 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
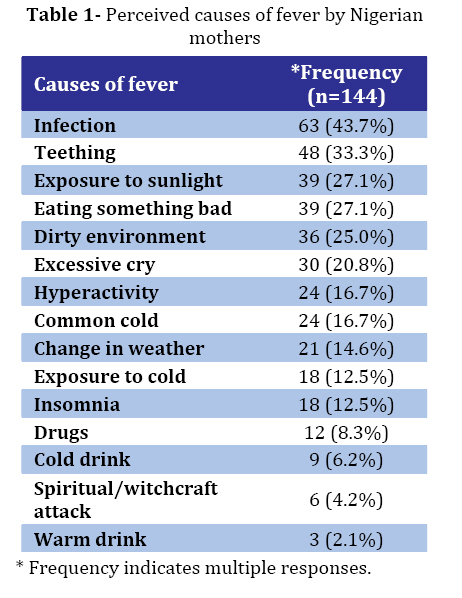
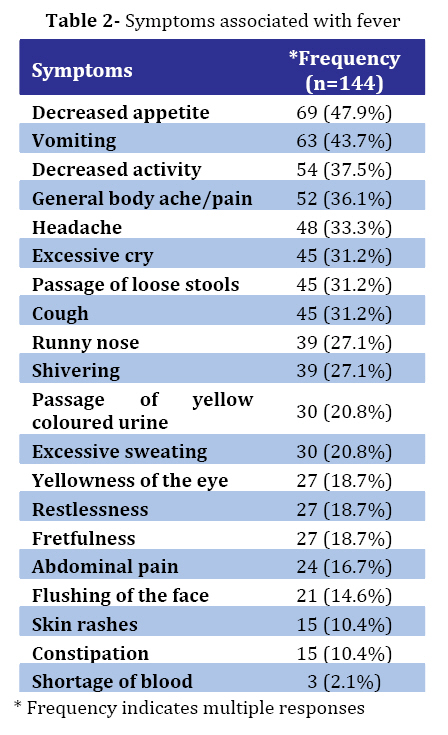
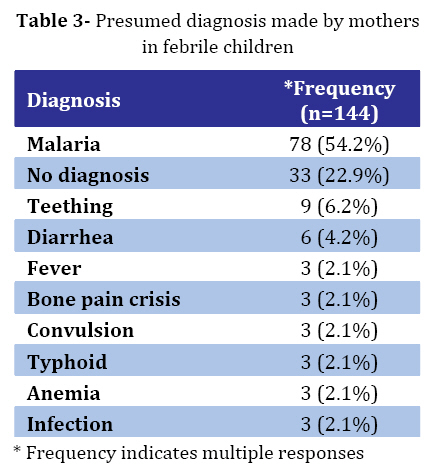
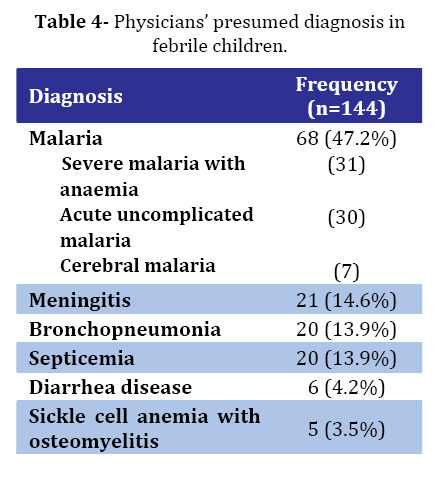
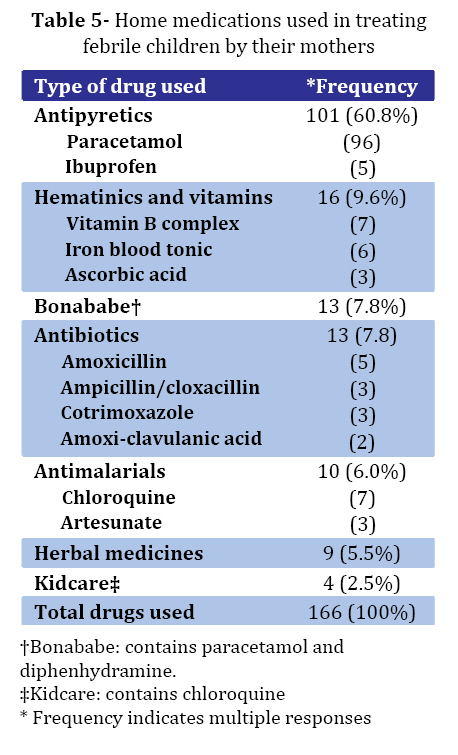
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 229-236 Fever in Children: Mothers' Perceptions and their Home Management Kazeem A Oshikoya1,2, MD; Idowu O Senbanjo2,MD, FWACP 1. Pharmacology Department, Lagos State University College of Medicine, Ikeja, Lagos, Nigeria Code Number: pe08036 Abstract Objective:A wide range of childhood illnesses are accompanied by fever, many of which are treated at home prior to presentation to hospital. An assessment of mothers’ knowledge and ability to recognize fever in their child, as well as management instituted at home were the focus of this study. Key Words: Fever; Children; Mother; Knowledge; Home management Introduction Fever is said to occur in children when the body temperature is above 370C (98.60F). It occurs when various infectious and non-infectious processes interact with the host’s defence mechanism[1]. In most children fever is either due to identifiable microbiologic agent or occurs during exposure to excessive environmental heat or during heavy physical work[2]. Fever from the latter causes is a passive rise in body temperature that subsides after a short time. Fever is one of the most common symptoms of childhood diseases. Malaria accounts for over 60% of outpatient visit in Nigeria and other Sub-Saharan African countries[3,4] and in areas with stable malaria or high transmission season like Nigeria, a recent history of fever is enough a criterion for diagnosis of uncomplicated malaria[5]. Fear and anxiety attached to fever by most mothers and some physicians are so much that it is labelled ‘Fever Phobia’[6-9]. One such fear is the belief that death may result from fever[6,7]. Many childhood febrile illnesses are treated at home prior to presentation[10]. This is a very common practice among caregivers in Nigeria[11-13] and other malaria endemic countries in Sub-Saharan Africa[14-16]. In Togo, only 20% of the children with suspected fever are seen at a health centre, while the remaining 80% are treated at home with an antimalarial drug[17]. In Nigeria between 60% and 80% of children would have been treated at home prior to reporting at health facilities[11]. Majority of these children are treated with antimalarial drugs. Going by the large population of children in Nigeria and a small proportion of health facilities available to cater for them, there is need to involve mothers in the management of minor diseased conditions presenting with fever. Such conditions include malaria and respiratory tract infections; the two common causes of fever in Nigerian children[14-16]. Roles of parents in the treatment of fever in their children could better be determined from their perception of fever and the understanding of its management. Health seeking behaviour had been shown in the past to be influenced by several factors such as: accessibility and availability of drugs; availability of health personnel; cost of treatment including drugs; perception of seriousness of the disease; knowledge of its cause and ability to diagnose and treat[18,19]. Most of these studies were community based in the rural areas and were carried out to evaluate home treatment of fever using household survey. This study was aimed at determining the knowledge and attitude of mothers in Lagos, an urban area in Nigeria, about fever in their children and how it was managed at home in this era of changes in the national policy for malaria treatment. Other purposes of this study were to determine the appropriateness of the home treatment, identify practices that were harmful, and to suggest more useful methods of fever management at home based on the findings from this study. Subjects & Methods Lagos is the smallest state but the most populous city in Nigeria with an estimated population of about 15 million inhabitants as of 1991 national census. It is divided into five divisions and twenty Local Government Areas (LGAs). Ikeja is one of the divisions and the state capital. It is also an urban area with so many industries and residents. LASUTH is situated in Ikeja and operates free health care for both paediatrics and geriatrics patients. Most of the children presenting to this hospital were self-presenting, the rest were referred from private hospitals/clinics and primary healthcare centres within and outside the state. One hundred and forty four mothers of children under the age of 12 years that were admitted to the children emergency room of LASUTH for various medical conditions were interviewed with a structured questionnaire by the researcher and two trained research assistants, who were staff of the pharmacology department, Lagos State University College of Medicine, Ikeja. Responses of the mothers were filled into the questionnaire by the interviewers because some of the mothers were illiterates and may not be able to read and fill the questionnaire appropriately. The study was done prospectively between July and December, 2006 and was approved by the ethical committee of LASUTH. All mothers whose children had fever as one of the presenting symptoms were interviewed. Mothers that did not give their consents were excluded. The questionnaire was divided into four sections. Section A and B were for the demographics of the mother and the child respectively. Section C was for the mothers’ knowledge of fever and section D for its management. The questionnaire was pre-tested at the children emergency room a month before the study was commenced. Data analysis was by SPSS version 13 and data expression was in percentages. Findings Demography of the mothers and their children: Sixty-three mothers (43.8%) were between 21- 30 years. Their levels of education ranged from illiteracy 30 (20.9%) to above secondary/high school 87 (60.5%). The majority of the mothers had 2 children (31.2%). Only three (2.1%) had more than 6 children. Their occupation varied from petty trading 42 (29.2%) to civil service 6 (4.2%). Few (10.4%) of the patients were neonates, 42 (29.2%) were aged 1-6 months, 54 (37.5%) were 1-6 years. Majority (61.8%) of them were males. Onset of fever in the patients, before presenting to the hospital, ranged from 6 hours (2.1%) to 14 days (27.1%). Temperature of the patients ranged from normal (16%), below 40oC (34.7%) to high grade (49.3%). Mothers’ knowledge of fever: Fever was perceived by 83.3% mothers as hotness of the whole body of the patient. Only 2.1% could not explain fever. The possible causes of fever was ascribed to infection by 63 (43.8%), teething by 48 (33.3%) and common cold by 24 (16.7%) mothers (Table 1). Perceived symptoms associated with fever were highlighted in Table 2 as decreased appetite (47.9%), vomiting (43.8%), decreased activity (37.5%), and shortage of blood (2.1%). Majority of the mothers believed convulsions (75%), loss of consciousness (22.9%) and irrational talk (27.1%) could result from fever. Death (31.3%), brain damage (31.3%), mental retardation (27.1%), paralysis (18.8%) and blindness (10.4%) are other indefinable effects of fever. Only (8.3%) mothers thought fever was harmless. Fever was detected by 120 (83.3%) mothers by feeling the skin of the patients with their back-hand and thermometer 24 (16.7%). Touching the forehead, chest and all the limbs of the patient with the hands was used to detect fever in 4.2% cases. Change in the facial look of the child was attributed to fever in three cases. Majority (75%) of the mothers that used thermometer to detect fever were able to correctly use it by cleaning the thermometer with savlon solution (n-propyl alcohol- 2.84% m/v, chlorhexidine gluconate-0.3g and centrimide-3.0g) or methylated spirit before and after use, shaking it very well before use, inserting it either in the armpit or anus, and allowing a contact time of at least 5 minutes before the thermometer is read. Normal body temperature was considered 36oC to 37oC with thermometer use. Ninety three mothers (64.6%) were informed about fever from health education talks at clinics/hospitals. Television and radio programmes (8.3%), newspapers and magazines (8.3%) and billboard adverts were the other sources of information to the mothers about fever. Mothers’ presumptive diagnosis of fever in their children is represented by Table 3. While malaria 78 (54.2%) was diagnosed most, 33 (22.9%) mothers were not sure of the diagnosis. The physicians’ diagnosis of the febrile condition was as shown in Table 4. Malaria was diagnosed in 68 (47.2%) patients: acute uncomplicated malaria (44.1%), severe malaria with anaemia (45.6%) and cerebral malaria (10.3%), followed by meningitis 21 (14.6%), bronchopneumonia and septicaemia 20 (13.9%) respectively. Management of fever by the mothers: Majority of the mothers 96 (66.7%) managed the fever at home. Only a few mothers (20.1%) correctly managed the fever by taking their children to hospital and primary health care centre. Taking the child to a chemist (4.2%), laboratory for investigation (2.8%), self medication (2.1%) and laboratory with self medication (2.1%) were the alternative methods of home management of fever by the mothers. All the 96 mothers involved in self management of the fever were involved in self medication. Supportive ways of fever management at home adopted by the mothers include reducing clothing and exposure to air (91.7%), tepid sponging (90.1%), cold bath (67.7%), fanning (9.4%), and taking a harmful step by wrapping the child up with a blanket (4.2%).Drugs used at home by mothers to treat fever in their children: Table 5 shows the list of self medicated drugs in fever management in the children. All the children with fever were given paracetamol. Antimalarials (6.0%) and antibiotics (7.8%) were the other major group of drugs used by the children. With regards to the number of children that were given drugs at home, 10.4% and 13.5% were treated with antimalarials and antibiotics group of drugs respectively. Oral herbal preparations were used by six of the children and topical herbal preparations were applied to the whole body of three of the children. Remnant of the previously used paracetamol that was kept at home was administered to 54 (56.3%) children with fever. Among those parents that administered paracetamol to their children, only 9 (9.4%) were able to identify liver problems as their potential adverse effects. Three of the five mothers were able to identify gastritis as a potential adverse effect of ibuprofen. Of the 13 mothers that administered antibiotics to their children, deaths and skin rashes respectively (46.2%), convulsion (38.5%), diarrhoea (30.8%), and skin peeling (23.1%) were the identified potential adverse effects of the drug. Discussion Previous studies in both Nigeria and other African countries on home management of fever in children concentrated on fever as a result of malaria[10,11,12,17,20-23], moreso those studies were done in the era when chloroquine and sulphadoxine/pyrimethamine were the first line of treatment. This study has however evaluated home management of fever in children; irrespective of the cause, in the era when artemesinin based combination therapy (ACT) remains the first choice of malaria treatment in Sub-Saharan African countries; endemic areas for resistant malaria. The results of this study have further reiterated that most childhood fever are first treated at home by their mothers or care givers. Help was sought thereafter if the fever was unremitting despite the initial treatment or complication sets in. Similar reports to this have been widely published in other studies from Nigeria[10,11,12]. Contrary to the reports of previous studies in urban areas of Uganda and Nigeria, mothers in this study were quite knowledgeable of the definition of fever, causes and associated symptoms[10-12,18]. This might be as a result of a larger percentage of the mothers (60.4%) being educated up to secondary level and beyond. Our findings however agree with the results of studies from Kenya, Togo, Ethiopia, and Sri Lanka[20-24]. Further analysis of the mothers’ knowledge of fever showed that they were able to correctly perceive fever in their children using their hands or thermometer which was corroborated by the 80.0% of the children presenting to the CHER with temperature above normal values. Also their knowledge of convulsion being a major consequence of fever is highly commendable. These findings are similar to the reports from Ethiopia[24] and Iraq[25] which may be a reflection of their level of education and their reliable sources of information about fever. The 54.2% mothers that made a presumptive diagnosis of malaria were less than the 47.2% children with fever that were diagnosed of malaria on admission to CHER (Table 3 and 4). Malaria being diagnosed most by both the mothers and the physicians further support the results of other studies that had reported malaria as a major ailment affecting most children in Nigeria[4,10-12,26-28]. It further corroborates the good knowledge of the mothers about malaria fever earlier observed in this study. However, the mothers were unable to identify the severe forms of malaria (malaria with anaemia and cerebral malaria) that carry a high morbidity and mortality in children. Similarly, mothers’ overdiagnosis of malaria can cause other life threatening conditions that require urgent medical attention, such as septicaemia, bronchopneumonia and meningitis that afflicted 42.4% of the children to be missed out by the mothers and further delay their treatments. This therefore calls for further education to the mothers on how to recognise malaria with complications and other life threatening conditions that may mimic malaria so as to present their child early to the hospital. In Mali[23] and Nigeria[10-12] mothers managed their child’s fever at home similar to our finding of 66.7% children treated for fever at home. Antimalarials (chloroquine and sulphadoxime/pyrimethamine) were the drugs used in home treatment of fever from previous studies[10-12,26-28], but contrarily paracetamol was the most commonly administered drug to the children in this study, despite the presumptive diagnosis of malaria by most of the mothers. Antimalarials (6.0%) and antibiotics (7.8%) were seldom used. This must have been as a result gradual phasing off of chloroquine and sulphadoxime/ pyrimethamine in the market, lack of awareness of artemesinin based combination drug as the recommended first line drug for malaria treatment or the exorbitant cost of the artemesinin based drug combination in the open market. The non use of antimalarials in the febrile children might explain the progression of some the uncomplicated acute malaria to severe malaria with anemia and cerebral malaria observed in this study. These findings therefore suggest that more studies need to be done to assess the acceptability of ACT by Nigerian mothers and the effect of its cost on home management of fever in children. Surprisingly, free malaria treatment policy is being practiced in all the government hospitals in Lagos where this study was conducted, and ACT was the choice of drug. In spite of this only 2.1% of the children presented early to the hospital (within 6 hours of fever onset). The attitudes of the mothers therefore negate the effort of the government at reducing child mortality and morbidity; through free health care for children, thus increasing the burden of illness in the hospital and overstretching the inadequate health facilities. Therefore one of the limitations of this study is our inability to evaluate the factors that prevented the mothers from presenting early to the hospital. Home use of antibiotics as observed in this study is of great concern. The 13.5% antibiotics utilization rate in this study is lower than 31.3% previously reported in Nigeria[10] and much lower than 62.0% reported in Iraq[25]. The implication of this is that the children are at risk of developing adverse reactions since antibiotics constitute the leading cause of moderate to severe adverse drug reactions in children[29]. Also the potential for antibiotic resistance and treatment failure is high in these children; this may possibly explain the prolonged treatment and morbidity that were observed in the children from this study treated for bronchopneumonia and meningitis. In addition to administering paracetamol to all the children with fever by their mothers, other methods of reducing fever, such as reducing the clothing and exposing the child to air, tepid sponging, and cold bath, were well practised by the mothers, thus reducing the risk of convulsion and its attending risks in the children. Similar reports had been made in various studies on fever management in children in Nigeria[10,11,28]. Remnant of the previously used paracetamol that was kept at home was used in 56.3% children with fever. Drugs kept in home in a temperate weather are known to be ineffective as a result of loss of potency, besides their metabolites are known to be toxic[30]. This in addition to not treating the underlying cause of fever might explain the unremitting fever observed in these children when they presented to the CHER. Most of the mothers did not use the paracetamol correctly with respect to the dose and frequency of use. The use was associated with overdosage error. This might be as a result of lack of the mothers’ knowledge of the potential adverse effects of paracetamol. We have earlier reported overdosage error from paracetamol use in children[31], thus the children are the risk of liver problem from irrational use of paracetamol[32]. This study was done in an urban setting; the situation may be very different in a rural setting where people are at disadvantages of good health care facilities, quality education, and poverty. Similar study in the rural setting is suggested so as to achieve generalized application of the observed interventions of fever home managements. Conclusion This study has highlighted home management of fever amongst children from an urban area of Nigeria by their mothers/caregivers. Malaria, being a major cause of fever in the children, requires mothers/caregivers to be educated and provided guidelines on its early recognition; through symptoms and signs, appropriate diagnosis and treatment with artemesinin combination therapy. There is need to create more awareness on the use of artemesinin combination therapy amongst the mothers as the choice of malaria treatment in children. Mothers need to also be educated on when to consult health facilities should home treatment of malaria fails or the presenting symptoms and signs go beyond those of malaria. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08036t5.jpg] [pe08036t4.jpg] [pe08036t3.jpg] [pe08036t1.jpg] [pe08036t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}