 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
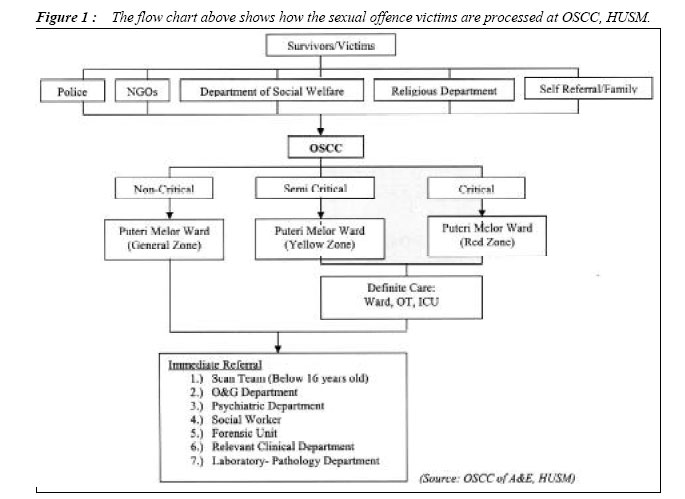
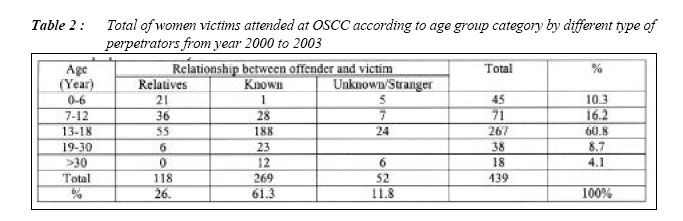
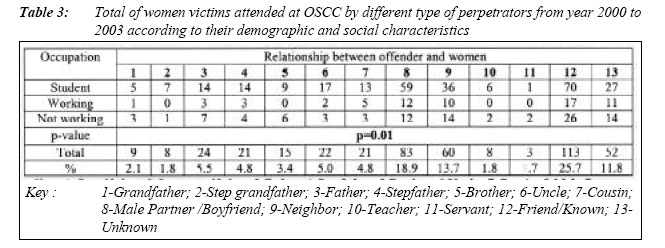
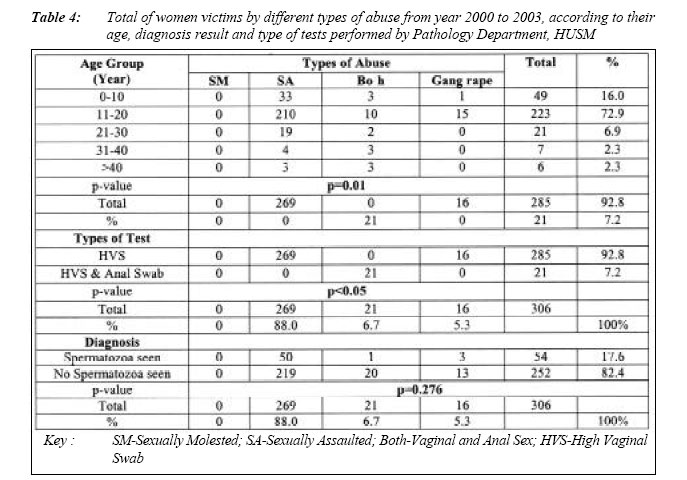
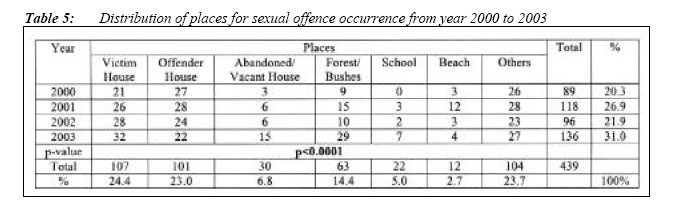
ORIGINAL ARTICLE PATTERN OF SEXUAL OFFENCES ATTENDED AT ACCIDENT AND EMERGENCY DEPARTMENT OF HUSM FROM YEAR 2000 TO 2003: A RETROSPECTIVE STUDY Mohammed Nasimul Islam, Khoo Lay See, Lai Chin Ting, Jesmine Khan School of Health Sciences, Universiti Sains Malaysia 16150 Kubang Kerian, Kelantan, Malaysia Code Number: mj06006 This paper investigates the pattern of sexual offence cases attended at the One Stop Crisis Center (OSCC) of the Accident and Emergency Department, Hospital Universiti Sains Malaysia (HUSM), Kelantan. A total of 439 reported sexual offence cases were examined over a period of 4 years from 2000 to 2003. Sexual offence constituted by male partner or boyfriend in 18.9%, by relatives in 27.3% and by “others” in 53.8% of cases. Only 0.7% of victims did not attempt to lodge a police report. There is a significant relationship between occupation and the risk of experiencing sexual violence. Students were mostly targeted by the perpetrator throughout the study period. Among the offences, rape cases were the highest in number, among those who attended at the OSCC, HUSM with a total of 72.7%; followed by 27.3% of incest; 26.4% of child sexual abuse; 4.8% of sodomy and lastly 1.6% of gerontophilia cases. Only 70% of the specimens obtained from sexual offences victims were sent for laboratory analysis. The result remained negative in 82.4% specimens and thus the laboratory analysis result is merely functioning as a supportive evidence for sexual offence cases attended at OSCC. The studies showed that most of the sexual assault perpetrators were known to the victims. The place of crime was also known to the perpetrators. Health sectors of various levels should be working in conjunction to promote a societal changes to improve more of the women’s right and thus to reduce the violence crime. Key words : Violence against women, Sexual offence, One Stop Crisis Centre. Introduction Sexual offense is considered as violence against women, which is a frequent and significant public health issue in countries of both the developed and developing world. It also implies serious consequences for the women physical and mental health. In HUSM, these victims are specifically handled by the One Stop Crisis Center (OSCC). The purpose of this center is to enable a multidisciplinary management of their problems - all in one place instead of having to send them to different units. The sexual offence cases those who attended at OSCC, HUSM are brought in mostly by the police from various police stations, Non-Government Associations (NGOs), Department of Social Welfare, Religious Department, victim or its family members. Materials and Methods A total of 439 sexual offences cases were received by OSCC, HUSM and the specimens of 306 victims those were sent to the Pathology Department HUSM were reviewed. The raw data collected from OSCC and the Pathology Department were arranged, sorted and tabulated according to age, sex, race, types of abuse, relationship between patient and sexual offender, whether a police report was lodged, education level of the patient and the districts where the patient was from, place of crime occurrence and destiny of patients after discharged from HUSM, type of tests performed, results and from which department the patient’s specimen was obtained. The destiny of sexual offence victims was categorized into discharged to mother, family or to welfare department for further care. The organized data was later entered into SPSS software for further analysis of Independent T-Test, Mann-Whitney U Test (Wilcoxon Rank Sum W Test), Chi-Square Test or Fisher Exact Test and ANOVA. Figure 1 : The flow chart above shows how the sexual offence victims are processed at OSCC, HUSM. ResultsOf the whole sample data of 439 sexual offence cases, all victims of sexual offences were found to be female (100%) and were Muslims (100%). Prevalence of Sexual OffenceBelow are the statistics of prevalence of victims based on age and types of abuse: Table 2 : Total of women victims attended at OSCC according to age group category by different type of perpetrators from year 2000 to 2003 Table 3: Total of women victims attended at OSCC by different type of perpetrators from year 2000 to 2003 according to their demographic and social characteristics Factors associated with sexual offence Laboratory results from Department Pathology Out of a total of 439 cases received, only 306 cases (70%) were sent to Department Pathology for further laboratory analysis. Pattern of sexual offencesThe sexual offence cases receivedby OSCC, HUSM were quite constant from year 2000 to 2003; 20.3% cases in year 2000; 26.9% cases in year 2001; 21.9% cases in year 2002; and 31.0% cases in year 2003. Month of December had the highest amount of cases (49/439) and the least cases (29/439) in the month of February and August. Discussion RapeRape is a complex, psychosocial problem which inflicts pain, terror and humiliation as well as physical and psychological harm on the victim (1, 10). The study revealed a high prevalence of rape cases, which were 72.7% of the total sexual offence cases. This number could be higher because many victims do not report their rapes or even characterize their assaults as being rapes. These cases are only the tip of an “ice berg” issue, where data gathered on rape are based only upon reported rape cases, but for various reasons, many rapes are not reported. These are due to the victim that: (a) may not want the family or other people to know, (b) may be embarrassed, (c) may not understand the legal definition of rape, (d) may not want to report someone they know as being rapist, (e) may lack proof that a rape occurred or (f) may be afraid of subsequent victimization by the police as well as court system. However, more than 95% of the sexual offence cases were reported to the police, either by the victim herself or through the hospital when victim were attended at OSCC, HUSM for treatment (5,13). From this study, there was a significant relationship between rapist and the victim. It was found that 27.5% of the victims were raped by a friend or known person; 18.9% by male partner or boyfriend; 13.7% by neighbor; and 11.8% by an unknown. Among the women who attended at OSCC, HUSM, 77.9% had experience sexual assault in the last 4 years. This was compared with women treated in various communities of different hospitals; the prevalence of sexual violence by male partner was 14.4% (17). Justice system statistics and data from rape crisis centers in Chile, Peru, Malaysia, Mexico, Panama, Papua New Guinea and the United States, indicate that the majority of perpetrators (6078%) were people known to the victim (8). Comparisons with other studies involving patients’ sample were difficult, with too many different variables (country, health system, women’s characteristics, and indicator of violence). Nevertheless, the prevalence found in this study was similar to that found in two recent UK studies (2, 3). The prevalence of sexual violence perpetrated by a male partner in a current relationship was of 5.9%. There was also an association between women’s occupation and the risk of experiencing a sexual offence in the last four years. Students were found most likely to report a sexual offence by any perpetrator, which was 63.3%. Romito and Gerin (2002) also found out that students and women in a precarious situation (with an irregular job or looking for a job) were significantly more likely to report physical or sexual violence by male partner or any perpetrator (p<0.0001) (14). Throughout the study, it was found that sexual offence cases were highly perpetrated by a known person or friend to the victim, followed by the male partner or boyfriend to victim. These findings are found to be similar to the study done by Romito were Gerin (2002) (14). On the other hand, there was a significant association found between age of victims and relationships of victims with offender. This shows that younger women from age 0-6 and 7-12 years old tend to be sexually abused by relatives, as where women from age group of 13-18 years old were more likely to be sexually abused by a known person. Laboratory results from the Department Pathology was usually used only to confirm the presence of spermatozoa and as supportive evidence. High vaginal swabs would be taken from suspected rape victims, such as in cases of sexual assault and gang rape. No laboratory test was performed on sexually molested victims. Anal swab will be taken from victims that experience anal sex as well. Chi square test shows that there was an association between types of abuse and type of tests performed by pathologist. In contrast, there was no association found between types of abuse and the diagnosis result. Out of 284 specimens sent to Department, Pathology reported as, only 17.6% were found to be positive, which was “spermatozoa seen”. About 70% of the total cases attended at OSCC, HUSM, were sent for further laboratory analysis. However, all rape victims would be physically examined by the medical doctors. Table 4: Total of women victims by different types of abuse from year 2000 to 2003, according to their age, diagnosis result and type of tests performed by Pathology Department, HUSM IncestThis study showed that incest cases in Kelantan state were not an infrequent sexual behavior, in which the sexual partners were close blood relations. Though incestual practice is legally prohibited, but the number of cases had shown to increase from year 2000 to 2003. Majority of victims of incest fall into category of age 0-6, 7-12 and 13-18 years. Only 6 cases were reported by victims from age 19-24 and 25-30 years. From the total of 439 sexual offence cases, 120 cases (27.3%) were found to be incest. It is indicated that 2.1% were victims of incest by their grandfather; 1.8% by their step grandfather; 5.5% by their father; 4.8% by their stepfather; 3.4% by their brother; 5.0% by their uncle; and 4.8% by their cousin. According to the National Center for Victims of Crime and Crime Victims Research and Treatment Center (1992), from the 61% of rape victims, 11% were raped by their fathers or stepfathers, and 16% were raped by a relative (11). This findings were similar to the results found in this study where 10.3% of victims attended at OSCC, HUSM were raped by fathers and stepfathers where as another 17.1% were raped by relatives. Table 5: Distribution of places for sexual offence occurrence from year 2000 to 2003 Child Sexual AbuseA child is defined as “every human being below the age of 13 years unless under the law applicable to the child majority is attained earlier” (United Nations, 1996) (2). Meanwhile, according to WHO (1999), child sexual abuse is the involvement of a child in sexual activity that he or she does not fully comprehend; is unable to give informed consent to, or for which the child is not developmentally prepared and cannot give consent (13). The media and popular cultural stereotypes tell us that the most likely victim of sexual abuse is female between the ages of 18 and 30. However, it was startling to know that the finding that sexual offences were committed against victim under the age of 12 years old. From this study, child is in the age group of 0-6 and 7-13 years old, which consist of 45 cases and 71 cases respectively. This contributed to 116 cases of the child sexual abuse, which is 26.4% of the total case. Perpetrators of child sexual abuse were also found among family members, which was categorized under incest. 46.7% were victims of incest from age group of 0-6 years and 50.7% were from age group of 7-12 years old. On the contrary, 53.3% were victims of sexual offences from age group of 0-6 years and 49.3% were from age group of 7-12 years old. Children aged 0-6 years were found to be sexually abused by their servants at home. 29.3% of child sexual abuse were perpetrated by neighbors and were found to contribute the most compared to other perpetrators of child sexual abuse. Among family members or relatives, the uncle was the most who contribute to child sexual abuse (12.1%); followed by 9.5% by the father; 7.0% by the cousin; 6.0% by the grandfather; 5.2% by step the grandfather and step the father; and 4.3% by the brother. SodomyOf the whole sample, only 4.8% of the women victims experienced both sodomy and vaginal rape. Hence, High Vaginal Swab and Anal Swab were taken from these victims for further laboratory analysis. However, only 1 case (4.8%) had shown a positive result. 95.2% of the rest of the specimens were negatively diagnosed with “no spermatozoa seen”. Sodomized victims were 14.3% from age 06 years; 47.6% from 7-12 years; 33.3% from age 13-18 years; 9.5% from 19-24 years; 4.8% from both age group of 25-30 and 37-42 years; 14.8% from age 31-36 years; and 19.0% from age more or equal to 43 years old. GerontophiliaGerontophilia is the use of an elderly person as sexual object (10). This type of sexual offence were rarely seen and reported. 0.9% of women from age 37-42 years and 1.6% of women from equal or more than 43 years old reported to have experienced sexual abuse for a period of 4 years. These women aged equal or more than 43 years old, experienced only 2 types of abuse, which were sexual assault (27.3%) and both sodomy and vaginal rape (36.4%). In contrast, the elderly women aged 37-42 years old experienced 3 types of abuse (excluding gang raped), which were sexually molestation (9.1%), sexual assault (18.2%) and both sodomy and vaginal rape (9.1%). ConclusionRape is thought to be the most heinous of crimes. The by-products of rape can include the destruction of the victim’s feeling of worth and the victim’s internalization of feelings of responsibility for her own victimization (4). Many people, including victims, police and social scientists generally agree that rape is a crime of violence rather than a crime of sex. Feminists regard rape as the epitome of sexism and a symbol of the oppression of women by men (16). This study has proven that the myth about rape that “rapists are usually strangers” is not true. About 88.2% of the perpetrators were known to the victims and only 11.2% were unknown. The known perpetrators vary from family members, relatives, to male partners or boyfriends, neighbors, teachers, servants and friends. In addition, people always think that crime scene, especially where rape or sexual assault occurred, is a dark and secluded place. However, this study shows that nearly all rapes occurred at the victim’s home or the offender’s home as well as neighborhood. Sexually abusing one’s own child as in incest cases is considered as a social and familial offence. In this study, the result shows that most incest cases were by the victim’s own father, followed by the uncle and the stepfather. It was also shown that the rumors that incest cases are high in Kelantan are true. 27.3% of the victims attended at OSCC, HUSM were noted to be incest victims. The health sector, at various levels, could and should be more active in working together with women’s movement, to highlight the extent of the problem and to advocate for societal changes. Besides, it is essential that all legal, medical and police procedures must not cause further trauma to the sexual offence victims who must actually be given all possible supports and care. Grassroots organizations, researchers, workers in the health sectors and the policymakers, need to acknowledge and not to deny the existence of this problem and start to assess what role they can play in promoting change. AcknowledgementThis study was supported by Universiti Sains Malaysia Incentive Grant (2003) and presented at the 10th NCMS USM Health Campus. The authors wish to thanks Dr. Haji Ramli Saad, Former Director HUSM, Dr. Zaidun Kamari, current adjunct Director HUSM, Dr. Wan Aasim Wan Adnan, Former Head of the Department Emergency Medicine and Associate Professor Dr. Hasnan Jaafar, Head of the Department of Pathology for their kind permission to allow us to handle the documents in the OSCC and Department of Pathology of HUSM respectively, as well as DSP Sulong Affandi Bin Mohd Hashim of Kelantan police contingent for his cooperation by giving us statistics from the police record. References
© Copyright 2006 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj06006t4.jpg] [mj06006t2.jpg] [mj06006f1.jpg] [mj06006t5.jpg] [mj06006t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}