 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 15, No. 2, April 2008, pp. 43-46 CASE REPORT Molecular Genetic Analysis Of A Suprasellar Immature Teratoma : Mutation Of Exon 4 P53 Gene Nujaimin Udin, Ku Asmarina Ku Ahmad, Farizan Ahmad, Effat Omar*, Mohd Ezanee Aziz**, Raj Kumar, Jafri Malin Abdullah Department of Neurosciences, Department of Pathology*, Department of Radiology**,
School of Medical Sciences, Universiti Sains Malaysia, Health Campus
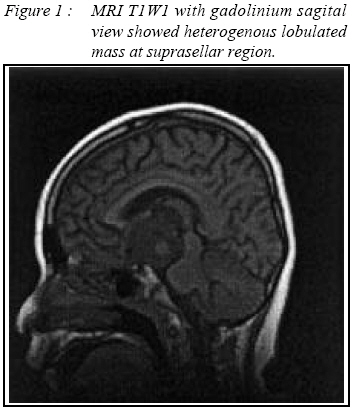
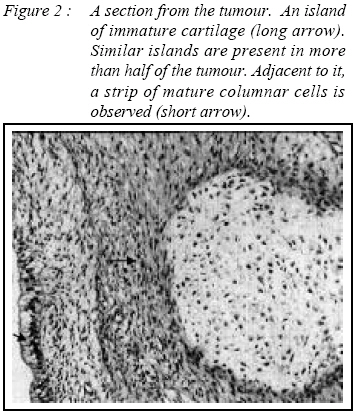
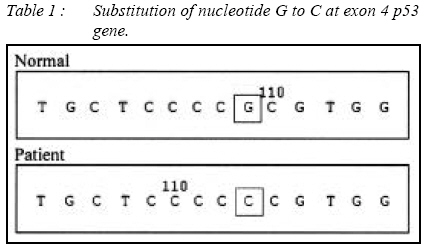
16150 Kubang Kerian, Kelantan, Malaysia Submitted-20-02-2005, Accepted-30-12-07 Code Number: mj08018 We described an intracranial immature teratoma in a 13 year old Malay boy who presented with history of chronic headache and blurring of vision. Physical findings revealed bilateral papilloedema but no other localizing sign. A Magnetic Resonance Imaging of the brain revealed a suprasellar well defined lobulated midline heterogenous mass which was intraoperatively described as mainly solid tumour with multiple small cystic component filled with yellowish jelly like material. Histopathological finding confirmed the case as immature teratoma. Molecular genetic analysis of p53 and p27 genes revealed substitution of nucleotide G to C at location nucleotide 12139, exon 4 of gene p53. No alteration was detected at exon 5-6 and 8 of p53 gene and exon 1 and 2 of p27 gene. This is the first case report of an intracranial immature teratoma with genetic mutation occuring in a Malay boy. Key words : Teratoma, Immature, Suprasellar, Genetic Analysis Introduction Central nervous system germ cell tumours which include teratomas are commonly encountered amongst children and adolescents and they constitute about 0.5% of all primary intracranial neoplasms (1). The most common site intracranially is midline about the third ventricle, the commonest being the pineal region followed by suprasellar region. Mature and immature variants require distinction. The p53 gene is believed to play a critical role in the carcinogenesis of astrocytic brain tumors. In contrast, only few studies have examined the significant of this p53 mutation in non-astrocytic brain tumors. We reported a case of grade 4 immature teratoma located in the suprasellar region with a genetic mutation of p53 suppressor gene but no mutation detected in the p27 gene. Case Report A 13 year old Malay boy presented with one month history of chronic headache and blurring of vision without diplopia or visual field lost. The symptoms acutely worsened 2 days prior to admission, with deterioration of conciousness on the day of hospitalization. He regained full conciousness after admission but the headache and blurring of vision persisted. Past medical history was insignificant and there was no known brain tumour within the family. On clinical assessment, he was normotensive and examination of higher mental function was normal. Eye examintaion revealed reduced visual acuity and papilloedema bilaterally. There was no abnormal mass palpable in the abdomen or scrotum. Pituitary function test, screening of alpha fetoprotein, human chorionic gonadotropin and placental alkaline phosphatase were normal. MRI of the brain with focus on the sellar region disclosed a well defined lobulated midline heterogenous mass at suprasellar region mesuring 3.7 x 4.4 x 4.3cm with minimal perilesional edema, a small area suggestive of blood product and some cystic year-old areas. Post godolinium, the mass showed heterogenous marked enhancement, extended into the sella region and the pituitary gland was flattened (Figure 1). The patient underwent a subfrontal craniotomy and tumour excision. Intraoperatively the mass was described as mainly solid tumour with multiple cystic component filled with yellowish jelly like materials but none which could suggest bone, teeth or hair within the tumour. Pathological examination Grossly the tumour was received in multiple fragments. The largest fragment was solid and cystic measuring 55 x 45 x 20 mm. The external surface was smooth with tiny papillary configurations seen in few areas. Microscopically the tumour was composed of tissue of the three germ cell layers. More than half of the tumour consists of islands of immature mesenchymal and epithelial tissue, mostly immature cartillage. Mature elements such as sebaceous cells, squamous and respiratory epithelium as well as loose fibrous connective tissue are seen in between the structures. Neuroectodermal element is not present (Figure 2). Specimens and DNA samples The specimen was obtained from the Brain Tumor Tissue Bank of the Department of Neurosciences, University Science of Malaysia. This study was approved by the Research Development and Human Ethics Committee, School of Medical Sciences, University Science Malaysia, in year 2000. Genomic DNA was extracted from the tumor tissues using DNeasy Tissue Extraction Kit, QIAGEN (USA) according to the protocol suggested by the manufacturer. Blood samples were also extracted using DNeasy Blood Extraction kit, QIAGEN (USA) and used as normal controls. Polymerase Chain Reaction Amplification of p53 and p27 genes Exon 4, 5-6 and 8 of p53 gene and exon 1a, 1b and 2 of p27 gene were amplified using 6 different pairs of primers. The amplification was performed using a Thermal Cycler PTC-200 (MJ Research) in a 50µl volume assays, containing 100ng of genomic DNA, 0.5µM of each oligonucleotide primer, 0.2mM of dNTP mix, 1X PCR buffer containing Tris-HCl (pH 8.8), (NH4)2SO4, 1.5mM of MgCl2 and 0.025 units of Taq DNA polymerase. PCR products were then electrophoresed in 2% agarose gel and the bands were visualized by UV transilluminater and camera system with conjunction to software. As for controls, we performed PCR using extracted DNA from normal blood obtained from healthy volunteers together with the PCR reactions for p53 and p27 genes. To confirm the effectiveness of the procedure, we also sequence the DNA of the control amplified product. DNA sequencing The PCR product was purified using GeneClean II Kit (Bio 101 Inc, USA) before it was sent to First Base Laboratories (Malaysia) for the DNA sequencing analysis. Results Our DNA sequencing results revealed a substitution of nucleotide G to C at the location of 12139 in exon 4 of p 53 gene. However, there was no alteration found in exon 1a, exon 1b and exon 2 of p27 gene and exon 5-6 and exon 8 of p53 gene. Discussion Teratomas are defined as tumours derived from the 3 embryonic germ layers: ectoderm, endoderm, and mesoderm, which are not normally found at the site of detection. Teratomas may be classified into mature or immature based on the presence of immature elements within the tumor. Mature tumors classified as grade 0 has no immature elements. In grade 1 tumors, immature elements are limited to 1 low-power field per slide; in grade 2, fewer than 4 fields are detected per slide; in grade 3, more than 4 fields are detected per slide (2). Macroscopically immature teratoma will have immature element of fat, chondroid nodules, teeth, hair and bony spicules. These immature components have been reported to undergo spontaneous differentiation into mature somatic type tissue after some times. Teratoma with malignant transformation is the one that contains additional malignant component of conventional somatic type. Immunohistochemical study may show positivity of alpha fetoprotein and cytokeratin. Radiologically teratoma commonly appears on computed tomography and magnetic resonance imaging as heterogenous lesion that can be shown to contain intratumoural cysts admixed with calcified foci and regions having low signal attenuation suggestive of fat. Two previous studies in molecular genomic analysis of intracranial germ cell tumours were restricted to investigation of the p53 tumour suppresor gene. The first study by single strand conformation polymorphism analysis and direct nucleotide sequencing reported p53 gene mutation in one of seven germinomas and three of five yolk sac tumours but none of teratoma (3). The second study using a yeast functional assay however failed to reveal any p53 gene mutation on assessment of seven germinomas, five teratomas and two embryonal carcinomas (4). We have studied both p53 and p27 genes and have successfully demonstrated substitution of nucleotide G to C at location nuleotide 12139, exon 4 p53 gene. We however failed to demonstrate any genetic mutation at exon 1a, 1b and 2 of p27 gene. The presence of p53 mutation may indicate the possibility of malignant transformation of immature and mature teratoma. However no large study has yet been done to prove this hypothesis. From our study, we postulate that genetic mutation of p53 suppressor gene is likely to be detected in immature teratoma of higher grade as described in our case. The degree of the teratoma immaturity and genetic mutation with potential malignant transformation may determine patient’s survival. Conclusion Intracranial teratomas are rare. This is the first case report of immature teratoma in a Malay boy with p53 mutation on molecular genetic analysis but there is no mutation seen on molecular genetic analysis of p27 gene. Acknowledgements We thank School of Dental Sciences, USM for the p53 primer and MAKNA for the grant that support our neurosciences brain tumour research work. References
© Copyright 2008 - Malaysian Journal of Medical Science The following images related to this document are available:Photo images[mj08018t1.jpg] [mj08018f1.jpg] [mj08018f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}