 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 290 - 295 5 year old girl with malignant lymphoblastic lymphoma: Challenges of managing haematological malignancies in a developing country Amiwero C1, Okuku G1, Adeboye N2, Aina O3 1Department of Haematology and Blood Transfusion, Federal Medical Centre, Bida, Niger state, Nigeria *Corresponding author Dr. Christian Amiwero Department of Haematology and Blood Transfusion Federal Medical Centre Bida, Niger state Nigeria +234 80 75848871, +234 8058697855 E-mail: dramiwero@yahoo.com Code Number: hs11046 Abstract Background: Lymphoblastic lymphoma (LBL) is a neoplasm of lymphoblasts. The condition is predominantly
lymph nodebased disease arising from immature T cells in 85-90% of cases and immature B cells in the remainder. The
lymphoma is aggressive, progresses rapidly, and often presenting as stage IV disease in more than 70% of patients. This disease
makes up approximately 20% of childhood NHL
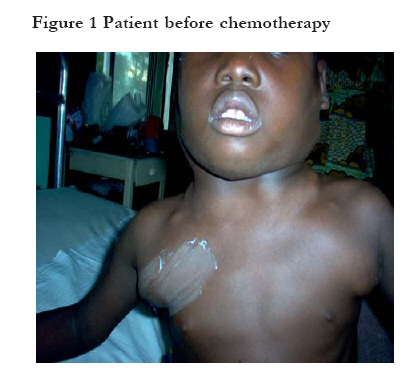
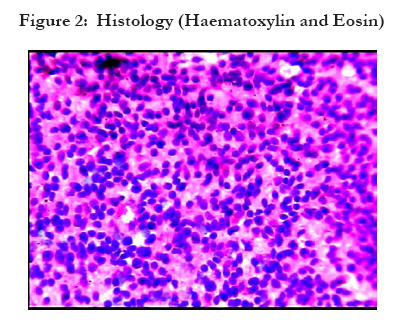
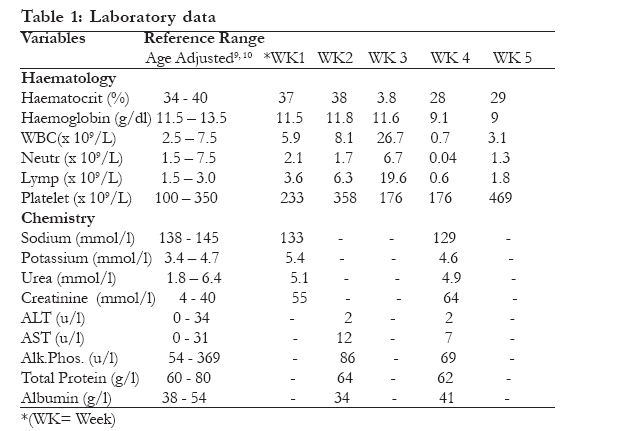
Key words: Haematological malignancies, management, constraints, developing countries Introduction Lymphoblastic lymphoma (LBL) is a neoplasm of precursor T and B cells, or lymphoblasts. The condition is predominantly lymph nodebased disease arising from immature T cells in 85-90% of cases and immature B cells in the remainder.1,2 The lymphoblasts infiltrate nodal structures or extranodal structures, especially the bone marrow, spleen and central nervous system (CNS).3,4 Lymphoblastic lymphoma is aggressive and progresses rapidly, presenting as stage IV disease in more than 70% of patients.1 In 30-50% of patients, the lymphoblasts infiltrate bone marrow, causing ineffective haematopoiesis. This disease makes up approximately 20% of childhood NHL5,6, Lymphoblastic lymphomas are usually positive for terminal deoxynuleotidyl transferase (TdT), with more than 75% having a T-cell immunophenotype and the remainder having a precursor B-cell phenotype.6 However, the management of this highly aggressive malignancy in the developing countries such as Nigeria is still a daunting task to their health care providers, with attendant short survival and high mortality among the patients. Using the current treatments, the overall survival rate at 5 years in children with lymphoblastic lymphoma is 80-90%.7 Many current routine diagnostic procedures as well as chemotherapeutic agents for haematologic malignancies are available for the management of patients in the developed countries. The application of specialized regimens with CNS prophylaxis, is a gold standard in the management of patients with highly aggressive lymphoblastic lymphoma.8 The aim of this case report is to highlight some of the limitations faced by specialists in management of patients with lymphoblastic lymphoma while emphasizing the implications for patients. Case Report A 5 year old girl presented at the Federal Medical Centre, Bida, Nigeria with 3 months history of generalized lymphadenopathy, weight loss, night sweats and intermittent low grade fever. There was no significant finding on systemic review. General examination revealed a chronically ill-looking young girl, with low grade pyrexia (Temp-37.8oc), no clinical evidence of anaemia or jaundice, had generalized lymphadenopathy involving the following groups of lymph nodes: cervical, (8cm x 6cm); Axillary, (6cm x 4cm); Inguinal, (4cm x 4cm). The lymph nodes were discrete, firm and mobile. Abdominal examination showed hepatomegaly (liver span; 14cm), spleen and kidneys were not palpably enlarged. Baseline ancillary plus diagnostic investigations included: full blood count (FBC), erythrocyte sedimentation rate (ESR), serum electrolytes, blood urea and creatinine (E/U + Cr), liver function test (LFT), cerebrospinal fluid examination (CSF), bone marrow aspiration (BMA) / biopsy, fine needle aspiration cytology (FNAC), lymph node biopsy(LNB), chest x-ray (CXR), human immunodeficiency virus (HIV) screening, and abdominal ultrasound (ABD U/S). The initial white blood cell count (WBC) by the first week on admission was 5.9 x 109/L while absolute lymphocytes count (ALC) was 3.6 x 109/L. Both counts gradually increased, and by the third week, FBC investigations revealed leucocytosis (White Blood Cell count [WBC] = 26.5 x 109/L), and absolute lymphocytosis (Absolute lymphocyte count [ALC] = 19.6 x 109/L). There was no anaemia (Mean Haematocrit [PCV] = 0.34 ± 0.05) or neutropaenia (Mean absolute neutrophil count [ANC] = 2.4 ± 2.6 x 109/L) until a week after the commencement of chemotherapy, and all through this period, there was no thrombocytopaenia (Mean Platelet count = 282 ± 128 x 109/L). Blood film showed lymphoblasts with high nuclear-cytoplasmic (N:C) ratio, scant basophilic cytoplasm, open and lacy chromatin pattern. There were accompanying smear cells, and moderate eosinophilia on film. Bone marrow aspiration/biopsy revealed lymphocytic infiltration with preservation of other cell lines. Fine needle aspiration cytology of the cervical and axillary lymph nodes showed numerous populations of intermediate sized lymphoblasts. Histological examination showed the same morphological type. The essential finding in the abdominal ultrasound was that of an intra-abdominal para-aortic lymph node enlargement. Chest x-ray revealed hilar adenopathy, electrolytes, urea, creatinine, and liver function test results were within the reference ranges. HIV screening results was negative. Based on the above findings, a diagnosis of High grade, Non-Hodgkin lymphoma, lymphoblastic variant (International Working Formulation) stage IVB was made. Supportive management was offered using intravenous fluids (4.3 percent dextrose in 0.18 percent saline) to maintain the cardiovascular status, while intravenous cefuroxime a broad spectrum antibiotic at 15mg/kg every 12 hours was used empirically for presumed bacterial infections (in view of the pyrexia noticed at presentation) for a period of 7days. The reason for this choice of this broad spectrum antibiotic is that in view of the diagnosis and commencement of induction therapy there is a possibility of opportunistic infections resulting from depressed immunity. Initially the fever subsided, however after one week of chemotherapy it recurred. Intravenous cefuroxime using the same dosage as above was given in the fourth week for apparent neutropaenic sepsis (absolute neutrophil count was 0.04 x 109/L, with swinging temperature avg. 39.0oC). The treatment was given for 7 days, after which the mother requested for discharge. However she was counseled on her child's clinical condition, the options and use of cytotoxic agents as well as their possible adverse effect, first generation combination cytotoxic agents COAP (ALL Type- Regimen) for remission induction ( I.V Cyclophoshamide 650mg/m2 ( ÷ 455mg) days 1 and 8, I.V Vincristine 1.4mg/m2 ( ÷0.98mg) days 1, 8, 15, 21 and 28, I.V Cytosine arabinoside 100mg/m2 ( ÷ 70mg) days 1 to 7 and Oral prednisolone 40mg/m2 ( ÷ 10mg 8hourly) 1 - 28 )11,12 was commenced approximately three weeks after admission and after obtaining consent from her parents, and having satisfied the criteria (Absence of fever, packed cell volume à or = 25%, Absolute Neutrophil Count Ã1.0 × 109/L, Platelet Count à 75 × 109/L and normal liver function test table 2) for the commencement of the chemotherapy. 11 The chemotherapy dosages were based on the patient's surface area of 0.7m2 (height of 92cm, weight of 22kg). The COAP regimen is used either with intra-thecal methotrexate or cytosine arabinocide plus hydrocortisone and is the standard treatment for childhood aggressive lymphoma in Nigeria. The alternative regimens are ABVD(Adramycin, bleomycin, vinblastine and dacarbazine) and CHOP (Cyclophosphamide, Adramycin, vincristine and prednisolone)11, 12, 13 Allopurinol 50mg 8 hourly was administered for 7 days prior to induction therapy in an attempt to prevent hyperuricaemic nephropathy. The patient could not benefit from intra-thecal prophylaxis because the available chemotherapeutic agents were barely sufficient to complete the first course of the combination regimen. Due to financial constraints, the patient was allowed home on request after the completion of the intravenous doses of the cytotoxic agents. The high grade pyrexia had subsided with temperature remaining at 36.5oC at the time of discharge. The patient should have been re-admitted for the second cycle of chemotherapy (consolidation therapy) in the light of apparent good clinical response on day 29 of the chemotherapy; however, this was not possible due to financial constraints. It was for the same reason that we were unable to carry out a repeat bone marrow aspiration, and full blood count to assess haematologic remission or clinical remission. This hospital at which our patient was managed is a public facility used by anyone seeking medical attention. Therefore patients on admission are responsible for paying any bills that accrue during the process of receiving health care that ranges from bed fees, drugs to investigations including full blood count and bone marrow evaluation. Figures 1, 2, & 3, Table 1 Discussion Lymphomas are neoplastic proliferations of the lymphoid cell. As in this case, the lymph nodes are the sites most frequently involved with progressive lymphadenopathy.8 The diagnosis of malignant lymphoblastic lymphoma was arrived at by employing the technique of blood film, fine needle aspiration cytology (FNAC) and histological examination of the excised lymph node. The histology revealed diffuse monomorphic population of intermediate sized lymphoblasts composed of finely dispersed chromatin and scant cytoplasm. The nuclei are irregular in outline and the nucleoli are inconspicuous. The finding on bone marrow aspiration showing lymphoblastic infiltrations of less than 25% of the marrow nucleated cells justifies the classification of stage IV LBL in line with Ann-Arbor tumour staging.14 CSF cytology which in this case was negative for malignant pleocytosis suggesting non-involvement of the central nervous system however, prophylactic intra-thecal administration of cytotoxic (methotrexate or cytosine arabinocide plus hydrocortisone) would have been beneficial.12 It is essential to state that effective management of LBL revolves around the availability of modern techniques required for accurate and precise diagnosis as well as availability of affordable cytotoxic agents. The challenges faced by many hospitals are several fold and include the following: Establishing a diagnosis; the diagnosis and tumor classification in the index case were purely based on morphology due to lack of the necessary ancillary diagnostic facilities for specialized techniques like immunophenotyping, immunohistochemistry, immunoenzymatic technique, monoclonal antibody technique for cell surface antigens, and cytoplasmic antigens.14,15 Cell mapping allows for adequate tumor classification and thus places oncologists in a proper perspective in terms of the choices of management protocol, and prognosis.18 The provision of the above investigative procedures in our various institutions requires commitment on the part of the managers of the various hospitals, backed up by increased funding on the part of the government. This is a challenge begging for attention so that the medical personnel and other allied workers could begin to carry out some of these investigations considered as routine procedures in the developed countries. Treatment- In high grade non-Hodgkin lymphoma (LBL), the prognosis without treatment is very poor7,8, therefore aggressive combination chemotherapy is generally used. In contrast to low grade lymphoma, the early mortality of high grade lymphoma is extremely high but paradoxically those who go into remission may have prolonged disease-free survival and close to one third may be cured.7,8,16 Achieving this requires first, second or third generation chemotherapeutic agents. Unfortunately, availability and affordability of the first generation cytotoxic agents, is not general in developing countries. This unfortunate circumstance is undoubtedly forcing these patients, who might have hitherto benefited from these agents, to alternatives such as spiritualist or traditional healers / alternative medicine practitioners, and of course to early graves. It is therefore justifiable to advocate similar publicity and resources being offered to patients infected with human immunodeficiency virus (HIV) with the same measure of zeal, for thousands of patients frequently diagnosed with, and dying prematurely from primary malignant lymphoma conditions or lymphomas accompanying HIV/AIDS.17, 19 The social work departments in all hospitals need to be strengthened financially to enable them to perform their statutory role of welfare and social support, especially with regards to the management of cases of this nature. In this way, financial benefit could be extended to our patients who are usually from low socio-economic background.19 While it is true that a few tertiary institutions have in place the policy of patients' exemption from payment of all fees related to the management of malignant conditions; this is not true in many others, and in any case, where such policy exits, the drugs are often out of stock. The few locations where these drugs are available provide the opportunity, created by poor implementation of health policy, to exploit these patients.20 Concerted efforts from the government and non-governmental agencies in collaboration with pharmaceutical companies would go a long way to ameliorate the situation. Other stakeholders in the health sector should redouble their efforts to see how all of these essentials could be made more available at a subsidized rate in the country, with special emphasis on the tertiary institutions where these essentials are mostly utilized.21 Manpower- Adequate specialized manpower is needed in many hospitals. Training and re- training on newer techniques should be advocated for those involved in this sub-specialty. In spite of the aforementioned limitations and challenges faced by specialists in this part of the world, chemotherapy following only morphological diagnosis continues to be useful as indicated from this case. Recommendations According to World Health Organization (WHO), low income and medium income countries are hardest hit as compared to the developed countries yet their governments make little or no effort to ameliorate the additional burden of cancer. It is now time that all stakeholders critically look at revamping the ailing health sector in the developing countries by way of increased funding, providing up-to-date equipment and ensure implementation of health policy that could benefit cancer patients while ensuring strict compliance by all public health institutions. Conclusion Training and re-training of our medical personnel in the midst of various daunting challenges in our health centres will go a long way in alleviating the additional burden posed by cancer in the developing countries. Acknowledgements We thank Dr A. Adepoju and the entire staff of the department of Paediatrics, Federal Medical Centre, Bida, Nigeria for their various roles in the management of this patient. We are grateful to Professor Philip O. Olatunji of the department of haematology, Olabisi Onabanjo University Teaching Hospital, Ogun State Nigeria and Professor Robin Prescott of Medical statistic unit/Public Health Sciences Department, University of Edinburgh, United Kingdom for their various contributions to this piece of work. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11046f3.jpg] [hs11046f2.jpg] [hs11046f1.jpg] [hs11046t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}