 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
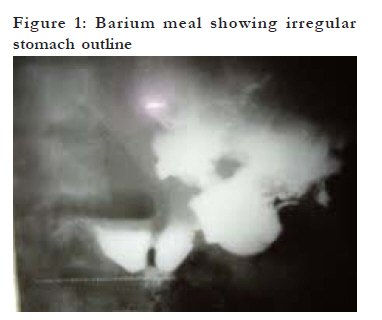
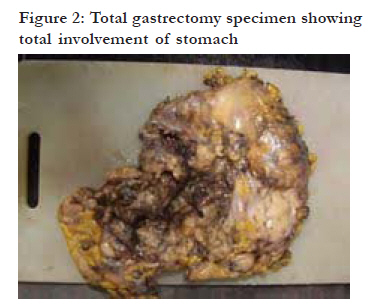
Case reports Gastrointestinal stromal tumour in Ibadan, Nigeria: a case report and review of current treatment *Afuwape OO, Irabor DO, Ladipo JK Department of Surgery, University College Hospital, College of Medicine University of Ibadan Code Number: hs11020 Abstract Gastrointestinal stromal tumours (GIST), though rare, present to the gastric surgeon not infrequently making a heightened awareness of this condition a pre-requisite of prompt recognition and timely treatment.. We describe the presentation, diagnosis and the limitations of treatment and follow up of a patient with GIST in a developing country. Surgery still remains as the only readily available modality of treatment in developing countries. Key Words: Gastrointestinal Stromal Tumours Introduction Gastrointestinal stromal tumours (GIST) are rare neoplasms of the gastrointestinal tract with an incidence of less than 1%. Most GIST are asymptomatic at the initial stage. Although still relatively uncommon, prompt recognition, accurate diagnosis and early intervention are critical in this potentially surgically curable disease. We describe a case of GIST in a forty-five year old man and the difficulties with management of GIST in a developing country. Case Report A forty five year old man presented with an eight month history of epigastric pain and weight loss and two months history of vomiting of recently ingested food. The pain was occasionally relieved with ingestion of antacids. There was a history of early satiety as well as recurrent episodes of haematemesis and melaena. He smoked about five to six cigarettes daily and took alcohol occasionally. He was chronically ill looking with fluffy hair, loss of cutaneous fat and a Karnofsky performance index of 60%, he was pale with no palpably enlarged peripheral lymph nodes. Abdominal examination revealed tenderness in the epigastrium. There was no palpable mass or demonstrable ascites. A diagnosis of gastric carcinoma was made. Oesophagogastroduodenoscopy revealed a dilated stomach with an extensive hemorrhagic mass with raised edges in the lesser curvature. The barium meal revealed loss of normal mucosa pattern and irregularities of the lumen of the whole stomach excluding the duodenum (fig.1). Abdominal ultrasound revealed a thickened stomach wall but no specific lesion was visualized. There was no radiological evidence of hepatic metastasis. The biopsy result obtained from the gastroscopy showed chronic gastritis. He was worked up for surgery. Findings at surgery were minimal ascites, a large exophytic mass involving the body and pylorus of the stomach infiltrating the pancreas, transverse colon and the spleen (fig.2). The liver was grossly normal. He had a total gastrectomy, transverse colectomy, splenectomy and distal pancreatectomy with a loop oesophagojejunal anastomosis and jejunojejunostomy. Postoperatively the patient was commenced on oral intake on the fifth day. He was discharged home a month after surgery to be seen on outpatient basis. Histology of the stomach showed a malignant mesenchymal tumour composed of spindle shaped cells with moderate cytoplasm and hyperchromatic nuclei .The predominant pattern of differentiation was of the smooth muscle type. There were 2-3 mitotic figures per high power field. These features are in keeping with a gastrointestinal stromal tumour (GIST) of the stomach. The implications of the histology report were discussed with the patient. He was seen in the surgical outpatient clinic for follow up. He was symptom free for the next three months following surgery. On his fourth clinic visit he complained of right hypochondrial pain. Examination revealed an enlarged nodular liver. Abdominal ultrasound revealed multiple hepatic metastases. He continued to deteriorate and his failure to show up for his fifth clinic appointment portends severe morbidity or mortality. He lived for about eight months post-surgery.Discussion Gastrointestinal stromal tumours (GIST) are mesenchymal tumours commonly claimed to originate from the neoplastic transformation of intestinal pacemaker cells (Intestinal cells of Cajal) 1,2,3. GIST comprise a majority of tumours previously thought to be gastrointestinal leiomyomas, leiomyoblastomas and leiomyosarcomas. They also include tumors hitherto diagnosed as neurofibromas or schwannomas2.There is no doubt that most of GIST originate from the pacemaker cells of Cajal, however the presence of the receptors in omental tumors, the mesentery and uterine tumors has raised doubts about the exclusivity of their origin from pacemaker cells3,4. The tumour arises predominantly in the stomach (60%) small intestine (25%) and the rectum (5%). Other rarer locations are the gall bladder pancreas and the retro- peritoneum5. The peak age of presentation is about 60 years. There is no consensus on the classification of GIST; however the pattern of recurrence even after twenty years supports the classification as; low, intermediate and high-risk for malignant behavior6. Indices for prognostication include the size, mitotic index and location of the tumor. Others are intratumural necrosis, aneuploidy, the presence of metastasis at presentation and the age of the patient7. GIST often present with mass related symptoms, anemia or as a result of features of mucosal ulceration. Occasionally they are incidental findings in radiologic imaging or secondary findings in resected specimens8. The diagnostic evaluation is determined by the mode of presentation. Patients who present with gastrointestinal hemorrhage are often diagnosed by oesophagoduodenoscopy which may reveal a sub- mucosal mass. Routine endoscopic biopsy samples rarely contain tumour cells. Endoscopic core biopsy increases the yield with a risk of hemorrhage. Percutanous biopsies are acceptable for inoperative tumours9. GIST are typically immunoreactive for KIT. KIT is a transmembrane receptor (CD117) which is part of the tyrosine kinase receptor complex. Thus in centers where this facility is available one can confirm the diagnosis of GIST with immunohistochemistry; CD117 positivity is seen in about 90-100% of GIST while positivity for CD34, the hematopoietic progenitor cell antigen, is reported in 70-80% of GIST10,11 .Other useful diagnostic modalities are computed tomogram and magnetic resonance imaging which are appropriate for staging and organ invasion12 . Recent studies have demonstrated an extremely valuable potential for preoperative positron emission tomography (PET) 13. Direct spread and metastatic spread, (often hepatic and less often peritoneal) are common. Other sites of metastasis include the retro- peritoneum, lungs, bones and the brain. Ascites and lymph node metastasis are rare. Surgery remains the main modality of treatment in primary GIST. Meticulous dissection is required to avoid intraoperative rupture of the tumour. The exophytic nature of the tumour may necessitate resection of adjoining structures to achieve negative surgical margins however the status of the margins are not as important as direct shedding of tumour cells into the peritoneal cavity. The five year survival of patients with complete tumour is 88% 7 . This is dependent on the histogical grade of the tumour 7. The post operative treatment of these patients is with a combination of clinical evaluation and appropriate imaging techniques directed at early detection of resectable confined relapses14. The liver and peritoneum are the most common sites with a median time to recurrence of 1.5 to 2 years 15. Conventional chemotherapy has a limited role in the treatment of GIST. However the advent of targeted therapy with Glivec (Imatinib) a tyrosine kinase inhibitor has shown some promising results. Prior to the use of imatinib the response to chemotherapy was less than 10%.The survival was 41% at 2 years and 25% at 5 years with a median survival of 19months. The current data on the use of Glivec demonstrates a response in 50% and a stable prolonged disease in 75%. Indeed some reports have encouraged the use of neadjuvant Glivec therapy especially in patients with massive tumours in a bid to avoid multi-visceral resection. This modality of treatment downstages the tumor to an extent that a planned total gastrectomy may then be substituted with a partial gastrectomy11. At present Glivec is not readily available in developing countries thus making the outcome of GIST treatment very poor. In our patient total gastrectomy had to be performed by necessity knowing that battling with post-gastrectomy nutritional problems was going to be the price we would have to pay. Leaving the patient with gastric outlet obstruction and recurrent severe hematemesis was not an option we would have been comfortable with. Indeed the patient's quality after surgery did not change significantly from his 60% Karnofsky assessment pre-operatively. His dietary intake was mostly semisolids and fluids and he needed to sleep propped up at night to avoid reflux into his oesophagus but he was able to care for most of his personal needs with occasional assistance. His cause of death was attributable to progression of the malignancy through massive and multiple hepatic metastases. Problems in developing countries Magnetic resonance imaging (MRI) and computerized tomography (CT) scan are beyond the reach of most centres. The cost of these investigations in tertiary centres with these equipments is out of the reach of many patients. Importantly most of our laboratories do not have facilities for immunohistochemistry and those that do probably may not stock the antibodies against the KIT receptor (CD 117) because of the rarity of GIST in this environment. All these combine to make pre-operative diagnosis very difficult if not near-impossible thus surgery to remove the gross tumour remains the only readily available treatment modality. Recent reports have demonstrated an 88% 5 year overall survival following R0 resection margins compared with 0% following palliative surgery7. Tyrosine kinase inhibitors are expensive and difficult to procure. Thus follow-up is just for assessment of the tumour free period and probably survival data. The outlook for this type of malignancy will continue to be grim until effective awareness campaigns for screening and yearly full physical examinations for adults above 45 years is entrenched. The screening may just be upper gastrointestinal endoscopy for patients with dyspepsia such as is done in China and Japan where a lot of gastric malignancy is seen and treated. Limitations of finance should be ameliorated with National Health Insurance and such a scheme has flagged off in Nigeria. It is hoped that efficient and just execution of this national health scheme will benefit millions of low-income earners to have access to prompt diagnosis and speedy treatment. Conclusion Prompt recognition through effective awareness campaigns for screening and yearly full physical examinations for adults, accurate diagnosis and early intervention will go a long way in developing countries to ameliorate this potentially surgically curable disease. References
The following images related to this document are available:Photo images[hs11020f1.jpg] [hs11020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}