 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 12, No. 1, March, 2012, pp. 77-80 A case of quackery and obsession for diastema resulting in avoidable endodontic therapy *Arigbede AO1, Adesuwa AA2
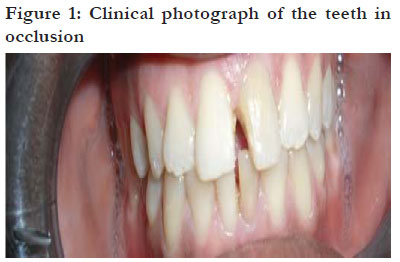
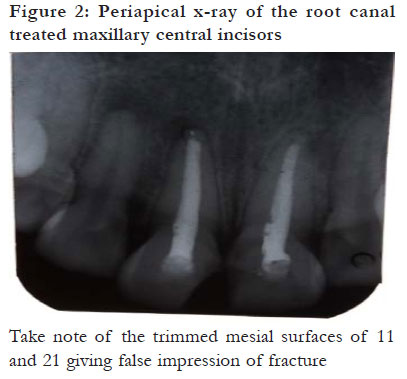
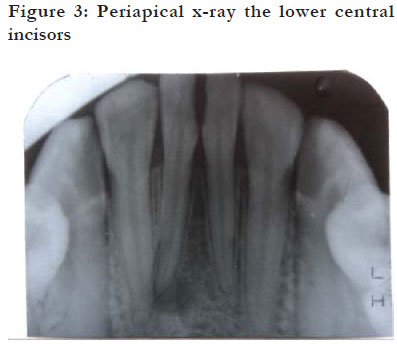
Code Number: hs12014 Abstract Background: Perception of midline diastema differs among individuals and cultures. To some, it is a feature of beauty, while to others it is aesthetically appalling. From a scientific point of view, midline diastema is a deviation from normal adult dentition. It is not uncommon among some African natives to find individuals demanding for artificially created midline diastema from dental practitioners. Key words: diastema, dental quack, root canal therapy Introduction Diastema is a distinctive gap or space between two teeth.1,2 It is most commonly applied to an open space between the upper central incisors, that is, maxillary midline diastema.3,4 A large maxillary diastema may result from disproportionate arch development with disharmony in the size of individual teeth.5 True midline diastema is defined as the one without periodontal/periapical involvement and with the presence of all the anterior teeth in the arch.3 The Black population is said to have a higher incidence of maxillary midline diastema compared to the White population.6 In some dentally aware societies, the presence of diastema in the anterior region can be so displeasing that many patients are motivated to improve such appearance by orthodontic treatment or restorative veneers.7,8 However, the perception of diastema varies in relation to culture, age group, and racial background. In Nigeria, maxillary diastema is generally regarded as a symbol of beauty, hence individuals with midline diastema often enjoy a lot of compliments in the society. In a previous study2 conducted among Nigerians, about 30% of the participants would not mind having artificial diastema. Generally, adolescents have been known to express more intense concerns about their dental-facial appearance compared to adults. Because they undergo a period of biologic growth that involves dramatic physical, sexual, emotional, and cognitive changes, their responses to their appearances are frequently distorted.9 Moreover, they are often exposed to peer pressure and societal vogue which could, sometimes, make them do despicable things in pursuit of beauty. 9 The current case presents a bizarre and unusual aetiology of pulpal necrosis involving maxillary and mandibular central incisors (11, 21, 31 and 41). This was as a result of poorly executed teeth modification (11,21,31 & 41) by a dental quack in a bid to create upper and lower midline diastemata. The justification for this report is derived from its rarity and the usefulness of the experience as further evidence in support of the need for a rigorous dental health education and functional disciplinary body against unprofessional dental practices. Case report A 23-year old married lady with secondary school education presented in our restorative clinic and complained of toothache in relation to 11, 21, 31 and 41. The symptom started three years earlier as a sharp painful sensation of short duration initiated by contact with cold water. The complaint started shortly after maxillary and mandibular midline diastemata were created for her by a dental quack. She claimed that the quack utilized a sharp filing instrument to trim the mesial surfaces of the four central incisors without any form of anaesthesia. Later, the painful sensation became spontaneous and persistent. Two weeks before presentation, there was acute exacerbations in relation to 11 and 21 which led to a sharp, spontaneous, and persistent pain associated with palatal swelling, discharging sinus, and sleep disturbance. She embarked upon selfmedication which only gave her temporary reliefs until the condition became recalcitrant. Systemic review was non-contributory. Examination revealed a symmetrical upper lip swelling associated with tenderness and fullness of the sub-labial sulcus. There was associated discharging sinus in relation to 21. There was a tender and fluctuant palatal swelling measuring about 2cm by 2cm in relation to 11 and 21. Other essential findings include: tenderness of 11 and 21; slight discolouration of the upper left and both lower central incisors; and eccentric relation of the maxillary midline diastema relative to the mandibular midline diastema (figure 1). The patient was fully dentate and her oral hygiene was generally fair. There was no carious or mobile tooth. Vitality test revealed pulpal necrosis with respect to 31 and 41. Periapical x-ray revealed widening of periodontal ligament space in relation to the four central incisors and apical radiolucency in relation to 21 and 41(figures 2 and 3). The root canals were patent and there was no significant alveolar bone loss. Palatal abscess with a discharging sinus secondary to pulpal necrosis of 11 and 21 and Ellis class IV trauma, in relation to mandibular central incisors were diagnosed. Root canal treatment and porcelain fused to metal crown were planned and discussed with the patient and treatment commenced immediately after prophylactic scaling and polishing. The patient was placed on a five-day course of broad spectrum antibiotics and simple analgesics. Root canal treatment of the upper centrals had been completed; but that of the lower centrals and fabrication of porcelain fused to metal crown was deferred on financial grounds. Discussion A previous report2 in the south-western part of Nigeria revealed that about 30% of the respondents would not mind having artificially created diastema. This underscores the value placed on midline diastema in the Nigerian society. The case being presented was that of a Nigerian young adult who expressed so much passion for midline diastema that she submitted herself to unprofessional tooth modification without local anaesthesia. The fact that an individual with secondary education could subject herself to such an harrowing experience of having extensive tooth filing without demanding for local anaesthesia or at least pondering over the possibility of cross-infection and /the or other complications of the procedure, brings to fore the deplorable state of dental health education in Nigeria. It further exemplifies the lack of correlation between general literacy and dental health literacy previously alluded to by Akadiri et al.10 A study conducted in the mid-western part of Nigeria suggests that most dentists did not support the idea of artificially created diastema.11 It is probable that this patient was denied such service by some professional dentists but because of her obsessive passion for diastema, a purported symbol of beauty, she sought the service of a quack. Another possible reason could be the sparse distribution of dental experts in the riverine area of Niger delta region where the patient lived at the time, thereby giving room for quackery. An interesting observation in this case was the demand for both upper and lower midline diastema by the patient. Co-existence of upper and lower midline diastema is an uncommon phenomenon in nature. An incidence of 3.2%2 was reported in a previous study conducted in Nigeria. The general perception has been in favour of maxillary midline diastema which recorded a prevalence of 21.0% in the same study. It is not unlikely that greater premium was placed on combined upper and lower midline diastemata within the patient’s local environment. A study on perception of diastema among major ethnic groups in Nigeria is suggested. Since all the teeth had irreversible pulpal damage and sufficient tooth tissue, RCT and porcelain fused to metal crown is the treatment of choice. Root canal treatment of the upper centrals had been completed, but that of the lower centrals and porcelain fused to metal crown for each respective tooth was deferred on financial grounds. Traditional treatment of oral diseases is said to be extremely costly in several industrialized countries, and it is described as not feasible in most low-income and middle-income countries.12. It is regrettable that a huge and avoidable expenditure in time, skill, and money is incurred on teeth that could otherwise have served a life span. Conclusion This is a case of obsession for midline diastema, poor dental health education, and unprofessional dental practice. The current case underscores the influence a societal belief could hold on the oral health seeking behaviour of an individual. In addition, evidence in support of the need for vigorous dental health education and a functional disciplinary body against unprofessional dental practice in Nigeria is presented. References
Copyright 2012 - African Health Sciences The following images related to this document are available:Photo images[hs12014f1.jpg] [hs12014f3.jpg] [hs12014f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}