 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
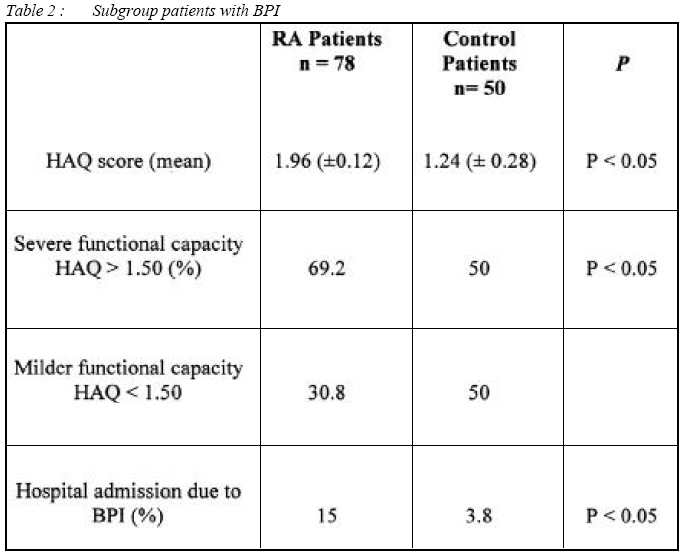
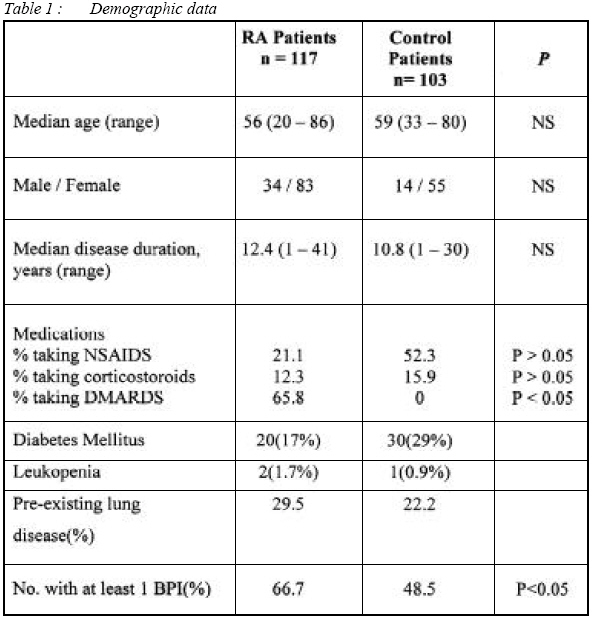
Malaysian Journal of Medical Sciences, Vol. 15, No. 2, April 2008, pp. 24-28 ORIGINAL ARTICLE The Prevalence of Bronchopulmonary Infection Among Patients with Rheumatoid Arthritis Versus Non Rheumatoid Arthritis Patients Anwar Arshad & Rozita Rashid Penang Medical College, No4, Jalan Sepoy Lines, 10450 Penang, Malaysia. Submitted-28-10-2007, Accepted-24-02-08 Code Number: mj08014 A high frequency of bronchopulmonary infections complicating rheumatoid arthritis has been described in reports of case series. This study was undertaken to confirm and compare these finding in patients with RA and control. 117 patients with RA and 103 patients with OA/soft tissue rheumatism as controls. Study subjects were studied using their medical records available from hospitals‘ casenotes and GP data base. Details of all documented bronchopulmonary infections for the preceding year including lower and upper respiratory tract infections were recorded. Details of hospital admissions due to bronchopulmonary infection, antibiotic usage and functional capacity were also recorded. Mean age for RA was 56 and 59 for control. There were 34 males and 83 females in RA group, however, 14 males and 55 females in control group. There were at least 1 episodes of BPI in 66.7% (p<0.05) patients with RA and 48.5% in control. 69.2% (p<0.05) of subgroup patients with RA were noted to have poorer functional capacity compared to 50% in control. More RA patients with BPI (15%) (p<0.05) were admitted to hospital compared to control (3.8%). Significance findings were noted in terms of prevalence of BPI in RA patients compared to controls as well as patients with RA have severe course of BPI warranting hospitalization. RA patients with poorer functional capacity also noted to have high incidence of BPI. Key words : Bronchopulmonary infection, Lung infection, Rheumatoid arthrtitis Introduction Compared with the general population, the life expectancy of patients with rheumatoid arthritis (RA) was found to be shorter, and the surplus mortality was associated with, among other things, the occurrence of infections 1 . Infection complicating the course of RA has been persistent problem and has long been recognised as an important cause of death. Over the past few decades, studies from various countries have established that patients with rheumatoid arthritis (RA) have higher mortality due to common infectious disease, in particular, bronchopulmonary and genitourinary infections, when compared with the general population 2-5 . There was also special relationship between bronchopulmonary infection (BPI) and RA, not just a major cause of death in RA patients, but, incidence of BPI were thought to be more common in RA patients. Aronoff (2) described in 1967 that bronchitis was commoner in patient with RA and suggested that this could be due to increased susceptibility to infection. Walker (3) also reported in the same year that BPI was commoner in RA patients. This study will be focusing on the frequency and prevalence of BPI only as the main theme of this research. We hypothesized that, patients with RA will have higher incidence of BPI than control. thus the main objectives of this study were to confirm and characterize the occurrence and prevalence of BPI in patients with RA and controls. The study also attempts to examine whether degree of disability predict the frequency and severity BPI in patients with RA. Methodology A study was conducted on 117 subjects with RA and 103 subjects of matched control at Alor Star Hospital rheumatology outpatient clinic. All cases suited the criteria for classic or definite RA if they had 4 out of 7 American College of Rheumatology criteria (revised ACR criteria 1987) and all rheumatological diagnoses (including those in the controlled group) were made by a qualified rheumatologist. Both early and late disease of RA were included in his study. Most of the diagnoses in control group were osteoarthritis (OA), soft tissue rheumatism and fibromyalgia ( i.e. primary or secondary OA of the knees, hips, spine, generalised OA, bursitis, tenosynovitis and low back pain ). All subjects with OA of the hip and knee were all suited the 1990 and 1986 ACR criteria for diagnosis respectively. Fibromyalgia syndrome diagnosis was also based on the 1990 ACR diagnostic criteria. Information on demographic data such as gender, age and duration of rheumatological diagnoses of all patients were recorded. All necessary facts about patients regarding BPI, medications, functional capacity (mHAQ) and chest problems were available through reviewing their medical record (hospital and GPs). A total of 230 patients were recruited in this stud and finally only 117 RA patients and 103 controls remained for analysis and study. The patients‘ casenotes were reviewed and noted whether they had any BPI during the preceding year. Data on all episodes of infection requiring medical care were collected. Information on minor upper respiratory tract infections was also collected and patients’ history of visiting their general practitioner (GP) were recorded. The primary outcome measure was infections with objective confirmation, defined as those with positive results of either microbiologic, cultures or radiologic imaging, or both. Secondary outcome measure included infections that required hospitalization and all physician-documented infections. The operational definition for BPI were as follows: isolation of a pathogenic microorganism from 1 or more sputum cultures, with fever (>38.0°C), pneumonia, presence of new infiltrates, consolidation or effusion seen by chest radiography an suggestive clinical features. Lower respiratory tract infections (LRTI) could be included on the basis of a physician’s diagnosis and relevant clinical finding alone, but microbiologic culture result were recorded if available. For each episode of BPI, we collected information on accompanying fever, leukocytosis, and findings of relevant investigations, including microbiologic culture and radiologic findings. We also recorded whether the infection required hospitalization, and length of hospital stay. Information on potential confounding factors for infection such as diabetes mellitus, leucopenia, neutropenia and corticosteroid use, along with dates of onset, was ascertained through medical record review. Concurrent chronic respiratory problems in all subjects were recorded such as bronchial asthma, chronic obstructive airways disease (COPD), fibrosing alveolitis, bronchiectasis (BR) and lung malignancy. The status of concurrent respiratory diseases were assessed with the help of patient‘s own GP, hospitals‘ casenotes and verification with the attending chest physician. In order to study the functional activity of all subjects, modified health assessment questionnaires (mHAQ) were used. All subjects were further subdivided into 2 groups according to their mHAQ scores to categorized their severity in terms of functional capacity. Those who score 1.50 and less were categorized as having mild disease and those with scores more than 1.51 were regarded as having severe disease. Results are analyzed using SPSS version 9.0. The statistical tool employed was student‘s T-test with a confidence interval of 95%. P value <0.05 is considered significant. Results Demographic Profile There were 117 RA patients and 103 controls group. Of 103 controls, 63 subjects with OA, 26 with fibromyalgia and 14 with soft-tissue rheumatism. There were 34(29.1%) male and 83(70.9%) female patients in the RA group. In control group only 23(22.7%) male patient identified and 80(77.3%) female. Gender distribution was homogenous. The mean age of RA patients was 56 years old ± SEM 1.3 (ranging from 20 – 86 years). The mean age of 69 patients in control group, the mean age was 59 years old ± SEM 3.4 (ranging 33-80 years). Table 1 illustrates the distribution of age group amongst the 2 comparative groups. Majority of the patients studied were above 40 years old. No significant difference in age distribution. In RA group the mean disease duration is 12.40 years ± SEM 0.94 (ranging 1 – 41). In the control group the mean disease duration is 10.8 years ± SEM 3.51 (ranging 1-30). In RA patients 24 subjects (21.1%) were treated with analgesia/NSAID, 14 (12.3%) patients were on steroid only and a significant number of patients; 75 (65.8%) were on DMARD however there was only 1 patient not on any treatment at all (refer table 1). In control group 54 patients (52.3%) were on analgesia/NSAID, 16 patients on steroid (15.9%) and 33 (18.2%) patients were not on treatment at all. The patients whom were on steroid in this group probably not for their rheumatological condition but for other conditions such as COPD. Prevalence of bronchopulmonary infection. In this study 78 (66.7%) patients with RA were noted to have had at least 1 episodes of BPI, 50 (48.5%) in control group and the difference reached statistical significance (p>0.05). Details of hospital admission due to bronchopulmonary infection. There were 18 (15%) patients in RA group admitted to hospital due to severe BPI and 4 (3.8%) in control group and this also reached statistical significance (p>0.05). Pre-existing lungs problems In RA group, 29.5% of the patients reported pre-existing lung disease whereas in control group, 22.2 % reported those condition as well. These findings were not statistically significant (p>0.05). In RA patients, 2.6% had bronchiectasis (BR), 17.9 % had chronic obstructive pulmonary disease (COPD), 5.1 % had asthma and 1.3 % had recurrent chest infection. However in non-inflammatory diseases, 11.1 % had asthma, 5.6% had recurrent chest infection and lung fibrosis respectively. Functional disability (modified HAQ score) In sub group RA patients with BPI, mean HAQ score is 1.96 ± SEM 0.12 (p<0.05), however in control group, mean HAQ score is 1.24± SEM 0.28. In terms of severity, 69.2% of RA patients with BPI were found to be in the more severe group (HAQ>1.50) and 30.8% in the milder group (HAQ<1.50). These observation were statistically significant (p<0.05) as only 23.2 % of the control with RTI were in the more severe group and 76.8% in the milder group. Majority of subjects in controls group with mHAQ of more than 1.50 were found to have OA and fibromyalgia syndrome. Discussion This study clearly demonstrate that the prevalence of BPI in patient with RA are higher than in control group and BPI requiring hospitalization were also higher in patients with RA than controls. The above results, confirms with the tentative hypothesis that RA patients are prone to be more susceptible to BPI. A recent large population-based study in Rochester, Minnesota also found that patients with RA are at twice the risk of developing an objectively confirmed infection compared with age and sex matched individuals in the same community who do not have RA 6 , however, 2 previous studies 7,8 in the 1987 and 1988 respectively from the same center showed no difference in infection rates between cases and control, however, these 2 previous studies used different methodologies that might explained the negative results. In principle, various mechanisms could account for this phenomenon. It might be that an increased susceptibility to infections already exists before RA develops, and that this susceptibility is part of the general causal pathway which leads to the development of the disease. A higher frequency of infection in RA patients might also be due to medication, decreased mobility, skin defects, or impaired neutrophil function9. Recent evidence suggest that RA patients have immunologic abnormalities involving the majority of circulating T cells, from an early stage in the disease course10 . Thus, the ability of the immune system to respond to novel antigenic stimuli may be compromised. It was also observed that, the prevalence of RA patients with BPI was higher in those with severe functional capacity compared to those in control group. These finding were statistically significant. It was notable that a higher frequency of infection in patients with RA might be due to the impairment of host defense, related treatment and decreased mobility 11.Decreased mobility also was reported to be one of the factors responsible for infection. As far as the context of this study is concerned, an assumption could be table out higher HAQ score will be consistent with poor mobility. Thus the finding would fit the previous description which explained the susceptibility of those with poor mobility to infections. There are many implications from these study, firstly, sepsis should strongly suspected in RA patients with fever and cough as this might more common than an extra-articular manisfetation of RA, secondly, those with more severe functional disability are the one that will succumb badly during course of infection. Conclusion In patients with RA, the prevalence of bronchopulmonary infection noted to be higher than those in control and severe functional disability is associated with an increased incidence of bronchopulmonary infection. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08014t2.jpg] [mj08014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}