 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Medical Journal of the Islamic Republic of Iran , Vol. 19, No. 2, August, 2005, pp. 127-130 PREDICTING THE RISK OF PRETERM LABOR BY SECOND TRIMESTER MEASUREMENT OF MATERNAL α-FETOPROTEIN LEVELS AND A RISK FACTOR SCORING SYSTEM FATEMEH DAVARI TANHA,* M.D., FARIBA SARDARI, M.D.,ZAHRA EFTEKHAR, M.D., MAHBOD KAVEH, M.D., AND NARGESSIZADY MOOD, M.D. From the Department of Obstetrics & Gynecology, Mirza Koochek Khan Hospital, Reproductive HealthResearch Center, Tehran University of Medical Sciences, Tehran, Iran. *Assistant professor, Department of Obstetrics & Gynecology, Mirza Koochek Khan Hospital, Reproductive Health Research Center, Tehran University of Medical Sciences. Address: Mirza Koochek Khan Hospital, Villa St., Karim Khan Blvd., Tehran, Iran.Telephone: #98-21-8900002,Fax:#98-21-8904172, E-mail: fatedavari@yahoo.com Code Number: mr05005 ABSTRACTBackground: Preterm labor (delivery after 20 weeks and before 37 weeks of gestation)
is the leading cause of prenatal mortality in developed countries. Many women
who have preterm labor have abnormally high plasma levels of α-fetoprotein
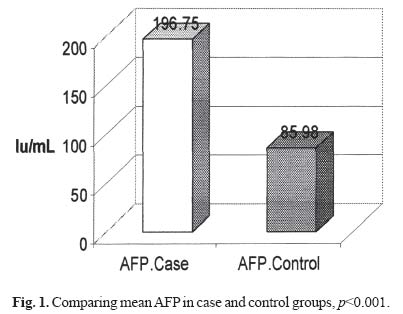
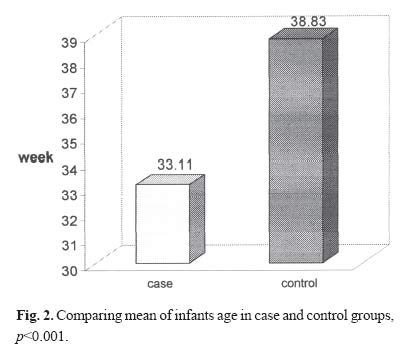
in early pregnancy. Keywords: α-fetoprotein, prematurity, preterm delivery. INTRODUCTION Preterm labor is the leading cause of prenatal mortality in developed countries. Survivors of preterm birth may face permanent intellectual and physical handicaps and have higher incidences of chronic illness, hospital admission, growth failure, and learning difficulties than infants born at term.1 Preterm birth results in enormous financial costs. The immediate prenatal care of a child born at 25 to 27 week’s gestation in the United States is estimated to cost >28000 dollars, compared with 9800 dollars for a child at term. Additional health costs arising from the long-term complications of prematurity were estimated, even in 1988, at 5.5 billion per year2 Although the prevention of preterm birth has long been recognized as an important goal, the incidence of preterm birth has actually remained unchanged for >30 years. Attempts to prevent preterm birth have focused on 2 strategies, which may be complementary4: 1- inhibition of preterm labor (reactive strategy) and 2-prevention of the initiation of preterm labor (proactive strategy). The reactive approach is limited because many women with preterm labor still seek treatment at an advanced stage and because current tocolytic treatments are successful in prolonging gestation for an average of only 24 to 48 hours.5 The proactive approach depends on the recognition of basic mechanisms of preterm labor and intervention to modify these mechanisms at an early stage in affected pregnancies. Such an approach requires the use of a screening test that will discriminate high risk pregnancies.4 Screening has been performed by the identification and scoring of clinical risk factors for preterm birth,6 but risk factor scoring has proved to have a poor detection rate and a poor predictive value.7 Furthermore, because a risk factor score is based largely on a women’s previous obstetric history its accuracy is particularly low among primiparous women, who constitute approximately 50% of those affected by preterm delivery. Previous studies have found the relationship between maternal serum AFP and CRH in the second trimester and preterm labor.10 The α-fetoprotein level rises a few months before labor. There is a similar association of second trimester maternal plasma α-fetoprotein (AFP) concentration with preterm delivery alone or associated with risk factor scoring and this led us to postulate the existence of a “placental clock”controlling the length of human pregnancy. Based on studies increase of AFP plasma level in mother not only shows fetal abnormality, but also can be due to multiple pregnancy, spontaneous abortion, still birth, preterm labor, pre-eclampsia, and low birth weight.6 In this study the relation between second trimester maternal plasma level of AFP and the system of risk factor scoring for the prediction of preterm labor has been assessed. PATIENTS AND METHODSThis is a nested case control study and subjects were recruited from an antenatal clinic in 2002-3. Six-hundred patients were evaluated. One-hundred twenty patients were chosen at delivery. The case group (n= 60) were women with preterm labor, single pregnancy without uterine anomaly or fetal abnormality and a certain gestational age. The control group (n=60) were women with the same criteria but term gestation. Exclusion criteria consisted of uncertain gestational age, multiple pregnancy, uterine anomaly, trophoblastic disease and fetal abnormality. Six-hundred women were chosen with gestational age from the beginning of the second trimester until delivery. One sample was tested for each woman between 17-30 week’s gestation. Then AFP level was measured in the sample of women in case and control groups which were detected after delivery. AFP level and the system of risk factor scoring for preterm labor based on Table II were assessed as indicators of preterm labor. The sensitivity, specificity, predictive values, LR+, LR-and accuracy of the test were calculated by Excel system. Comparisons of AFP values and the system of risk factor scoring between groups were assessed with Fisher exact test and t- test. Data were analyzed by SPSS. RESULTSThe range of age of patients was 20-41 years in the case group, mean 27.56+5.33 years and 19-44 years in the control group, mean 28.4+6.65 years which is not statistically significant (p= 0.436, Table I). Thus none of the patients had less than 18 years. Mean value of maternal plasma level of AFP was 196.75±151.48 IU/mL in the study group and 85.98±55.90 IU/mL in the control group (p<0.001), which is significant statistically. (Table I, Fig. 1). Mean values of neonatal age were 33.11±3.40g in the study group and 3241±405.98g in the control group (p<0/001) which is statistically significant (Table I). (Fig 2)
Neonatal sex had no statistically significant difference in the two groups. After determination of risk factors and scoring (as seen in Table II) the following results were obtained. The minimum and maximum score in both groups was 0 and 20 respectively: a score >10 in 17% of the study group and 8% of the control group. Ten women in the study group and 5 in the control group had a history of one preterm labor (OR= 2/2). 17 women in the case and 11 in the control group had had one spontaneous abortion before (OR=1/76). Three women in the case group had a history of two spontaneous abortions but no one had this history in the control group. Three women in the study group and two women in the control group had a history of abortion and preterm labor (OR=1/ 52). There was no history of three induced abortions or smoking. The history of urinary tract infection and cervix cerclage was the same in the two groups (two and three cases respectively). A concentration of AFP higher than 100 IU/mL or higher than the normal range of the laboratory was considered as positive and less than this value considered as negative. Cases who had preterm labor and high plasma AFP levels were considered true positive, and those with term labor false positive; those with low plasma AFP level and term labor were considered true negative and those with low plasma AFP level and preterm labor false negative. There was 47 true positive, 21 false positive, 39 true negative, and 13 false negatives. Based on our data the sensitivity of this test was 78%, CI 95% and range 66.38%86.88%, specificity was 78% with CI 95%, range 52.4075.80%. Positive predictive value (PPV) was 69.10% with CI 95%, range 57.20-78.20% .Negative predictive value (NPV) was 75% with CI 95%, range 63.20-82.90. LR+ = 2.24, was calculated in range (1.56-3.24) and LR-= 0.333 in range (0.199-0.558), accuracy test was 71%. DISCUSSION The main object of this study was to assess the relationship between maternal serum AFP level in the second trimester and preterm labor. In our study as seen in Table I the same association is shown and women with preterm labor had higher AFP values in the second trimester of pregnancy. Prematurity is a heterogenic disorder with multiple causes. Most cases are idiopathic and may be due to Table II. Method of calculation of risk factor score.
acceleration of the “placental clock”. Measurement of the AFP level may be effective in detection of these groups. In a previous study7,9 in women with high AFP levels in the second trimester the risk of obstetrical complications, mainly preterm labor, low birth weight and prenatal death were higher. It is suggested that by considering AFP as a routine test in prenatal care, and as the role of this test in detection of some fetal abnormalities such as neural tube defect (high AFP) or Down syndrome (low level) has been proven, if AFP is routinely assessed in the second trimester and a high level is detected, target sonography is suggested to rule out any abnormality. If an abnormality is excluded prophylactic management consisting of bed rest, decrease in maternal activity, and corticosteroids for lung maturation between 24-34 weeks of gestation are recommended. Another goal of this study was determination of the relationship between risk factor scoring system and preterm labor. The minimum and maximum score in both groups was 0 and 20 respectively. History of preterm labor and abortion in the study group was more than the control, and when this history is present it is an alarm for repeating preterm labor. In this study vaginal bleeding after 10 weeks of gestation, urinary tract infection and cerclage of the cervix was the same in both groups and has not been considered as a risk factor for preterm labor. In the study of Mc lean et al. in 1999 a score higher than 10 was seen in 28% of cases of preterm labor and 7% of term ones. In our study the difference between the two groups was less (17% versus 8%) and was not statistically significant. CONCLUSION Prevention of preterm birth has been a major goal in modern obstetrics, but progress in this area has been disappointing. A significant obstacle to the success of prevention programs has been difficulty in discriminating a high risk pregnancy.10 Recent insights into the processes of normal and abnormal parturition have found a number of potentially important biochemical mechanisms that have a bearing on the timing of delivery. Our understanding of these processes is still rudimentary, but the results of this study suggest that testing for biochemical markers may provide a way forward in the attempt to first predict and then prevent preterm birth. The combination of measurement of maternal serum AFP in the second trimester associated with a risk factor scoring system provides a more accurate indicator of the risk of preterm delivery and therefore may be of use in targeting prevention strategies. REFERENCES
Copyright 2005 -Medical Journal of the Islamic Republic of Iran The following images related to this document are available:Photo images[mr05005f1.jpg] [mr05005f2.jpg] | |||||||||||||||||||||||||||||||||||||||||
| |||||||||
{kind=link}
{kind=link}