 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Seroprevalence of Hepatitis A in 7-10 Year-old Children Seyed Alinaghi Kazemi *1, MD; Manoochehr Mahram1, MD; Ali Koosha 1, MD; Hamid Reza Amirmoghaddami 2 1Department of Pediatrics, Zanjan University of Medical Sciences, IR Iran Received: 7/9/06; Code Number: pe07009 Abstract Objective: Hepatitis A is one of the most common infections during childhood,
especially in
developing countries. Regarding the high prevalence of the disease in Iran,
this study was
performed to detect the rate of the contact of the children of Zanjan/Iran
with the virus of hepatitis
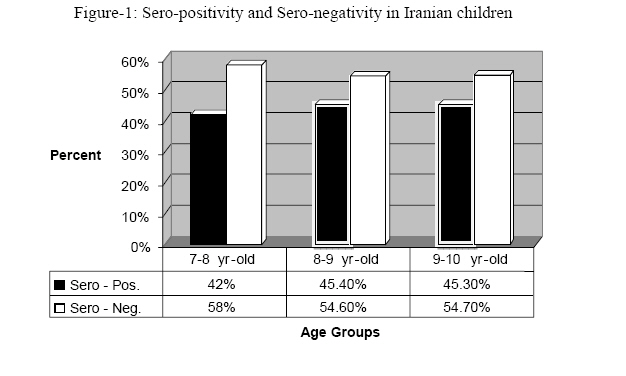
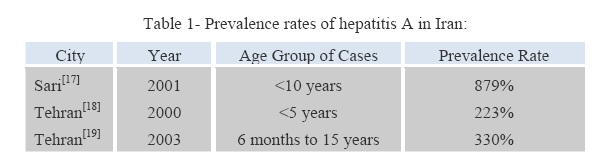
A (HAV). Key Words: Anti-HAV, Children, Hepatitis A, Viral infection Introduction Hepatitis A (HA) does not recognize country, state, and international borders[1], but it is a usually mild and self-limited disease, and rarely causes chronic illness[2]. The disease in children has good prognosis, with no chronicity[3]. HA in children is mostly asymptomatic, and the disease was seldom clinically evident[4]. For example, in children less than 3 years, more than 80% of infections are clinically silent[5] but rarely serious complications, such as pleural effusion, are reported[6]. HA causes approximately half of the cases of viral hepatitis in the United States[7]. Based on a one-year study in USA, of 270,000 patients of hepatitis A, 159,200 were under 10 years old[8]. In another study, the rate of seropositivity of hepatitis A in the population of that country was reported to be 60%[9]. Hepatitis A incidence rates in the United States reached their lowest level in 2002[7]. In developing nations, most individuals acquire antibody by 5 years of age [1]. In a study in India, 80% of 5-10 year-old children were seropositive for the disease[10]. The rate of seropositivity and involvement of the community decreases with increase in socio-economic level and welfare in community[11,12]. Transmitted maternal antibody can protect an infant completely up to 6 months of age[13]. Although vaccination against hepatitis A in infancy is less efficient[14], this performance after 2 years of age has had desirable result[15] Anti-HAV can be found in serum from disappearing of the virus in stool, its level reaches maximum in a few months, and will remain measurable up to several years. IgM-antibody remains high only for two months, rarely may be measurable in the next year, and is used to diagnose recent infections. The role of IgGantibody is to prevent next episode of the infection[16] This study was performed on 7-10 year-old children of Zanjan (as a relatively deprived city in Iran), regarding limited studies of this kind in the country. It seems that with the improvement of socio-economic level of the nation, the rate of involvement with the infection is gradually diminishing, but since the disease is accompanied with more complications in older age groups, and with regard to the neighboring countries of low socio-economic and hygienic levels with high prevalence of the infection, the risk of transmission of the disease and occurrence of epidemics in this country should be seriously kept in mind. Material & Methods This descriptive study was accomplished from February 2003 through February 2004 in Zanjan City (North-West of Iran). The sample consisted of 300, 7-10 year-old school children. Using multi-stage randomized method, the children were selected by systematic sampling from 30 primary schools, 10 children from each school. The sample consisted of equal number of both sexes. The minimum sample size for the study was calculated considering p=80% and α=95%. After two sittings with the schoolmasters and children's parents the aim and potential risk factors of the study were explained to all subjects and their parents before informed consent was obtained. Then, all information needed for the study was registered in questionnaires. Five ml venous blood was collected from each one of the children. The serum from collected blood samples were promptly frozen and kept in micro tubes in -70°C temperature to be examined simultaneously later. To measure total anti-HAV, we used One-Step Competitive ELISA (Dia-Pro, Milan, Italy) method. Quality control of the kits was performed at a specialized laboratory in Zanjan. Specific antibodies present in serum, compete with specific antibodies linked to HRP (Horse Radish Peroxidase) enzyme to attach to antigens. By adding the enzyme substrate, the strength of the produced color will be reversely proportionate to the quantity of specific anti-HAV antibodies in the serum sample. Sensitivity of this method is 10 IU/L (conformable with WHO standard), specificity and accuracy of the kit were more than 99%. For statistical analysis of the quantitative and qualitative parameters, we used T-test and K² analysis, respectively. An institutional review board in Zanjan University of Medical Sciences approved the study procedures. Findings Out of 273 children, including 134 (49%) boys and 139 ( 51%) girls, 322%, 322% and 356% were in age groups of 7-8, 8-9 and 9-10 years, respectively. There was no significant difference in distribution of samples in age or sex groups. 27 children rejected to participate in the study On the whole, 121 (443%) cases had high serum level of total antibody against hepatitis A. 425% of girls and 46% of boys were seropositive. Although this showed a little higher prevalence in boys, was not significant statistically. Comparison of age groups for being seropositive is shown in Fig 1. Discussion This study showed that about 443% of 7-10 yearold children in Zanjan City had previous contact with hepatitis A virus, with no significant difference in distribution of samples in age or sex groups There are three similar studies on the prevalence rate of hepatitis A in Iran, which are shown in Table 1[17-19]. The two studies in Tehran indicate the prevalence rates of 33% for children under 5 years and 223%, for those aged 6 months to 15 years [18, 19]. Different researches show lower prevalence rates in developed communities. For example, 27% of 8-13 year-olds were seropositive in Canada by prior contact with HA virus or immunization[4]. On the other hand, occurrence of the infection is seen in underdeveloped communities up to 100% [20]. Involvement with hepatitis A in childhood is directly proportionate to the hygiene level of the community and observance of the rules of health by the people [16]. A decrease in the prevalence of the disease up to 29% [21] in Turkey during recent years and unchanged 95% statistical reports in Syria [22] confirm this assertion. These reports show a change in age pattern of contamination to the virus. Ehsani et al have recommended revision of prevention protocols of hepatitis A, after contact with this virus in highly contaminated areas in Iran [19]. Although these results were similar to the results of a study in Istanbul with a prevalence of 29% [21], had a significant difference with the similar studies in Syria (95%) [22] and Palestine (937%) [23]. In our study there was no difference between sexes, but in one recent study in Canada female gender was associated with a higher proportion of anti-HAV IgG positivity [4]. There is no program for routine hepatitis A vaccination in Iran; this means that 443% of 7-10 year-old children of Zanjan City have had previous contact with Hepatitis A Virus. More than 55% of teenagers in this city would be at risk for infection in case of contact with HAV. Changes in immunization policy against hepatitis A should be considered especially with regard to many travels of people between Iran and other countries with high prevalence of disease such as Syria. The probability of an epidemic of the disease in the country should always be kept in mind. To prevent the disease, revision of national prevention protocol, i.e. public vaccination and eventually passive immunization (immuneglobulin) is recommended. Conclusion According to this study, 443% of 7-10 year-old children of Zanjan City has had previous contact with Hepatitis A Virus.. This shows a high rate of seronegativity and sensitivity in adult community susceptible to infection with regard to the high incidence of travels between Iran and neighboring countries with high prevalence of disease. Therefore, revision of national prevention protocol is recommended. Acknowledgment The Deputy of Research Affairs of Zanjan University of Medical Sciences funded this research, for which we are highly grateful. We also have to thank Dr Faranak Sharifi, for her unreserved cooperation and collaboration References
The following images related to this document are available:Photo images[pe07009t1.jpg] [pe07009f1.jpg] |
| |||||||||

{kind=link}
{kind=link}