 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 8, No. 1, Jan-Mar, 2009, pp. 50-54 Relationship between orofacial pain and absenteeism among workers in Southern Brazil Anderson Nardi1, Edgard Michel-Crosato2, Maria Gabriela Haye Biazevic3, Edgard Crosato4, Eduardo Pizzatto5, Dagmar de Paula Queluz6 1MS, Universidade do Oeste de Santa Catarina (Unoesc), Joaçaba (SC), Brazil
Received for publication: July, 17, 2008 Code Number: os09010 Abstract
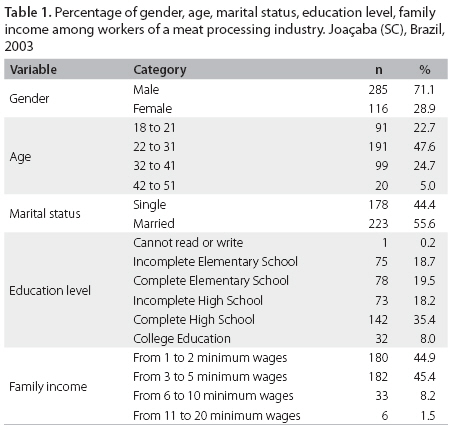
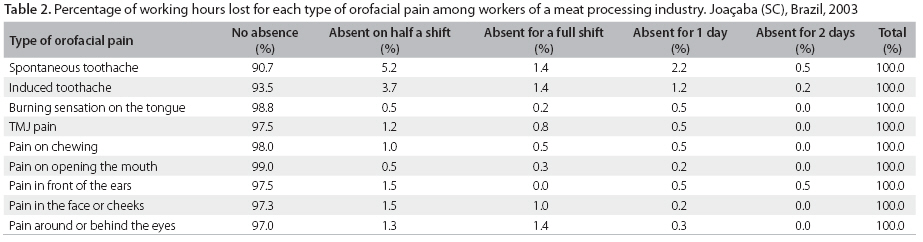
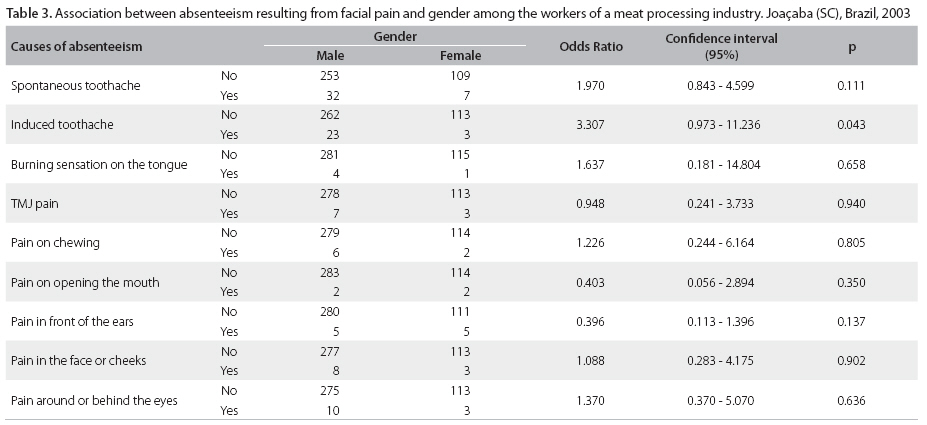
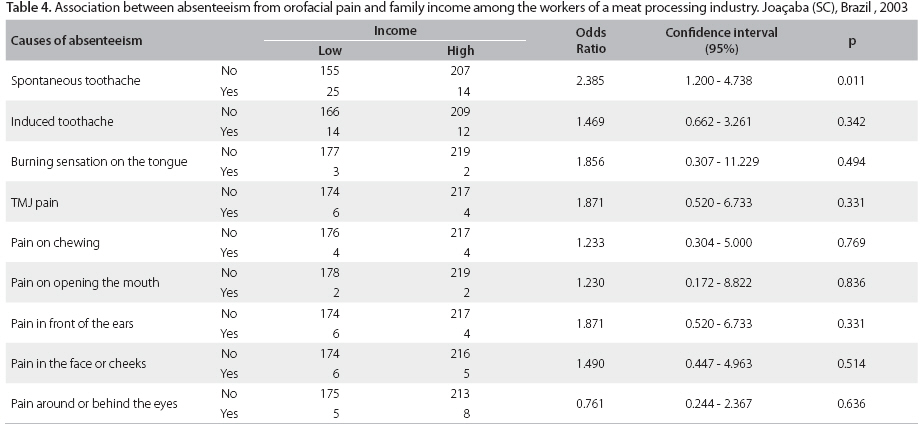
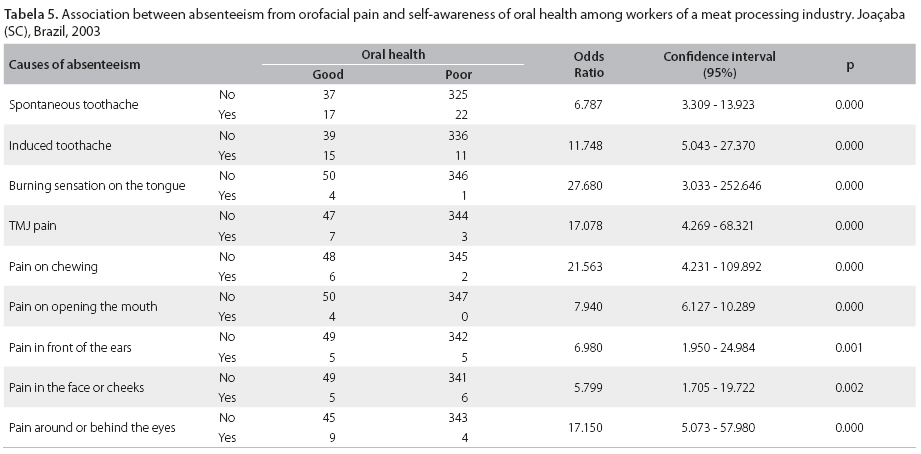
Aim: To verify the relationship between orofacial pain and absenteeism in workers of slaughter and meat processing industries in the Southern region of Brazil. Keywords: absenteeism, facial pain, facial pain/epidemiology, oral health. Introduction Absenteeism is an issue of growing interest as a result of the economic importance of competitiveness, driving companies to seek means to reduce its occurrence and, consequently, to increase the profitability and achieve sustained growth1,2. Various epidemiological studies have demonstrated that the prevalence of absenteeism resulting from dental reasons varies from 10 to 35%, and the average number of working hours lost varies from 1.24 to 6.20 working hours/workers/years3-9. The pain is a private percept that arises in a conscious brain, typically in response to a noxious provoking stimulus, but, sometimes, in the absence of a stimulus. The relation of the percept to the stimulus is variable, and depends on the individual’s prior expectations and beliefs, and on his/her cognitive and emotional state – not just on the nature of the stimulus itself. While acute pain is, by definition, a brief and self-limiting process, chronic pain comes to dominate the life and concerns of the patient, and often also family, friends and other caregivers. In addition to the severe erosion in quality of life of the pain sufferer and those around him/her, chronic pain imposes severe financial burdens on many levels. These include: costs of healthcare services and medication, job absenteeism and disruption in the workplace, loss of income, non-productivity in the economy and in the home, financial burden on family, friends and employers, worker compensation costs and welfare payments. The workers can reduce absenteeism and healthcare utilization from the risks from dental disease by incorporating dental education into workplace wellness. The aim of this study was to verify the relationship between orofacial pain and absenteeism in workers of slaughter and meat processing industries in the Southern region of Brazil. Material and methods The study population was composed of a sample of 401 workers of slaughter and meat processing industries in the Southern region of Brazil. The company workforce was composed of 1,187 employees. Sample size calculation was done using the following criteria: confidence level 95%, sample mistake 4% and unknown prevalence, and estimated prevalence 50%. The selection process of the samples was realized through simple random drawings. An observational and cross-sectional study design was used. Data collected referred to absenteeism resulting from orofacial pain, as well as social and economic characteristics of the study population (gender, age, marital status, area of work, address, educational level and family income). A questionnaire developed by Locker & Grushka6-7 was used as an instrument for the survey, which was validated in Brazil in the Bambuí Health and Ageing Study (BHSA)10. The questions in the survey instrument referred to the situation of absenteeism caused by nine different types of orofacial pain and also the amount of time the employee was kept from work. The questionnaire was prepared to gather information about orofacial pain and absenteeism at present or in the recent past. All questions referred to the period encompassing the six months prior to the survey. This relatively short period of time is normally used to minimize bias due to possible lapse of memory of the surveyed study population11,12. About the family income, low means until two minimum wage, and high means two or more minimum wages. The oral health, it was self related good or poor. The questionnaire was first applied to 15 employees. Thereafter, it was applied by duly trained surveyors to the employees that agreed to be enrolled as volunteers after granting authorization from the company management and after the participants had signed an informed consent form to take part in the study. The research project was approved by the Research Ethics Committee of the Universidade de Passo Fundo (UPF) under the protocol number 194/03. Data were analyzed by the chi-square test using the Stata 8.0 software and presented in tables, according to the frequency distribution. A 5% significance level was adopted for all analyses. Results The social and economic status of the studied population is shown on Table 1. Among the participants in the study, 60 employees declared having lost working hours due to orofacial pain in the six months prior to the survey. Consequently, the prevalence of absenteeism due to orofacial pain in this study was of 15%. The types of orofacial pain that cause more absenteeism were: spontaneous toothache (9.7%); toothache caused by cold or hot liquids or sweet foodstuff (6.5%) and pain around and behind the eyes (3.2%). Table 2 shows the percentage of loss of working hours for each of the nine types of orofacial pain described. The predominance of loss of half and full work shifts was observed for all types of orofacial pain experienced. A half work shift was considered as a period of four hours, in other words, half a day’s work. The types of orofacial pain that caused two and three days or more of absence from work were the spontaneous toothache, toothache caused by hot or cold liquids or sweet foodstuff, pain in front of the ears and pain around and behind the eyes. Considering the prevalence of absenteeism according to the number of types of pain experienced by workers, 26 employees informed having been absent from work due to one type of orofacial pain (6.5%), 18 employees informed having been absent as a result of two types of orofacial pain (4.5%), nine employees informed having missed work as a result of feeling more than three types of orofacial pain and only one worker informed having missed working days as a result of feeling the nine types of orofacial pain (0.2%) in the last six months (Table 2). The association between absenteeism and gender indicated that the prevalence of absenteeism resulting from toothache caused by hot or cold liquids or sweet foodstuff (p = 0.043) was higher for male workers (Table 3). Table 4 shows that the prevalence of absenteeism resulting from spontaneous toothache was higher among workers with the worst level of family income (p = 0.011). An association was also observed between absenteeism resulting from orofacial pain and self awareness of oral health (p < 0.001). Employees who declared having poor oral health conditions presented a higher prevalence of absenteeism resulting from orofacial pain, in the nine types of orofacial pain studied, than those who declared having a good oral health status (Table 5). Discussion The prevalence of absenteeism due to orofacial pain for the workers of the meat processing industry was of 15%, and the average number of lost working hours as a result of dental causes was of 0.88 working hours/employee/year. When comparing the results of this study to those of various epidemiological studies3-9, it was noted that the prevalence of absenteeism for dental reasons in the study population matched the previously found values. However, the average number of working hours lost by the employees of the meat processing industry was below those results previously presented. The orofacial pains that caused the highest levels of absenteeism were: spontaneous toothache (9.7%); toothache caused by cold or hot liquids or sweet foodstuff (6.5%) and pain around and behind the eyes (3.2%). These pains have the characteristic of acute cases with a relatively short duration and that can be rapidly treated, reestablishing the workers’ capabilities to perform their functions and enabling their prompt return to their jobs. Considering the amount of time absent from work as a result of orofacial pain, there was a predominance for the loss of half or a full work shift as shown in Table 2. The average number of leave-of-absence days due to dentist certificates was of 1.5 days/employee/year. These results are consistent with those presented in previous studies11-14. Absenteeism caused by dental reasons in this meat processing industry was smaller than absenteeism resulting from medical causes in both average length and total number of leaves of absence, being these data similar to the survey by Reisine15. Employees who declared having poor oral health status presented a higher prevalence of absenteeism due to orofacial pain than those who declared having a good oral health status. In this sense, self-awareness of the oral health status coincided with the impact observed through the application of the instruments: work-related activities are more severely affected among employees who presented the perception of their poor oral health condition. This study did not demonstrate any associations between prevalence of absenteeism due to orofacial pain and age, marital status, schooling, geographical area (rural or urban), company sector or work shift. There are two types of absenteeism: absenteeism through the absence of work and physically present absenteeism. The first type can be measured and its costs can be calculated through the absence. The second type cannot be measured, since it represents the worker who cannot perform his/her normal working activities due to pain, despite being physically present to the workspace13. Labor is increasingly becoming effective and instrumental in the social-economical advancements in our society14. The attention of the authorities responsible for the implementation of the directives of a country that has its economy based on labor should be oriented towards the health and welfare. Consequently, workers should be the objective of measures and policies to preserve their physical, mental and social well-being. Therefore, maximum productive capacity is achieved when the worker is satisfied in his basic health needs11-16. Studies have shown that oral problems caused difficulties or incapacity to perform normal working activities, study or sleep in a percentage that ranges from 8 to 60%16-18. In the present study, associations between absenteeism from induced toothache and gender (p = 0.05); absenteeism, spontaneous toothache and family income (p = 0.011); and absenteeism, self-awareness of the oral health condition and the nine types of orofacial pain (p = 0.00) were observed. The prevalence of absenteeism as a result of orofacial pain was low. It is important to point out that the methodological aspects of future epidemiological studies about orofacial pain and absenteeism must be standardized, in such a way that the results of the various studies could be compared with greater reliability. Since absenteeism for dental reasons was not pronounced, the company did not present losses in productivity because their work force contemplates a surplus percentage of employees to compensate for absences. References
Copyright © 2009 - Piracicaba Dental School - UNICAMP São Paulo - Brazil The following images related to this document are available:Photo images[os09010t4.jpg] [os09010t2.jpg] [os09010t1.jpg] [os09010t5.jpg] [os09010t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}