 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 163 - 170 Clinical and prognostic features of patients with pandemic 2009 influenza A (H1N1) virus in the intensive care unit*Sertogullarindan B1, Ozbay B1, Gunini H2, Sunnetcioglu A1, Arisoy A3, Bilgin HM1, Mermit Cilingir B1, Duran M1, Yildiz H4, Ekin S5, Baran AI6 1Department of Pulmonary and Critical Care, Medical Faculty of Yuzuncu Yil University, Van, Turkye *Correspondence author: Bunyamin Sertogullarindan Department of Pulmonary and Critical Care Medical Faculty of Yuzuncu Yil University YYU Tip Fakultesi Arastirma Hastanesi 65100- Van, Turkye Tel: +904322164711 (6135) Mobile: +905053878238 E-mail: bunyaminsert@hotmail.com Code Number: hs11026 Abstract Objective: To investigate the clinical and prognostic features of patients admitted to intensive care unit (ICU)
with pandemic 2009 influenza A (H1N1) virus.
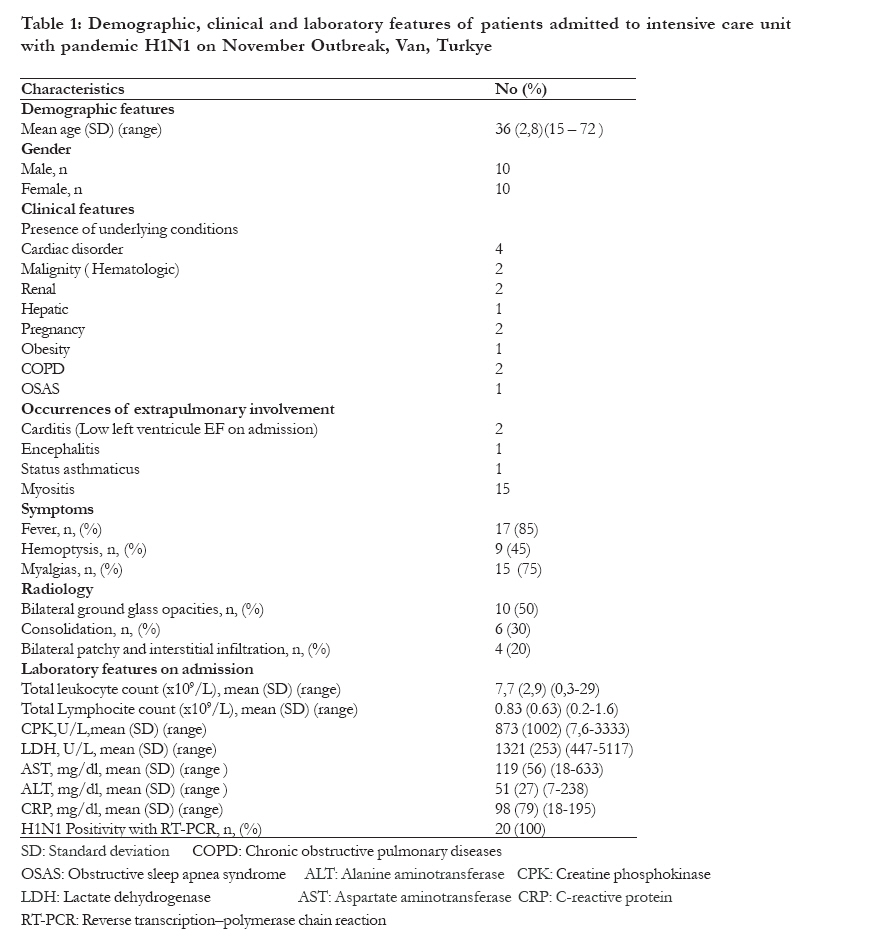
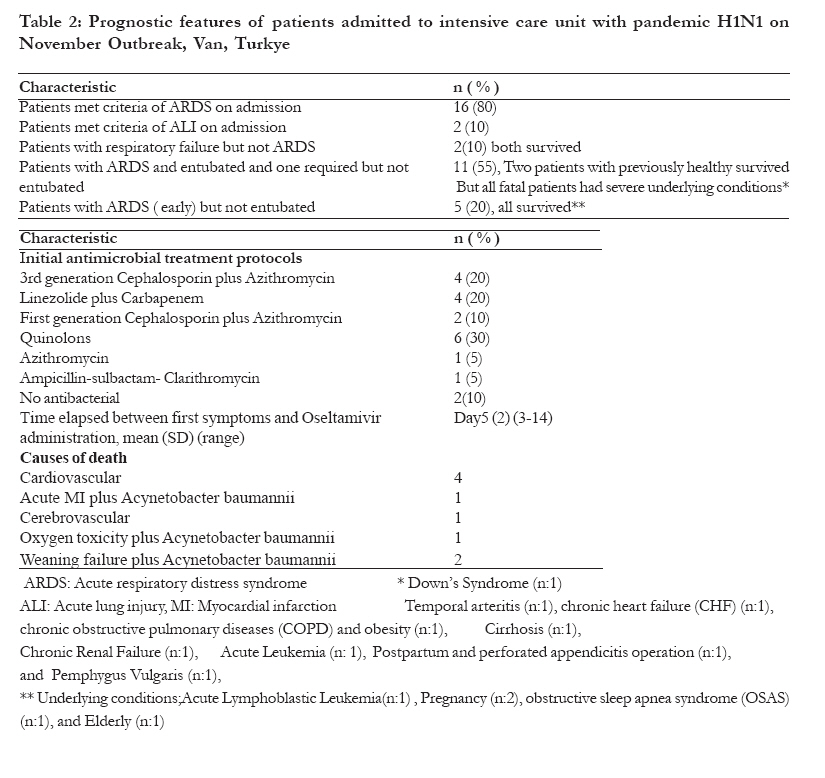
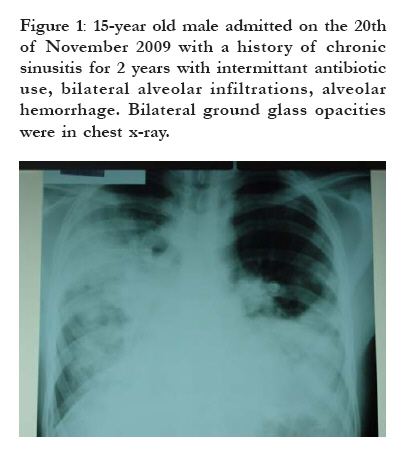
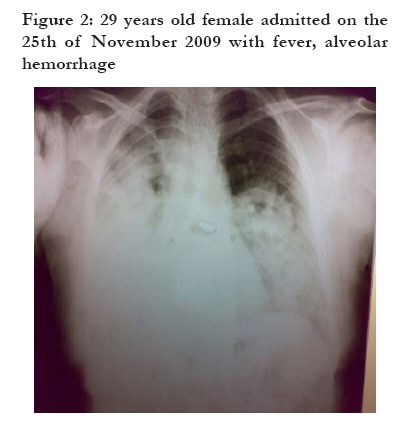
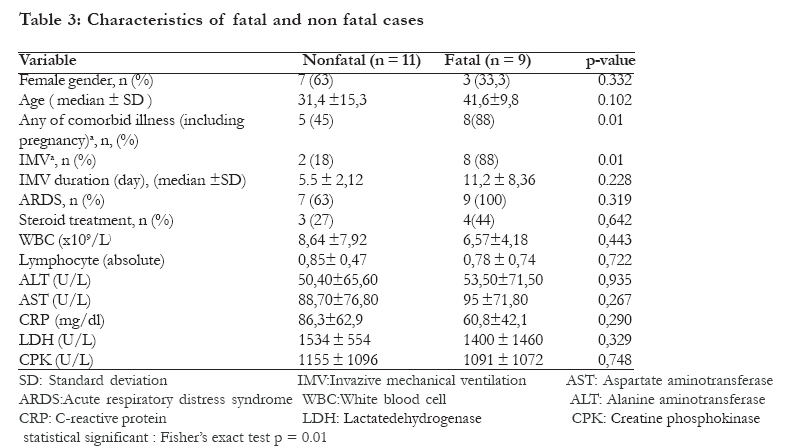
Key words: Pandemic 2009 influenza A (H1N1), intensive care unit, prognosis Introduction The new swine-origin pandemic 2009 influenza A (H1N1) virus has been identified as the cause of an outbreak of respiratory compromises throughout the world1, 2. Outbreak has reached to Turkiye in October, intensified in November, sustained in December 2009 and ended in January 2010. We have hospitalized severe community-acquired pneumonia (CAP) cases in the pulmonary ICU. The Ministry of Health of Turkye announced more than 600 deaths during the last influenza outbreak in Turkiye3. Although most patients presented mild and self-limited symptoms with no sign of pulmonary involvement, some people required admission to an ICU and received maximal life support measures4-5. Previous studies from Mexico and the United States reported that a prominent clinical feature of pandemic 2009 influenza A (HlNl) virus infection was severe CAP among patients6-7. Therefore, after the beginning of the outbreak in Mexico we took steps to deal with requiring bed capacity and ventilator capabilities for severe clinical patients. Previously researches reported that longer interval from onset of symptoms to treatment, concurrent underlying conditions, such as pregnancy, chronic respiratory illness, diabetes, obesity were related the severity of illness. In this article, we aimed to describe the clinical, laboratory and prognostic outcomes of the patients with pandemic 2009 influenza A (H1N1) virus and respiratory failure. Methods Setting The Department of Pulmonary and Critical Care of the Tertiary referral University Hospital has 6 beds in the pulmonary ICU and 19 beds in the clinical ward. The critically ill patients refer to this hospital. Patients This study was designed as a prospective observation. Patients were located in a city in the eastern part of Turkiye with a population of nearly 1 million, in November and December 2009. In this study, we only investigated cases requiring ICU due to severe CAP. Data Collection The study population consisted of ICU requiring cases having respiratory failure caused by severe CAP. The diagnosis of CAP were made by the presence of infiltrates on chest x-ray and at least two of the following symptoms; fever, cough and sputum. Chest x-ray was conducted for all patients on admission and during the course of the disease. The patients were screened for pandemic 2009 influenza A (H1N1) virus. Naso-pharyngeal swabs and, when appropriate, the deep tracheal aspirates for virological tests were obtained from all patients on admission in a standardized fashion. Samples were sent to Turkish National Institute of Health Ministry for RT- PCR detection of pandemic 2009 Influenza A (H1N1) virus. Patients were subjected to diagnostic tests for blood cultures, sputum samples for gram staining and culture, arterial blood gas analysis, biochemistry and complete blood count (CBC) tests on admission. Deep tracheal aspirates were used to obtain specimens from entubated patients. Demographic, clinical, laboratory, radiologic, medical historical data and prognostic characteristics were recorded. Underlying conditions of the patients were obtained from their referral forms or parents. Respiratory failure were classified into three groups that are ARDS, acute lung injury (ALI) and neither ARDS nor ALI. The diagnosis of ARDS and ALI followed the American-European consensus conference8. Patients were defined as ARDS if fulfilling the following requirements: (i) PaO2/FiO2 was 200 or less, (ii) a chest radiograph with bilateral pulmonary infiltrates compatible with pulmonary edema; (iii) no clinical evidence of congestive heart failure. Patients were defined as ALI if fulfilling the following requirements: (i) PaO2/FiO2 was 300 or less, (ii) a chest radiograph with bilateral pulmonary infiltrates compatible with pulmonary edema; (iii) no clinical evidence of congestive heart failure. The study subjects who met at least 1 of 2 major severe criteria (invasive mechanical ventilator, septic shock with the need for vasopressors) or 3 of 9 minor severe criteria (respiratory rate > 30/min; PaO2/ FiO2 <250; multilobar infiltrates; confusion and/or disorientation; uremia, blood urea nitrogen (BUN) > 20 mg/dL; leucopenia, leukocyte count < 4 x 10 cell/L; thrombocytopenia, platelet count < 100 x 109/L; hypothermia, core temperature < 36°C; hypotension, systolic blood pressure (SBP) < 90 mmHg) at the time of hospital admission were defined as ICU requiring CAP. We defined the variable "underlying conditions" as referring to cardiac, renal, and hepatic disorders, malignity (hematologic), pregnancy, chronic obstructive pulmonary disease (COPD), obstructive sleep apnea syndrome (OSAS), and obesity. Statistical analysis Descriptive statistics of the patients were performed and reported in terms of mean ± standard deviation (SD) and range for the quantitative variables, and in terms of absolute frequencies and percentage for the qualitative variables. Comparisons of the clinical characteristics and laboratory test results between the fatal and nonfatal cases were analyzed. The differences between independent groups regarding continuous variables were evaluated by Student's t-test. Nominal data were analyzed by Pearson's Chi-square test or Fisher's Exact test, where appropriate. Data were considered to be statistically significant, if the p values were less than 0.05. Results From November to December 2009, 49 adult patients were admitted to medical wards and 20 patients to the intensive care unit in the University Hospital. A characteristic feature observed in this outbreak was an increase in severe pneumonia cases requiring ICU. The main demographic features of 20 patients cared in the ICU are summarized in Tables 1 and 2. The ages of the patients ranged from 15 to 72 years (36 ± 13). Seventeen (85 %) patients were less than 50 years of age. The ratio of males to females was found to be 1:1. Most patients had complained of a fever (n = 17, 85%) and myalgias (n=15, 75%). Hemoptysis was developed in nine of the 20 patients (45 %). Of the 20 subjects, 17 (85 %) had underlying conditions (such as diseases, pregnancy or obesity). At the time of admission, pathogens were not identified from sputum and blood cultures. Of the 20 subjects, 3 (15 %) had leukocytosis and 2 (10 %) had severe leukopenia (400 and 300 per mm3) and 3 had mild leukopenia (3200, 2600, 1000 per mm3). Sixteen patient had lenfopenia (<1000 per mm3). The most frequent evidence of systemic inflammatory response was myositis associated with muscle involvement in 15 (75 %) patients. The elevated levels of C-reactive protein, lactate dehydrogenase, and aspartate aminotransferase were also observed in almost all patients. Of the 20 patients, 11(55 %) were discharged and 9 (45 %) were died. ARDS was diagnosed in 16 patients (80 %). Five patients (25 %) who had ARDS criteria and did not receive IMV. The median time from the onset of illness to initiation of oseltamivir treatment was 5 days (ranged, 2-7 days). Over-all patients received oseltamivir therapy at a dosage of 75 mg twice a day for 5 days. Two patients with non-severe CAP received no antibiotics. All patients had pneumonic infiltrations in their chest roentgenograms (Figures 1, 2). Oseltamivir (2x150 mg for 8 days) was started on the 7th day of the symptoms. Penicilin was started but then stopped after 2 days due clinical deterioration. Then linezolide, piperacillin and tazobactam were given for 8 days. Filgrastim (30 MIU) was given once for leukopenia. Due to ARDS 12cmH2O PEEP was required. Methyl prednisolone (40 mg/day) was given for 5 days. The patient was entubated on the 22nd of November and extubated on the 25th of November. He was discharged on the 1st of December. H1N1 was positive on RT-PCR assay. Bilateral ground glass and left lower consolidation were seen on chest x-ray. Due to ARDS 15 cm H2O PEEP was required. Oseltamivir (2x150 mg) was started on the 14th day of the symptoms. Linezolid (2x600 mg) was given for 7 days and methyl prednisolon (60 mg/day) for 5 days. The patient was entubated on the 25th of November and extubated on the 3rd of December. VAP was considered due to fever and tachypnea and piperacillin-tazobactam and amikacin were started. She was removed from ICU on the 7th of December and discharged on the 14th of December. While H1N1 was negative for nasopharyngeal swab taken on the 25th of November, it was positive for nasopharyngeal swab taken on the 4th of December in spite of treatment with oseltamivir for 10 days. She was readmitted on the 3rd of March 2010 with alopecia and malar rush otherwise healthy. All patients had positivity RT- PCR for pandemic 2009 influenza A (HlNl) virus. RT-PCR was negative on admission in one patient with ARDS, but in the 9th day it was found positive despite of oseltamivir administration. Characteristics of fatal and nonfatal cases are summarized in table 3. Between fatal and nonfatal cases mechanical ventilation rates and underlying conditions rates were different (p=0.01). No significant differences were found between the fatal and nonfatal cases with respect to sex, age, CBC and biochemistry values, steroid therapy, symptoms, and respiratory failure. The duration of mechanical ventilation in the 8 fatal cases (median, 11,2 days; range, 2-26 days) tended to be longer than that for the 2 survivors cases (median, 5,5 days; range, 4-7 days), although no significant difference was found between the two groups. Eleven (% 35) patients received steroids as part of their treatment with a 27 % rate of mortality (3 patients). Mortality rate was found higher (66 %) in the patients who did not received steroids. But this was not significant (P > 0.05). The most frequent causes of death were underlying conditions such as cardiovascular diseases and ventilator associated complications such as VAP associated with Acinetobacter baumannii. Discussion In the present study, we reported the clinical manifestations and outcome of 20 adult ICU requiring CAP cases with pandemic 2009 influenza A (H1N1) virus infection in Eastern Turkey during November and December 2009. Different mortality rates have been reported from different countries although it had a common characteristic of rapid spread in the community. High mortality rates were reported in Mexico, Ukraine, Turkey, Greece and Africa1,2,3,9,10. However, mortality rates in North America, English speaking countries and Japan were lower compared to the rates in the other countries11,13. One of the most important reasons of this could be the use of prophylactic antibiotics instead of antiviral agents in influenza-like diseases in developing countries, which may lead to severe community acquired diseases. Many studies reported that oseltamivir therapy is associated with survival in hospitalized patients with influenza pneumonia14,15. A study reported that the median interval from onset of symptoms to initiation of oseltamivir therapy was 2 days (13) for community cases, 4 days (26) for patients admitted to hospital and 6 days (49) for those admitted to an ICU [14]. In the current study and in the influenza pneumonia cases in Mexico and South Africa, the time between the beginning of the symptoms and the use of oseltamivir therapy was fifth day or later. We consider that this late initiation of oseltamivir treatment might cause high mortalty. However, some reports suggested that even it initiates late, antiviral treatment can reduce mortality, and national guidelines recommended that all hospitalized patients with pandemic 2009 influenza A (H1N1) virus infection should be treated with a neuraminidase inhibitor at a standard dose (75 mg every 12 hours) as soon as possible, regardless of when symptoms started16,17. We were successful in two cases where only oseltamivir was administered in patients with viral pneumonia in no more than one lobe. We also started oseltamivir treatment in a pregnant assistant doctor working in the outpatient clinic within 24 hours of the beginning of severe influenza symptoms. She had a significant clinical improvement and the symptoms disappeared in a short time. A similar event reported from Mexico. All of the 22 Mexican health workers with acute influenza symptoms had improvement after oseltamivir treatment18 showing the importance of early oseltamivir treatment. It was reported that although the virus was more common in the young, it was moreeffective in the elderly, the obese people, the pregnant women and the patients with underlying diseases. The case-fatality rates in those older than 50 years in Mexico, Spain, the United States and Greece were faster than those under 50 years15,18,19,20. Our results were consistent with this. However comorbidity may contribute to elderly patient's mortality. It was reported worldwide that 60 or 80 % of fatal cases older than 50 years had underlying diseases15,20. In our all fatal cases the patients had an underlying disease. Many studies have reported that the obesity is a risk factor for severe influenza diseases15,20. We had two obese patients. One of them had COPD and the other had OSAS. One of the obese patients showed improvement in his ARDS but died of cardiac ischemia. This condition suggests that obesity causes cardiovascular, pulmonary and metabolic diseases and thus it has been a relation severe CAP and mortality. The cumulative incidence of pandemic 2009 influenza A (H1N1) virus among Canuck pregnant women during the 2009 pandemic were estimated 8.6 % (24). A study from California was reported that 20 % of hospitalized pregnant women underwent ICU15. Similarly, a study from India reported that there were two pregnant cases among their 16 mortal cases22. But a report from Singapore noted the absence of any mortality from Influenza A/H1N1 in pregnant females23. Of more than 600 deaths in Turkiye, 40 were pregnant or postpartum females. Of our cases two pregnant women with ARDS and early ARDS have survived, but a pregnant woman with acute lung injury within postpartum thirteen day died. These different results may occur due to their time of admission to hospital and treatment of oseltamivir. Bacterial co-infection, especially in particular Staphylococcus aureus (SA) pneumonia is an important contributor to morbidity and mortality during influenza pandemics and during periods of seasonal influenza activity in inter-pandemic periods24-28. A study has reported that 252 patients with pandemic A (H1N1) 2009 influenza virus infection were admitted during the 3-month period of study. From these cases, 3 CAP cases of co-infection with pandemic 2009A (H1N1) influenza virus/meticilline resistance Staphylococcus aureus (MRSA) pneumonia co-infection were identified. In addition, 2 CAP cases of pandemic 2009 A (H1N1) influenza virus/meticilline resistance Staphylococcus aureus co-infection were identified at post-mortem examination during the same time period29. Of our cases, in a pregnant woman, entubation would have been undertaken (rapidly progressive bilateral alveolar consolidated round infiltrates, PaO2 / FiO2 under 200, hypoxemia, tachypne with a 40 to 50 respiratory rates per minute). This pregnant woman surprisingly showed prominent improvement within 3 to 4 hours after initialization of linezolide as anti-MRSA treatment. Likewise, an elderly man also rapidly improved in the same time after linezolide and meropenem administiration. From these cases it is suggested that an antibiotic treatment including meticillin-resistant bacteria should be started immediately in the patients showing rapid progress and not responsive to neuraminidase and prior empiric antibiotherapy treatment. We can save patients with early ARDS byobserving the effect of the treatment including antibiotics against meticillin-resistant Staphylococcus to avoid mortal VAP without requiring IMV. ARDS is one of the common causes of death and IMV in these patients5,22. But in current study between fatal and nonfatal cases ARDS rates was not different. IMV strategies must be suitable for these patients.Cardinal symptoms of the patients in this cohort study were fever, myalgia, and most importantly hemoptysis since it may be a sign of alveolar hemorrhage. Cough, sputum, and dyspnea are also well known and common symptoms of patients with severe CAP2,15,18. The ICU mortality had been reported different countries different each other. A study from Mexico reported eighteen patient with CAP were treated in ICU due to pandemic 2009 influenza A (H1N1) virus, ten (55 %) of them died2. In another study from Mexico, seven (58 %) of the twelve patients requiring IMV in ICU died18. In Greece, of the 294 ICU patients, 241 (81 %) underwent IMV, and 140 (47 %) died10. In California, of the 279 cases, 193 (65 %) required IMV, and overall mortality was 118 (42 %)15. As it can be seen, in these patients the intensive care unit mortality rates are high although they differ from each other. Therefore, early diagnosis and early oseltamivir treatment is important in these patients. Mortality rate was found higher in the patients who did not receive steroids, but this was not significant (P > 0.05). However, the prognostic effect of steroid use is difficult since most of the patients receiving steroid and the survivors had no serious underlying conditions. In our study, 3 of the 10 IMV fatal cases were complicated with VAP caused by A. baumannii. This situation is often found in patients requiring IMV9,30. Therefore, measures must be taken for VAP in patients undergo IMV. Conclusion During the pandemic 2009 influenza A, 20 adult patients mostly with identifiable risk factors became ill with severe pneumonia and managed in our intensive care unit with a 45 % of mortality rate. Early diagnosis and prompt antiviral treatment in people with influenza like symptoms such as fever, myalgia, and dyspnea seem to be the best approach to avoid serious illness caused by the Influenza virus. Special attention should be given to patients having underlying diseases such as cardiovascular and pulmonary diseases and conditions such as pregnancy. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11026t1.jpg] [hs11026f2.jpg] [hs11026t2.jpg] [hs11026f1.jpg] [hs11026t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}