 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 1, March, 2008, pp. 87-91 Letter to Editor Resolving Clubfoot Deformity Misleading and Delaying the Diagnosis of Tethered Cord Syndrome Amit Agrawal, MD, MCh; Neurosurgeon Department of Surgery, Datta
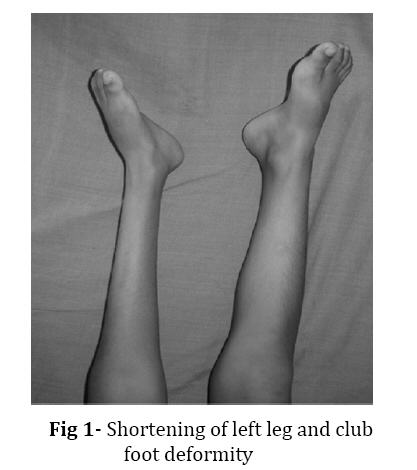
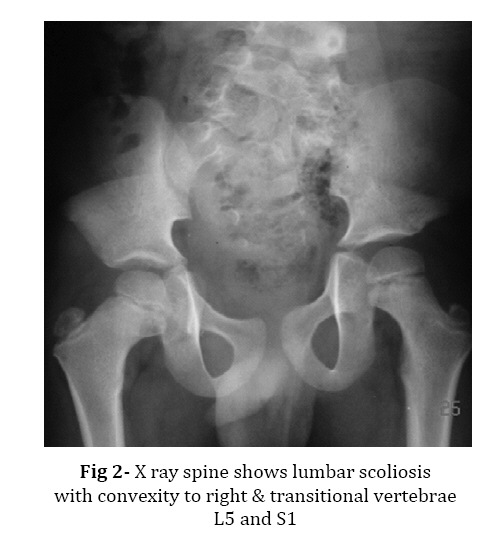
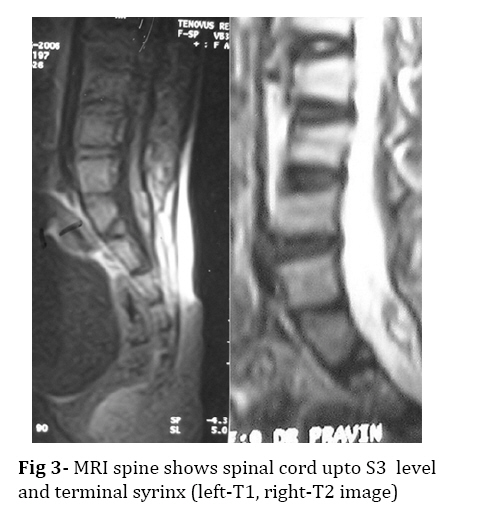
Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha, India Received: 01/09/07; Revised: 15/10/07; Accepted: 17/12/07 Code Number: pe08017 Neural tube defects comprise of a group of congenital malformations and failed closure at the cranial end is known as anencephaly, is a lethal condition, whereas failed closure at the caudal end usually results in a myelomeningocele.[1,2]Tethered cord syndrome (TCS) usually is a stretch induced functional disorder of the spinal cord. The mechanical cause is an inelastic structure anchoring the caudal end of the spinal cord that prevents cephalad movement of the lumbosacral cord.[3] Five years old male child presented with slowly progressive weakness of both lower limbs (left more than right) since birth, pain, paresthesia with shortening of left leg. There was no history of urinary or fecal disturbance. Patient had club foot deformity since birth for that he was evaluated and diagnosed as spastic type of weakness and was on regular physiotherapy at a local hospital. As he grew older, parents noticed shortening of left lower limb. His physical examination showed wasting of muscles in left lower limb in all groups and dissociated sensory loss below L3 with apparent shortening of left lower limb by 2 cm (Fig. 1). Mid thigh circumference of two thighs differed by 5.5 cm. Tone was decreased in left leg with power of 4/5 with absence of ankle and knee reflexes in both legs. On spinal examination, 2 cm defect was palpable over L3, 4, 5 vertebrae with tuft of hair on the overlying skin. Spinal X-ray showed scoliosis of lumbar spine with convexity to right, transitional vertebrae L5 and S1 (Fig. 2). MRI revealed spina bifida S1 and 2 with evidence of small herniation of dura with herniation of nerve roots with tethered spinal cord at S1 and 2 with small spinal lipoma on right side at S1 level & focally dilated syrinx L1 and L2 level (Fig. 3). USG study of abdomen was normal. Patient was subjected to detethering of spinal cord and excision of terminal lipoma. On follow up, patient is doing well with relief in pain and minimal improvement in power. In present case club foot was treated in an isolated manner and other stigmas of tethered cord were not looked for. Child showed apparent improvement in spastic clubfoot deformity secondary to the development of lower motor neuron type of deficits. It is suggested that tethered cord syndrome should be clinically suspected and investigated and detethering should be done early to avoid the sequelae of the disease as in this case.[4] These defects are a complex disorder involving many genetic and environmental factors.[2]Folate metabolism pathway genes have been examined for association with these congenital defects.[1,2] Animal models demonstrate that periconceptional folate supplementation protects against congenital defects in the face, neural tube, and conotruncal region of the heart. Low folate could directly limit its availability to cells or indirectly disrupt methionine metabolism, thereby increasing homocysteine in the maternal serum.[5]Future studies aimed at identifying these risk factors must approach the problem with a wide perspective including several genes and collecting as much environmental data as possible.[2]In a study from North-East area of Iran, which has a high prevalence of neural tube defects the role of zinc deficiency has been investigated and it has been shown that there is an association between neural tube defect and low serum zinc level in the newborns.[1]This finding focuses attention once again to the importance of nutritional factor in the etiology of neural tube defects. Further studies should be carried out to verify or prove the cause - effect relationship of zinc deficiency with NTD.[1]This case illustrates that we should make aware all the medical persons involved in care of these patients and help to investigate all patients with congenital deformities of lower limbs particularly when it is associated with features of spina bifida occulta and also there is need to take preventive measures to avoid neural tube defects. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08017f3.jpg] [pe08017f1.jpg] [pe08017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}