 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 26-31 Clinical characteristics and risk factors for peripartum cardiomyopathy Huang GY1, Zhang LY2, Long-Le MA1,3, *Le-Xin Wang1,3
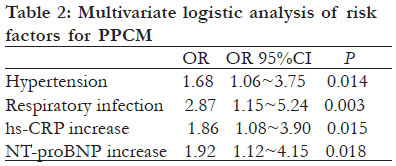
Abstract Background: Peripartum cardiomyopathy (PPCM) is a potentially fatal form of heart failure and the recognition of its risk factors is important for prevention and treatment. Key words: peripartum cardiomyopathy, inflammation, hypertension, C-reaction protein,mortality. Introduction Peripartum cardiomyopathy (PPCM) is an idiopathic cardiomyopathy presenting with heart failure secondary to left ventricular (LV) systolic dysfunction towards the end of pregnancy, or in the months following delivery, where no other cause of heart failure is found1. The left ventricle in patients with PPCM may not be dilated but the ejection fraction (EF) is nearly always reduced below 45%1. The exact cause of PPCM is unknown, but various viral infections, and autoantibodies have been implicated in the pathogenesis of this disease.1 In addition, advanced maternal age, multiparity, African descent, twin pregnancy, pregnancy-induced hypertension and long-time miscarriage are also found to be related to PPCM2,3. The reported prevalence of PPCM is highly variable, from 1 case per 6 000 live births in Japan, to 1 case per 1000 live births in South Africa, to 1 case per 350-400 live births in Haiti2,3. The usual causes of death are progressive heart failure, arrhythmia, or thromboembolism. A wide range of mortality rate due to PPCM has been reported. In the United States, a 15.9% two-year mortality rate was found among African American women, but a 3.3% - 9.6% mortality rate was reported in other studies4,6. The purpose of this study was to describe the clinical characteristics and risk factors for PPCM from a single medical center in the inland Shandong Province of China. Methods Patient population From May 2007 to May 2009, we prospectively analyzed patients with PPCM admitted to our hospital. It is a major tertiary teaching hospital providing services to an inland population of approximately 5.6 million people in Shandong Province, China. This study received approval of the institutional review board of Liaocheng People’s Hospital, and written informed consent was obtained from all participants. The diagnosis of PPCM is based on exclusion. The diagnosis for PPCM was suggested when patients presented with heart failure symptoms in late pregnancy or within the first five months postpartum1,7. Heart failure symptoms were verified by transthoracic echocardiographic examination, which showed a left ventricular EF of less than 45%1,7. Finally, other causes for heart failure and cardiomyopathy, such as pre-existing hypertension, coronary heart disease, heart valve disease, congenital heart disease, alcoholic cardiomyopathy and tachycardia-induced heart disease, had to be excluded. We also selected healthy women who had a normal delivery during the same period to be controls. The matching conditions included occupation, economic status, education and an age difference of less than 10 years. Echocardiography was performed in these healthy controls to verify left ventricular function. Clinical data collection A standard survey questionnaire (in Chinese) was used for the investigation of epidemiology and lifestyle of patients with PPCM and the control group8. The items in the survey included family history of PPCM, medical history (such as hypertension, diabetes, coronary heart disease, myocarditis, and infection), economic status, education, smoking and drinking history. Gestational hypertension or pregnancyinduced hypertension is defined as the development of new arterial hypertension in a pregnant woman after 20 weeks gestation. Multi-delivery was defined as two or deliveries. Laboratory tests Two-dimensional and Doppler echocardiographic studies were performed within 6 hours after admission by a cardiologist using ViViD7 cardiac ultrasound unit with a 2.5-MHz transducer (GE, PA, USA). Left ventricular ejection fraction (EF) was measured from the apical views by Simpson’s biplane method. The mean of three measurements was used. On the day of admission, blood samples were collected to measure high-sensitivity C-reactive protein (hs-CRP), cardiac troponin I, blood lipids and biochemistry profile. All blood samples were analyzed in the central laboratory of Liaocheng People’s Hospital. All tests were repeated before discharge and at the first follow up visit, which was two - four weeks after discharge. Treatment of heart failure All PPCM patients received standard therapies for heart failure during hospitalization, which were mainly loop diuretics and b-Blockers. Digoxin was also prescribed to patients with class IV of New York Heart Association (NYHA) function class. For postpartum PPCM, angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), were also administered. Statistical analysis Analysis was performed using SPSS 12.0 for windows. Absolute number and percentage were computed to describe the patient population. Data were expressed as mean ± SD for continuous variables. Analysis of variance was used for the comparison of the means of two groups. The chi square test was used for the comparison of rates between the two groups. Multivariate logistic regression analysis was performed to identify independent factors of PPCM. A p-value 0.05 was considered statistically significant. Results General findings Out of 18 000 women admitted to the obstetrics wards for child birth and follow up for up to five months, 52 (0.29%) met the diagnostic criteria for PPCM during the hospitalization. The general characteristics and laboratory test results of the patients and healthy control are listed in table 1. The age of the patients ranged from 19 to 38 years. Fortysix (88.5%) of the PPCM patients were farmers mostly with primary to high school education. The onset time of symptoms was 1-60 days after childbirth (median, 10 days). Seventeen (32.7%) of the patients experienced PPCM after delivery of the second child, and 34 (65.4%) patients received a cesarean section. In addition, 6 patients (11.5%) had gestational hypertension, whereas none of the control group subjects had gestational hypertension. The New York Heart Association (NYHA) function class IV, III and II, was found in 12(23.1%), 36(69.2%), and 4(7.7%), respectively. In patients with PPCM, bronchitis/ pneumonia was suspected in 19 (36.5%) due to clinical symptoms such as cough, fever (body temperature >37.5°C) and chest X-ray changes (increased markings or white patches in the lung fields). Six patients (10.9%) in the control group also had signs of respiratory infection but the mean body temperature was lower than in the study group (p<0.05, table 1). These patients were treated with antibiotics during hospitalization. Cesarean section wound infection was found in two. Thirteen of the patients (25%) with respiratory infection also had serum evidence of past viral infection, with positive ELLISA tests for Coxsackie IgG in eight and adenovirus IgG in five. The mean body temperature of the thirteen patients were slightly higher than the other 6 patients who had no positive IgG (38.7 ± 0.8 vs 38.4 ± 0.8, p>0.05). Twelve of the 13 patients with past viral infection received traditional Chinese anti-viral infection medicine Huang Qi (radix astragali) for a week. Risk factor analysis of PPCM As shown in table 1, compared with the control group, PPCM patients were older, with a higher blood pressure, a higher rate of gestational hypertension, and a higher rate of suspected respiratory infection. The white blood cells, cTNI, hs-CRP and NT-proBNP in the PPCM patients were also higher than in the control, whereas blood albumin level was lower. There was no significant difference in the rate of multi-delivery or cesarean section between the two groups. Multivariate logistic analysis on risk factors for PPCM Non-conditional logistic regression was conducted to analyze risk factors for PPCM. As shown in table 3, a higher systolic blood pressure (³ 140/90 mmHg), respiratory infection, increased hs-CRP (³ 9.0 mg/ L), and increased NT-proBNP (³ 450 pg/ml) were significant predictors for PPCM (table 2). Clinical outcomes All PPCM patients received standard treatment for heart failure, including ACE inhibitors or ARB, âblocker and loop diuretics. Twenty-six patients with NYHA class IV heart failure also received oral digoxin. Nine patients also received low-molecular weight heparin for thrombosis prevention during hospitalization. Average in-hospital days were 11.6±3.5 days. There was no mortality during hospitalization. Heart failure symptoms and signs were markedly improved in all patients before discharge. Patients were followed up in the outpatient clinic for 21.6±5.4 days (14-34 days). One patient died suddenly at home four weeks after being discharged from hospital. The cause of death was unclear but it was mostly likely sudden cardiac death due to heart failure. The other patients remained symptom free or with symptoms well under control. The results of blood pressure, of the follow up are shown in table 3. The levels of blood pressure, hs-CRP and NT-proBNP were at the end of the follow up were lower than the pre-treatment levels. At the end of the follow up the mean left ventricular EF was increased, and 16 (31.4%) had a left ventricular EF of >50%. There was no statistically significant difference in the left ventricular EF between the 12 patients who were treated with herbal medicine Huang Qi (radix astragali) and those who were not (48.4 ± 10.1 vs 48.9 ± 11.2). Discussion The PPCM is a unique cardiomyopathy which appears in pregnant women before or shortly after childbirth, being similar to dilated cardiomyopathy. This disease has a strong regional distribution pattern, being less common in European countries, but having a higher prevalence in West Africa1,2. Currently, the reported incidence of PPCM is about 1/350 to 1/15 000, the country with a high incidence is Haiti ; one lying-in woman has PPCM in every 350-400 cases.2 The prevalence of PPCM in China is unclear, but our screening of 18 000 women in the Liaocheng Hospital between 2007 and 2009 showed that about 0.29% women hospitalized for delivery suffered from PPCM. The cause of PPCM is unknown, and its pathogenesis is probably multi-factorial. Past studies found that risk factors of PPCM included advanced maternal age, multiparity, African descent, twin pregnancy, gestational hypertension and long-time miscarriage prevention2. Familial clustering and familial occurrences of PPCM have been observed, suggesting that genetic factors play a role in the pathogenesis of PPCM9. There is experimental evidence that unbalanced peri/postpartum oxidative stress is linked to proteolytic cleavage of prolactin into a potent antiangiogenic, proapoptotic, and proinflammatory factor. This may contribute to the pathogenesis of PPCM10. A recent proof-of-concept clinical trial showed that pharmacological blockade of prolactin with bromocriptine improved the condition of patients with acute onset of PPCM11. In addition, an elevated plasma concentration of tumor necrosis factor-á, C-reactive protein, interleukin-6 and FAS/Apo-1 in PPCM patients, suggests that abnormal immune activity and inflammatory mediators may play a role in the pathogenesis of PPCM12,13. In this study, hs-CRP, an indicator for chronic inflammation, was significantly higher in the PPCM group and multivariate logistic analysis showed hs-CRP as an independent predictor for PCCM. These results suggest that the chronic inflammation or pro-inflammatory cytokines may be involved in PPCM. Chronic and gestational hypertension has been considered as a risk factor for PPCM2,14,15. The high frequency of PPCM in some of the ethnic groups may represent the interaction of race with hypertension. Therefore, whether race per se is an independent risk factor for PPCM requires further investigation2. In the present study, the incidence of gestational hypertension in patients with PPCM was 11.5%, which was lower than the 43% reported by Elkayam et al, 4 but similar to the reported rate of 8% to 10% in the overall pregnant population16. Multivariate logistic analysis in our patients showed that hypertension was an independent predictor for PPCM. In the present study, 36.5% of the patients with PPCM had clinical evidence of respiratory infection, and 25% also had laboratory evidence of past viral infection. In the current analysis respiratory infection appears to be associated with PPCM. As the diagnosis of respiratory infection was difficult in the presence of congestive heart failure, the role of infection in the pathogenesis of PPCM in our patients remains unclear. Twelve of the thirteen patients with past viral infection were treated with radix astragali, an antiviral drug known as Huang Qi in Chinese. This drug does not seem to be related to PPCM, as its main chemical components are flavonoids and saponins17, none of which are known to cause cardiomyopathy or heart failure. Furthermore, at the end of the follow-up, the mean left ventricular ejection fraction in the Huang-Qitreated group was similar to those without Huang Qi treatment during hospitalization. A limitation of this study is that the outcomes of the patients were studied only during hospitalization and shortly after discharge (mean follow up time 21.6 days). Although only one patient (1.9%) died, probably of heart failure and other patients remained well, the long-term survival of PPCM in this population is yet to be determined. As PPCM was diagnosed after birth in all our patients, ACE inhibitors or ARBs were routinely used but it is important to note that these drugs are contraindicated during pregnancy. Hydralazine with or without nitrates are alternatives to ACE inhibitors or ARBs for heart failure during pregnancy.1 These drugs plus other conventional heart failure medications such as beta-blockers, diuretics and digoxin appear adequate in relieving the heart failure symptoms of PPCM. However, the long-term effect of these drugs on full recovery of left ventricular function is yet to be clarified. Conclusion In this single-center study, all PPCM occurred within weeks following delivery. Patients with PPCM were older, had a higher level of blood pressure, and a higher rate of suspected respiratory infection than in the controls. The level of hs-CRP, cTNI and NTproBNP were also markedly higher in the PPCM patients. Multivariate logistic regression analysis showed that hypertension and elevated hs-CRP were independent risk factors for PPCM. These results suggest that hypertension and inflammation may play a role in the pathogenesis of peripartum cardiomyopathy in our patient population. References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12005t3.jpg] [hs12005t2.jpg] [hs12005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}