 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
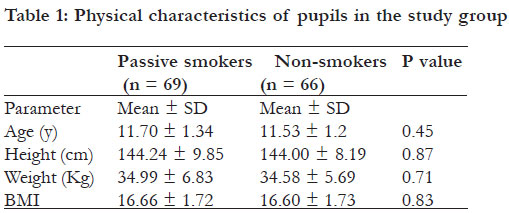
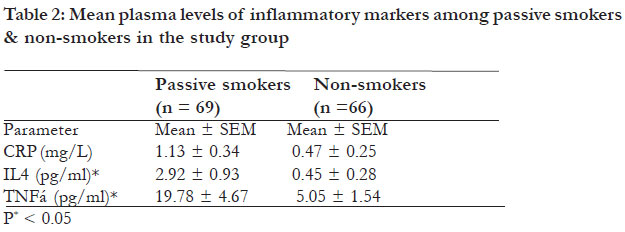
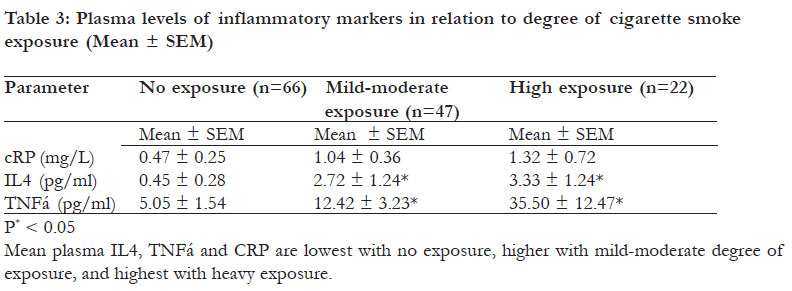
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 41-47 Changes in plasma IL4, TNFá and CRP in response to regular passive smoking at home among healthy school children in Khartoum, Sudan *Merghani TH, Saeed A, Alawad A Department of Physiology, Faculty of Medicine, University of Khartoum, Sudan Code Number: hs12007 Abstract Background: Regular exposure to tobacco smoke at home causes airway inflammation and altered cytokine regulation; however, there is variation between individuals of different countries. Key words: passive smoking, children, IL4, CRP, TNFa Introduction Tobacco smoke contains over 4 000 chemicals in the form of particulates and gases.1,2 Some of these have marked irritant properties and some are known or suspected carcinogens.1-3 Nicotine which is a weak alkaloid is the most addictive substance.4 It is absorbed from the airways to reach the brain in seconds.5 It acts on cholinergic receptors in the brain and other sites, causing release of dopamine, endorphins, and stress hormones that exert many effects in the body, including rise in heart rate and blood pressure.6,7 Tar, the particulate component of smoke without the water or alkaloid, contains many carcinogens, including polynuclear aromatic hydrocarbons, aromatic amines and N-nitrosamines.8 Carbon monoxide binds tightly to haemoglobin in red blood cells, causing reduction in the oxygen carrying capacity of red blood cells and therefore predisposes to polycythaemia.9 Nitrogen oxides and other oxidants participate in generation of airway inflammation induced by cigarette smoking.10 The inflammation results in increased mucus production, decreased ciliary movement, and increased mucosal permeability to allergens and therefore increased IgE antibodies & eosinophil count.11 The inflammatory markers C-reactive protein (CRP), interleukin-4 (IL4) & tumor necrosis factor-á “TNFá” play a central role in regulation of inflammatory responses. The CRP is an acute phase glycoprotein produced by the liver. Although its structure is distinct from the immunoglobulins, it shares with them many biological activities. For example, it activates complement,12 acts as an opsonin13 and participates in generation of cytokines that enhance inflammation.14 Its level rises significantly in inflammation, tissue damage and in the presence of malignant tumors. For this reason, quantitative measurement of CRP is increasingly used as a marker of inflammation and tissue necrosis. Passive smokers who are exposed regularly to environmental tobacco smoke have significantly higher CRP levels in plasma15-17 indicating an ongoing inflammatory process. However, many studies reported insignificant rise in plasma CRP among passive smokers.18,19 It is uncertain whether these variable results are due to genetic factors, environmental factors or related to the short half-life of CRP. The IL4 is a potent multifunctional cytokine. It is produced by T lymphocytes, mast cells and basophils to stimulate growth and differentiation of B lymphocytes that secrete the IgE. Cigarette smoking has been associated with increased serum levels of IL4 and increased risk of developing allergic-like symptoms.20 Many studies reported higher IL4 production by peripheral blood mononuclear cells of smokers, compared to that of non-smokers; However, insignificant findings were also reported. Flouris and his colleagues have recently investigated acute effects of environmental tobacco smoke exposure on plasma cytokines. They reported that IL4 and many other cytokines are highly elevated in response to one hour exposure and remain elevated for at least three hours, but effects of regular long term exposure were not studied.21 The TNFá is a potent cytokine that mediates inflammatory and immune reactions.22 It is produced mainly by macrophages to cause inflammation, fever, release of stress hormones, release of acute phase proteins, stimulation of chemotaxis and diapedesis for neutrophils and activation of macrophages.23,24 Many studies confirmed that TNFá production and concentrations in body fluids were greater in smokers than in non-smokers.25-27 However, several studies reported insignificant results.28,29 Recent studies have shown that TNFá plays an important role in the induction of the cigarette related COPD and in the maintenance of airway inflammation.30,31 Variation in the results may be explained in part by genetic factor polymorphism.32 That is why certain people are more susceptible to the negative effects of tobacco smoke than others. The aim of this study was to detect changes in plasma level of the inflammatory markers (CRP, IL4 & TNFá) in healthy male school pupils, in response to passive cigarette smoking. Methods Study area and population This is an analytic observational case control study conducted in three governmental primary schools for boys in Khartoum in the year 2009. The schools were selected randomly from 92 primary schools, the total number of public schools for boys in Khartoum. All pupils in the three schools were approached. Inclusion and exclusion criteria were used to select the test and control groups. The selected pupils were 9 to 14 years old. Parents of the pupils were generally of the average socio-economic class. They lived in houses near the schools of their pupils. Most of the fathers were manual workers or employees and the majority of the mothers were housewives. Inclusion and exclusion criteria Inclusion criteria for the test group were: schoolpupil, aged 9 - 14 years, healthy with normal BMI, has no symptoms or signs of acute or chronic medical illness during the last four weeks, no signs of respiratory disease or chest deformity, not on medical treatment, not active smoker, living with at least one smoker at home, exposed regularly to cigarette smoke at home of not less than two cigarettes per day for most days since birth, and not regularly exposed to environmental tobacco smoke or any other type of smoke outside the house. Inclusion criteria for the control group were: school-pupil, aged 9 - 14 years, healthy with normal BMI, has no symptoms or signs of acute or chronic medical illness during the last four weeks, no signs of respiratory disease or chest deformity, not on medical treatment, not active smoker and not exposed to environmental tobacco smoke or any other type of smoke inside or outside the house. Exclusion criteria for both groups were: age less than 9 or more than 14 years, abnormal BMI, presence of symptoms of acute or chronic medical illness during the last four weeks, presence of abnormal chest signs or skeletal deformity on clinical examination, being on medical treatment, active smoker, exposed to cigarette smoke, or another type of smoke inside or outside the house (for the nonsmokers), or exposed to smoke of less than two cigarettes per day inside the house or to other type of smoke inside or outside the house (for the group of passive smokers). Both groups were matched according to age, sex, height, weight, and area of residence. Methods of data collection Questionnaire Each school pupil was visited at home and interviewed in the presence of his parents to answer questions about his age, health status and smoking habits. Specific questions used for assessment of second-hand smoke exposure included the following questions: Do you smoke cigarettes? Have you ever smoked cigarettes in the past? Is there anyone in the house who smokes cigarettes? If yes, who? Are you exposed to his cigarette smoke? What is the frequency (number of cigarettes/day)? How many days per week? For how many years? Are you exposed to cigarette smoke outside the house? What is the frequency (number of cigarettes/day)? Are you exposed to any other type of smoke inside or outside the house?). Parents were asked to confirm exposure of their child to cigarette smoke at home and to approve the frequency and duration estimated by their child. The questionnaire paper also requested a signed permission to take a blood sample for measurement of pupil’s plasma cytokines. Evaluation of the degree of exposure The information obtained from each pupil and his family about frequency of exposure to cigarette smoke at home was used for classification of the pupils into three subgroups: group of no exposure (includes all the non-smokers), group of mildmoderate exposure (exposed to smoke of two five cigarettes/day) and group of heavy exposure (exposed to smoke of more than five cigarettes/ day). Clinical examination Each pupil was examined clinically to exclude presence of abnormal clinical signs. Height and weight of each pupil were then measured using standardized scales. The Body mass index (BMI) was calculated for each pupil as weight (in kilograms)/ height2 (in meters). The BMI results were compared to normal values of BMI, adjusted for age and sex.33 Preparation and storage of plasma samples Chemically clean and sterile disposable needles, syringes and swabs were used for all samples. About 5 ml of blood was withdrawn from each pupil from the antecubital vein. The blood was collected in a tube containing EDTA as an anticoagulant. Then the tube was sealed, labelled with the pupil’s number, incubated in ice and sent immediately to the laboratory for plasma separation. Plasma was prepared with centrifugation within two hours of venipuncture. The samples were frozen and stored at -20 îC for biochemical analysis. Biochemical analysis The inflammatory markers IL4, TNFá were measured using commercially available quantitative sandwich enzyme-linked immuno-sorbent assay (ELISA) kits according to instructions of the manufacturers. The analyses were performed with 96-well microtiter plate ELISA kits for IL4 & TNFá (from BD Biosciences Pharmingen/USA). CRP was measured with NycoCard Reader II quantitative test (from Axis-Shield/Norway). Test sensitivity was 2 pg/ml for IL4, 2 pg/ml for TNF-á, and 5 mg/L for CRP. Microtiter strips pre-coated with monoclonal antibodies generated against the proteins were used for quantification. Ethical consideration The research conforms to the ethical principles of medical research developed by the World Medical Association Declaration of Helsinki.34 Ethical approval was given by the Research Committee (Faculty of Medicine/ University of Khartoum). Approval was obtained from the Unit of School Health/ Ministry of Education. Permission letters were submitted to the headmasters of the selected schools. Written consents was obtained from the parents before entry into the study. Statistical analysis Data obtained with questionnaire and biochemical analysis were analyzed using the Statistical Package for the Social Sciences version 16 (SPSS Inc. Chicago, IL, USA). The independent student’s t-test was used for comparison between the passive smokers and the non-smokers regarding their physical characteristics (age, weight, height and BMI) and the mean values of CRP, IL4 and TNFá. Statistical significance was accepted when p-value was less than 0.05. Results Physical characteristics of pupils in the study group The mean values of age, weight, height and BMI for the group of passive smokers and the group of non-smokers are presented in table 1. Independent student’s t test was used for comparison of the means of the two groups. Effect of passive smoking on plasma level of inflammatory markers The mean plasma IL4 and TNFá were significantly higher in the group of passive smokers than the group of non-smokers. The mean plasma CRP was also higher in the passive smokers than the nonsmokers; however, the difference was statistically insignificant as shown in table 2. When the degree of exposure to cigarette smoke exposure. The difference between the three groups was considered, the mean plasma IL4, TNFá, and was statistically significant for IL4 and TNFá (p < CRP were lowest with no exposure, higher with mild-0.05). However, it was insignificant for CRP as moderate degree of exposure, and highest with heavy shown in table 3. Discussion Effect of passive smoking on plasma TNF-á It is well known that cigarette smoke can impair pulmonary immune function and initiate release of inflammatory mediators, hence influencing the development of lung diseases. Recent studies have shown that TNFá plays an important role in the induction of the cigarette-related COPD and in the maintenance of airway inflammation.35 Experimental studies in rats exposed to tobacco smoke confirmed the rise in TNFá in both serum and broncho-alveolar lavage fluid.27,36 In this study, a significant rise in plasma level of TNFá was detected in passive smokers, compared to the control group. This finding indicates that inflammation within the airways of passive smokers was already established and there would be a risk of progression to COPD with continuous exposure to tobacco smoke. The contribution of passive smoking to the pathogenesis of COPD and its related mortality was not studied in Sudan. However, worldwide, passive smoking is considered an important risk factor for 10-15% of COPD deaths that are not attributed to active smoking.37,38 In addition, a large proportion of the active smokers who suffer from COPD have been passive smokers during their childhood. Effect on plasma IL4 A number of studies proposed that tobacco smoke modifies CD4/CD8 ratio of T cells, increases T helper cells type 2, and increases IL4/IFNã ratio. This is either by increasing IL4 or decreasing IFNã, resulting in activation of B cells to produce IgE antibodies.11,20 El-nawawy and colleagues in 1996 conducted a research in Egypt on the effects of passive smoking on frequency of respiratory illnesses, serum IgE and IL4.39 They found higher frequency of respiratory illnesses per year, significantly higher total leucocyte count, higher percentage of eosinophils, and higher serum IgE and IL4 concentrations in pupils of smoking parents compared to the control group. Oryszczynin et al. reported a similar rise in IgE antibodies in adults.40 In this study, the rise in plasma level of IL4 in passive smokers was statistically significant. On the other hand, a significant rise in plasma IL4 was detected in the pupils with a high degree of exposure to tobacco smoke compared to the other pupils, again indicating a dose related effect. Effect on plasma CRP The acute phase protein CRP is a well studied marker of systemic inflammation41 and recently has been regarded as a predictor of cardiovascular disease.42,43 Although many studies reported significant difference in the level of CRP among passive smokers compared to non-smokers,15-17 the difference is insignificant in this study. This might be related to the short half-live of CRP or to the lower sensitivity of the quantitative test used for its measurement. However, similar insignificant results were reported in many other studies. In this study, effects of regular passive smoking at home on plasma inflammatory markers were tested among healthy pupils of the average socio-economic class, selected from three governmental primary schools for boys. Effects on girls should be investigated to determine whether there is gender difference in cytokine production or not. On the other hand, the effects of passive smoking on affluent pupils of private schools need to be documented because difference in the socioeconomic status of pupils in the two types of school may influence the mean values of the results. Previous studies confirmed that high socio-economic factors operating from early life, including the overall household income, affect the risk of developing COPD independently of smoking in both males and females.44 On the other hand, low socio-economic status has recently been related to higher levels of inflammatory markers.45,46 To avoid variation in the socioeconomic status between passive smokers and non-smokers, pupils of the two groups were selected from the same type of school and matched according to their area of residence. They were also matched according to their age, weight, height and BMI. Those with abnormal BMI were excluded because both obesity and malnutrition cause alterations in the rate of cytokine production.47,48 It is worth noting that interviewing pupils in the presence of their parents for assessment of secondhand smoke exposure has the disadvantage because they may not give answers that may make them get criticized by their parents. Nevertheless, it has the advantage that parents can confirm their estimation of frequency and duration of exposure. Conclusion These findings confirm that passive smoking causes a significant rise in plasma TNFá and IL4, with a dose dependent effect among school-pupils in Khartoum. Educational programs are highly recommended to increase awareness of parents about the adverse health effects of passive smoking on their children. References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12007t1.jpg] [hs12007t2.jpg] [hs12007t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}