 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
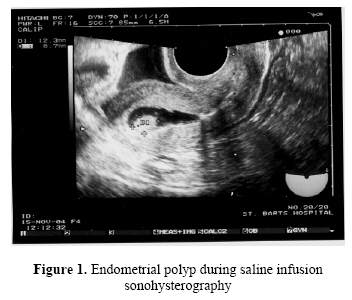
Middle East Fertility Society Journal, Vol. 12, No. 1, 2007, pp. 66-68 CASE REPORT Successful pregnancy and delivery following IVF treatment in a patient with endometrial polyp diagnosed by saline infusion sonohysterography at oocyte retrieval Ahmed S. Kassab, M.D. Ariel Zosmer, M.D. Clair Gillott, M.D. Amanda Tozer, M.D. Talha Al-Shawaf, M.D. Centre for Reproductive Medicine, Barts and The London NHS Trust, Kenton and Lucas wing, St Bartholomew’s Hospital, London EC1A 7BE., UK Correspondence: DR Ahmed Kassab, 21 Monmouth farm close, Pawlett, Somerset, TA6 4SP, U.K, E- mail: kassab1963@yahoo.com, Telephone: 00447810562693, Fax: 00441872255083 Received on August 17, 2006; revised and accepted on September 26, 2006 Code Number: mf07012 ABSTRACT Background: There is lack of consensus regarding the management of
patients diagnosed with endometrial polyp in assisted reproductive technology
(ART) cycles. Saline infusion Sonohysterography (SIS) may provide more precise
identification of endometrial pathology without need for hysteroscopy, cycle
cancellation or cryopreservation of all embryos. Key words: sonohysterography /endometrial polyp/ implantation INTRODUCTION In the transvaginal sonography performed in reproductive medicine, images compatible with endometrial polyps often appear, although their ability to interfere with fertility potential is unknown. There is lack of consensus regarding the management of patients diagnosed with endometrial polyp in ART cycles. Cycle cancellation or cryopreservation of all embryos, and embryo transfer after polypectomy is the current management choice (1), but this can be cost prohibitive. Saline infusion Sonohysterography consists of imaging of the uterine cavity, using real-time ultrasonography during injection of sterile saline into the uterine cavity. This provides information about the shape of the uterine cavity and endometrium (2). It provides more precise identification of endometrial pathology without need for more costly inconvenient procedures as hysteroscopy. Hysteroscopy then be perfect to treat the pathology. We report the first case of pregnancy after diagnosis of endometrial polyp using SIS at oocyte retrieval. Case Report A 38 years old woman was referred to our centre because of primary infertility of 7 years duration. Menstrual cycles were normal and regular with no intermenstrual or post coital bleeding. She had a laparoscopy 15 years ago that showed mild endometriosis which was treated by diathermy. A repeat laparoscopy 8 years ago showed normal pelvic organs, and no endometriosis. BMI was 21. Her partner was fit and well and his semen analysis parameter were within normal range (WHO criteria 1999). She underwent 3 unsuccessful cycles of ovulation induction with clomiphene citrate in 2002. She had Hysterosalpingo-contrast sonography (HyCoSy) that demonstrated an endometrial polyp 11.6 x 4.3 mm and bilateral tubal patency. This is followed by hysteroscopy and removal of the polyp. Histopathology showed benign endometrial polyp. Subsequently, she had 5 cycles of intrauterine insemination but she did not conceive. If anything of note is that whenever she is scanned on day 8 or 9 there was possible endometrial polyp raised with transvaginal scan. Scanning her on day 5 of the cycle endometrium was thin was no evidence of polyp, and that was put down therefore to just endometrial thickening with stimulation. Her first IVF cycle was in 2003. At that time here basal hormonal levels on day 3 of the cycle showed serum FSH 7.1 IU/L, LH 11 IU/L, E2 100 pmol/l. Controlled ovarian hyperstimulation(COH) protocol was with the long down regulation protocol using nafaralin as GnRH agonist and hMG 225 IU daily. Nineteen oocytes were retrieved, of which fourteen fertilized, two embryos transferred on day 2, and six embryos cryopreserved. That cycle was not successful. Six months later she had frozen embryo transfer in natural cycle, all the six embryos were thawed and two embryos were transferred but she did not conceive. In November 2004 she started another IVF cycle using similar COH protocol. On day 9 of FSH stimulation an endometrial polyp was noticed of size 14x 6.8 mm on routine transvaginal ultrasound. Option discussed with patient either to proceed to cryopreserve all the embryos and investigate or to do SIS during oocyte retrieval to confirm the findings and to be followed by hysteroscopy and polypectomy with cryopreserving the embryos or to continue and have day 3 embryo transfer. The patient requested to proceed with the treatment cycle and was reluctant to have cryopreservation of embryos and another hysteroscopy. On day fourteen of stimulation , eighteen oocytes retrieved and SIS was performed immediately afterwards while the patient still under sedation using Embryon HyCoSy catheter 5 fg (Rocket-UK) .This demonstrated 12.3 x 8.7 mm polyp (Figure 1) occupying the posterior fundal portion of the endometrium. To cover any possibility of infection cefuroxime 250 mg t.d.s. and metronidazole 400mg t.d.s. for 7 days were prescribed. The options were discussed again with the patient and she opted to fresh transfer. The following day ten oocytes fertilized and on day 3, eight embryos were developed .Two embryos were transferred both at eight cell stage, grade one and two and no embryo was cryopreserved. Pregnancy test two weeks from embryo transfer was positive. Transvaginal ultrasound showed twin pregnancy with crown rump length 8.2 mm, and 5.2 mm, and both fetal hearts were identified at seven weeks gestation with no evidence of a polyp. However rescan two weeks later confirmed no fetal heart in the second twin, but the first one continues and the patient had normal vaginal delivery of a girl at 40 weeks gestation. DISCUSSION There are only few reports in the literature concerning the effect of endometrial polyp on fertility and in none of them is any conclusion reached. Hereter et. al. (3) in his series of 33 patients with EP diagnosed by ultrasound scan compared with 280 without EP found no difference between the groups with respect to implantation and abortion in IVF cycles. Leiomyomas and polyps are growing tumors and both produce significant plasma glycodelin levels. Uterine glycodelin flushing is also elevated in patients with both polyps and leiomyomas. Elevated glycodelin levels in the follicular and peri-ovulatory period may impair fertilization and implantation by inhibiting sperm-oocyte binding (4). Endometrial polyps usually diagnosed using transvaginal sonography without the need for invasive testing but in view that on day 8 or 9 of the stimulation cycle there was possible endometrial polyp raised with transvaginal scan contradicting earlier scan on day 5 of the cycle, the endometrium was thin with no evidence of polyp. To accurately examine the endometrial cavity to confirm the presence of polyp, SIS was performed. The presence of a polyp was confirmed. The patient got lengthy discussion declining hysteroscopy and polypectomy. It is possible that irrigation of the uterine cavity with saline at the time SIS may have beneficial effect on implantation. Takahashi et al. (5) suggested higher pregnancy rate after hysteroscopy with saline irrigation of uterine cavity on day 7 prior to blastocyst transfer in patients who had failed to conceive after blastocyst transfer (5). IVF treatment and embryo transfer were preceded by repeated endometrial biopsies on days 8, 12, 21 and 26 in spontaneous cycles in a study by Barash et al. (6). A possible mechanism by which endometrial sampling might increase endometrial receptivity could involve events that accompany wound healing. This process is characterized by massive secretion of different cytokines and growth factors, which are also involved in implantation (7). On the basis of this case report, the use of SIS is possible during oocyte retrieval to diagnose missed intrauterine lesions without affecting the implantation potential. Larger cohort of cases of a randomized study will be required to confirm our finding. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}