The two observations were compared. After restructuring, Kolkata Municipal area is presently having 1 cold chain point in 14 boroughs (administrative units of Kolkata Municipal Corporation), 1 each in 14 state and central government run hospitals and 12 in 6 medical colleges of Kolkata, to a total of 40. Out of those, 20 cold chain points were selected by stratified systematic random sampling method for evaluation. For comparison, baseline data of only these 20 points were considered. The cold chain equipment available in these 20 cold chain points was evaluated to assess the availability, exterior condition and placement of equipment, placement of vaccines, temperature recording, preventive maintenance, display of different charts by using an observation check list prepared as per GOI protocol11. For the second objective, the study population was the designated cold chain handlers (one in each cold chain point). These cold chain handlers were designated only after the intervention procedure. They were interviewed by a pre-designed pre-tested pro-forma to assess their awareness and skill about correct vaccine placement, heat and cold sensitive vaccines, interpretation of temperature chart, VVM and shake test and preventive maintenance of apparatus. The whole evaluation and interviews were conducted by the staff of the Dept of Community Medicine, Medical College, Kolkata who were trained and adequately briefed before the study to maintain uniformity and to avoid bias. All the parameters studied were scored by 3 experts of public health in Kolkata and based on their scoring; final scoring was done by authors. Ethical clearance was obtained from the appropriate authority before conducting this study. The analysis was done in Microsoft excel, SPSS version 17.0 and t test, ANOVA, Chi square tests were used as appropriate. Results Cold chain status of 20 cold chain points were evaluated and scored. For each parameter, the gold standard condition was given highest score which was multiplied with total samples to give the total score. For example if voltage stabilizer was present exclusively for each cold chain apparatus (table 1), that condition was considered as gold standard as per GOI protocol11 and was given score as 4, which when multiplied by 20 gave the total score as 80. From table 1 it was evident that availability and adequacy of cold chain apparatus did not differ so much between baseline and after intervention, except the adequacy of vaccine carrier which improved significantly after the intervention (p= 0.02). This happened due to shifting of vaccine carriers towards the cold chain points from the different areas where large numbers of vaccine carriers were stocked. While evaluating the exterior condition of cold chain apparatus, their placement, cold chain room as shown in table 2, significant changes were observed in placement of cold chain apparatus 10 cm away from the wall and maintenance of stock security (p= 0.0001). Display of charts included 4 charts viz. 1. Chart for correct placement of vaccines in ILR and correct placement of icepacks in deep freezer; 2. Chart for monthly defrosting date; 3. Chart for equipment details (date of installation, make no, source of collection, name and telephone no of the person to whom break down of equipment to be reported); 4. Chart for emergency plan in case of equipment break down or electric failure. In the baseline survey no organization was seen to maintain any chart. After intervention improvement was mainly observed in display of chart no 1. Regarding interior condition of deep freeze and ILR as indicated in table 3, significant changes were observed after intervention in the parameters viz: ice pack correctly placed in deep freezer, vaccines ot placed in deep freezer, vaccines placed orderly in ILR, diluents kept in ILR, vaccines kept at card board box and vaccines not mixed (p= 0.0000). The parameters encompassing the temperature maintenance in cold chain equipment were studied which included display of temperature chart outside the equipment, twice recording of temperature once in the morning and once at afternoon and showing temperature within optimal range. All the parameters improved after intervention (table 4). When comparing change of score according to number of organizations (table 5), significant improvement was observed where more organizations shifted towards higher score range (31 45 and 46 62) after intervention (p= 0.0000) (total score for gold standard parameters was 62). Institution-wise comparison of baseline and after intervention score was also done. Baseline average with SD were seen as 13.71± 1.79, 11.85 ± 3.71 and 19.33± 16.70 for boroughs, other Government hospitals and medical colleges respectively; whereas the respective after intervention average score with SD were 43.28 ± 8.28, 39.85 ± 10.73 and 44.5± 7.81. No significant difference was observed when comparing the average score for baseline (p= 0.35) and after intervention (p= 0.63) within boroughs, other Government hospitals and medical colleges. Interview of cold chain handlers (table 6) revealed poor knowledge of heat sensitive vaccines; lack of preventive maintenance, correct contingency plan and temperature monitoring on holidays. The findings could not be compared as no specific worker was designated as cold chain handler during baseline survey. Discussion The potency of vaccines depends on maintaining the cold chain-that is, a prescribed temperature range of 2-8°C during transport and storage. The GOI protocol11,12 recommended that each vaccine storage and distribution facility with electrically operated refrigeration equipment has a power generator to secure a reliable source of electricity. Handbook on Immunization guidelines11 by the government of India also recommended that each equipment should be connected to voltage stabilizer with permanently secure plug and socket. Aggarwal et al3 reported a number of shortcomings concerning the cold chain such as power failures and improper and inadequate maintenance of cold chain equipment15. Bachani et al13 reported a shortage of temperature maintenance equipment. Defective stabilizers and electricity plugs and sockets were the reason of breakdown in many cases as reported in Haryana14. The present study did not observe any shortage of electrical equipment, but scarcity of cold box, vaccine carriers and voltage stabilizers existed even after intervention. Samant et al15 showed generator facility in 65% of PHCs. Back up generator services was only available in 20% of the centers in the present study, as probably long term power failure was not so rampant in Kolkata. The GOI protocol11,12 also recommended that ice-lined refrigerators and deep freezers be supported on wooden blocks and be located at least 10 centimeters away from walls. The present study observed these as 85% and 70% respectively. Though it was improved after intervention, only 25% of the institutions had separate and adequate cold chain room. As per recommendation11,12 that lock and key be provided to a designated worker, stock security was maintained in 70% of the organizations. It was recommended11,12 that ice-lined refrigerators, deep freezers and refrigerators would maintain a temperature of 2° to 8° C and a temperature maintenance chart. The present study observed that 55% of the organizations maintained temperature chart, 60% recorded temperature twice and 80% maintained temperature in optimal range. A study in Canada7 had shown that the general and pediatric practice offices had maintained temperature chart, but only one third had temperature within limits. In Australia8 general practice vaccine storage points, daily checks were minimal due to lack of thermometers. A study in South India16 had shown temperature chart in 65% of PHCs. In UK5, vaccines were seen exposed to freezing temperature as well as temperature above 8 degree. As per the guidelines of GOI11, interior of cold chain equipment was properly maintained in 80- 90% of the organizations in the present study, where as vaccines were not placed orderly in a study in Ethiopia9. The present study observed significant improvement in scores regarding some parameters involving exterior and interior conditions of cold chain equipment after intervention. A study in South India16 observed 65% compliance score at PHC level, though methodology and parameters for scoring was different from the present study. Unlike Ethiopia9, UK5 and Australia8, the present study observed one designated worker as cold chain handler in 95% of organizations after intervention. These cold chain handlers lacked the knowledge regarding effect of freezing on vaccines10, but practical skill to interpret VVM and shake test was more in the present study. Preventive maintenance and formation of contingency plan were grossly neglected. The present study had seen improvement of scores in maintenance of cold chain system in different cold chain points after intervention. Limitation of the study This included failure to evaluate all the cold chain points and interview all the personnel involved in managing cold chain due to time constraints. Conclusion The present cold chain status of Kolkata had substantially improved after intervention i.e. reorganization of the cold chain points and training. The success achieved after intervention significant improvement of interior condition of cold chain equipment, placement of vaccines, temperature maintenance and creation of a designated cold chain handler in each cold chain point. Persistent gaps included non-availability of cold chain equipment like voltage stabilizers, back up generator services and separate and adequate cold chain room, which mainly depended on policy makers and funding. Preventive maintenance of cold chain equipment on a fixed day monthly, temperature maintenance on holidays and formulating a proper emergency contingency plan were also unsatisfactory. Monitoring and supervision by medical officers in this regard can bring about and sustain the changes. Moreover, a second reorientation training of cold chain handlers followed by a reevaluation of cold chain status is warranted. Acknowledgement The authors thank the health professionals and health workers working in organizations, hospitals and medical colleges of Kolkata Municipal area for cooperation. We also acknowledge UNICEF, Kolkata office for their funding and support for the intervention. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11019t6.jpg] [hs11019t2.jpg] [hs11019t5.jpg] [hs11019t1.jpg] [hs11019t4.jpg] [hs11019t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}