 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 266 - 270 Factors affecting quality of life in cancer patients undergoing chemotherapy *Heydarnejad MS1, Hassanpour Dehkordi A1, Solati Dehkordi K 2 1Tehran University of Medical Science, Tehran Nursing Faculty, Tehran,
Iran *Correspondence author Ali Hassanpor Dehkordi Tehran University of Medical Science Tehran Nursing Faculty Tehran, Iran Ph & Fax: +98 9133830205 E-mail: ali_2762002@yahoo.com Code Number: hs11041 Abstract Background: Cancer can produce many different symptoms, some subtle and some not at all subtle. An
increasingly important issue in oncology is to evaluate quality of life (QoL) in cancer patients. The cancer-specific QoL is related to
all stages of this disease.
Keywords: Cancer, Chemotherapy (CT), Quality of life (QoL), Solid tumors. Introduction The term quality of life (QoL) is used to evaluate the general well-being of individuals and societies. According to the World Health Organization (WHO), quality of life (QoL) defined as individual perception of life, values, objectives, standards, and interests in the framework of culture. A number of illness-related factors exist that can affect QoL. The amount of symptoms distressed experienced by an individual has been related to QoL in a number of people with cancer. QoL is increasingly being used as a primary outcome measure in studies to evaluate the effectiveness of treatment1-4. Patients generally instead of measuring lipoprotein level, blood pressure, and the electrocardiogram, make decisions about their health care by means of QoL which estimates the effects on outcomes important to themselves5. An increasingly important issue in oncology is to evaluate QoL in cancer patients6. The cancer-specific QoL is related to all stages of this disease7,8. In fact, for all types of cancer patients general QoL instruments can be used to assess the overall impact of patients' health status on their QoL; however hand cancer-specific instruments assess the impact of a specific cancer on QoL6. In some cancer diseases (glioma for instance), QoL has become an important endpoint for treatments comparison in randomized controlled trials so that in these patients clinical studies increasingly incorporate QoL as endpoint9. Cancer can produce many different symptoms, some subtle and some not at all subtle. Some symptoms of cancer affecting QoL in patients would be cancer type and stage, as some types of cancer do not present any symptoms until they are in advanced stages, time since diagnosis, patient acceptance, intensity of the disease and the level of psychological distress experienced by caregivers. The main problems of long-term cancer survivors are in the areas of social/emotional support, health habits, spiritual/ philosophical view of life, and body image concerns10-13. Many studies show good or adequate overall QoL in these patients. However, among long-term survivors, psychosocial issues and physical symptoms such as pain and lymphedema, particularly the adverse effects of systemic adjuvant therapy (chemotherapy) on QoL still persist11-14. The aim of this study was to evaluate the QoL in cancer patients with solid tumors and at the different chemotherapy cycles. Methods This study was a cross-sectional. A total of 200 cancer patients were included in the present analysis. The study was conducted in Tehran hospital. Before being asked the subjects to participate and fill out QoL questionnaire, a formal consent was obtained from all of them. If the following criteria met by the patients15, then they were invited to participate:
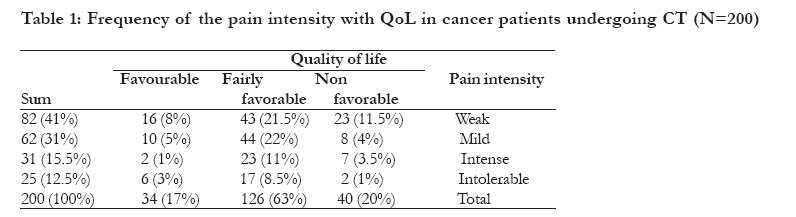
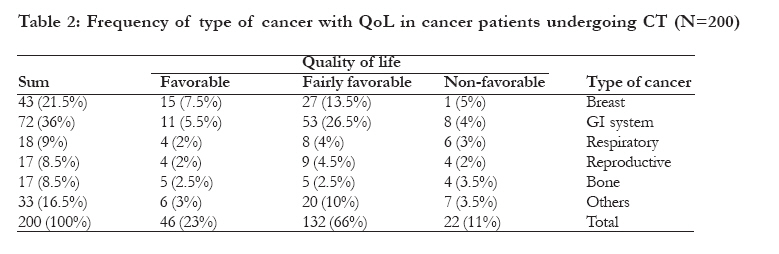
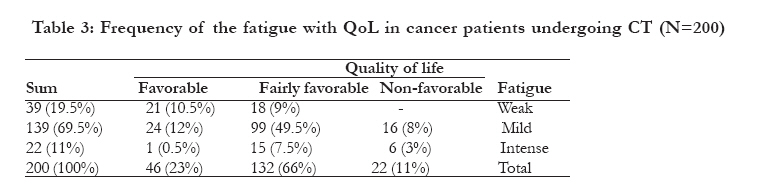
With some modification, the European Organization for Research and Treatment of Cancer QoL Questionnaire (EORTC QLQ-C30) was used to measure QoL in the patients. The test consisted of 56 questions and had arranged into 5 domains (Table 1): (a) physical, role, cognitive, emotional, and social functioning demographic data as well as cancer/treatment information (b) patient's general conditions (c) patient's physical activities (d) social status and occupational function and (e) sleep pattern. With the aid of a nurse and/or a medical student, the questionnaires were filled out during interview. Each question had an equal value and the QoL was quantified as the sum of the scores for all domains. The scores were classified into three categories, namely favorable, fairly favorable, and favorable. The higher scores on this scale represent a better QoL. The chi square test was used to find the correlation of the clinical variables and QoL scores using the SPSS software (version 14). The level of significance was set at p < 0.05 for all tests. Results The quality of life was lower in the patients with pain compared to those had no pain (Table 1). In addition, statistical analyses indicated that there was a significant relationship between the pain intensity with reducing or losing body performance and QoL (P <0.05). The majority of patients (54.5%) were male, aged 18-75 years, with a mean age of 46.2 (650%), unmarried (44%), primary school graduates (65%), and had not sufficient income (79.5%). The relationship between cancer type and QoL is depicted in Table 2. GI (gastrointestinal) cancer at the stage III was the most common cancer, accounting for 35-40% of all the patients. Most of the patients (85%) were aware of their disease. Findings about QoL in the rest of four domains depicts that the most common problems in regard to this category were: fear about future (29%), thinking about the disease and its consequences (26.5%), impatient (24%), and depression (17.5%). The QoL was fairly favorable in majority (66%) of the patients. There was no correlation between the QoL and variables such as age, sex, marital status, duration of disease, economic conditions, and occupational function. Furthermore, no correlation was found between QoL and the patients' educational level (literate or illiterate). Table 3 shows relationship between fatigue and QoL in cancer patients undergoing chemotherapy. Patients with low fatigue had better QoL than the others and in fact chi square test showed a significant relationship between the fatigue and QoL in cancer patients undergoing chemotherapy. The relationship between QoL and the number of CT cycles shows that majority (66%) of the patients had fairly favorable QoL. A strong correlation was found between QoL and number of CT cycles. Nevertheless, significant difference was found between the level of QoL in patients with < 2 CT cycles and/or with 3-5 cycles (p< 0.001). This was the case also for the level of QoL in patients with e" 6 cycles (p< 0.001). Discussion An important issue in cancer care and research is QoL. The QoL refers to "global well-being," including physical, emotional, mental, social, and behavioral components. In the last few years, a number of informative and valid QoL tools have become available to measure health-related QoL6. The most widely applicable instrument to measure the QoL in cancer patients is the EORTC QLQ-C30. Using this method, the current study assessed the QoL in cancer patients undergoing CT. Several studies support our findings on the influence of CT on good or adequate QoL among the cancer patients undergoing CT1,2. For instance Nematollahi showed in patients suffering from lymphatic tumors that there was a positive correlation between CT and QoL1. Likewise, the QoL of African American women with breast cancer was found to be relatively high; cancer recurrence and metastasis to the lymphatic glands had significant effect on the QoL17. It has also been shown that CT had a measurable adverse effect on QoL in women with node-positive operable breast cancer18. The results of our study indicate that CT may improve the QoL in cancer patients. Nowadays QoL has been introduced as an endpoint for treatment comparisons in many cancer types, particularly in advanced stages19. QoL also, as an early indicator of disease progression could help the physician in daily practice to closely monitor the patients20. QoL may be considered to be the effect of an illness and its treatment as perceived by patients3 and is modified by factors such as impairments, functional stress, perceptions and social opportunities4. As reducing mortality and ensuring optimal health-related QoL are perhaps the main objectives of medical care10, this study shows that improvement of QoL in cancer patient can be carried out by means of CT. In fact, improving QoL is as important as the survival benefit that a pharmacological treatment may provide. However, this is not always the case. For example, Nemati et al21 reported that the level of QoL in the patients with leukemia was 87.5% lower than that in the control group. The differences might be due to different patients' population (sample size or patient age), or cancer types. The current study selected patients (aged > 18 years) with various solid tumors while Nemati et al21 sampled 40 adolescence patients (aged < 18 years) with leukemia. In this study, the majority of the patients (68%) who had completed 3 or more cycles of CT reported a fairly favorable or favorable level of QoL. This may show that QoL is directly related to cancer treatment procedure, i.e. CT. Likewise, except for a small group (13.3%) of the patients that their sleep pattern was not favorable, the others had good QoL. This implies that CT can lead to the better sleep pattern in cancer patients. Our results are consistent with other studies. For instance Chen et al15 found that QoL in lung cancer patients during the fourth cycles of CT improved slightly over the baseline values; the patients perceived more sleep disturbances during the early cycles of CT. Similar results have been found in patients suffering from advanced cancer by Mystakidou22 and from breast cancer by Fortner21. The findings of the present study show that there is no correlation between QoL and age, gender, social status, marriage, and job. Similar results have reported by Nematollahi16, Vedat et al.24, and Rustøen25 studies. Further, there were no correlation between extent of the disease and QoL. In contrast, Rustøen25 and Holzner26 in two separate studies found that the extent to which QoL of cancer patients depends on the time elapsed since initial treatment; with an increase in the extent of the disease, a decrease in the QoL was observed. The difference might be due to the duration of disease; the extent of the disease in 87% of the patients of the current study was less than two years whilst it was more than 2 years in Rustøen25 and Holzner26 studies. Conclusion Cancer is an important health issue influencing QoL. An appropriate treatment which may provide care to the cancer patients is CT. The obtained results here indicate a strong correlation between QoL and number of CT cycles in cancer patients. Since CT is socially stigmatized in some countries e.g. Iran, encouraging patients to complete a CT course might play an important role in the treatment outcome and the QoL in cancer patients. Acknowledgement The authors would like to thank the staff members of radiation oncology departments in Tehran University of Medical Sciences. We also thank Iranian National Elite Foundation (Bonyad) and Mr. A. Mehran for his statistical consults. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11041t2.jpg] [hs11041t1.jpg] [hs11041t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}