 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
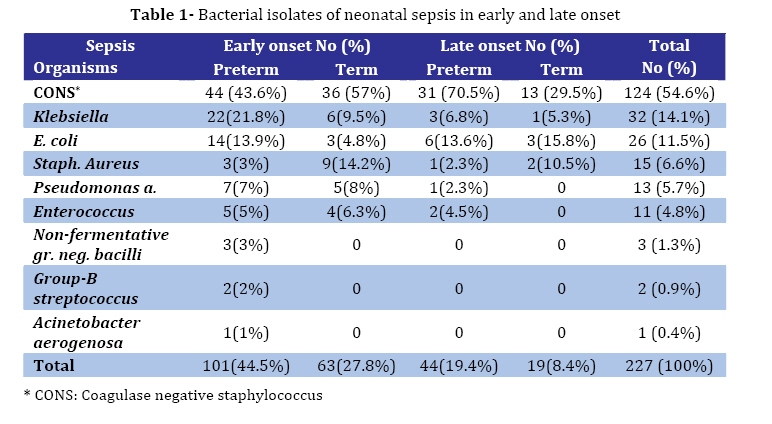
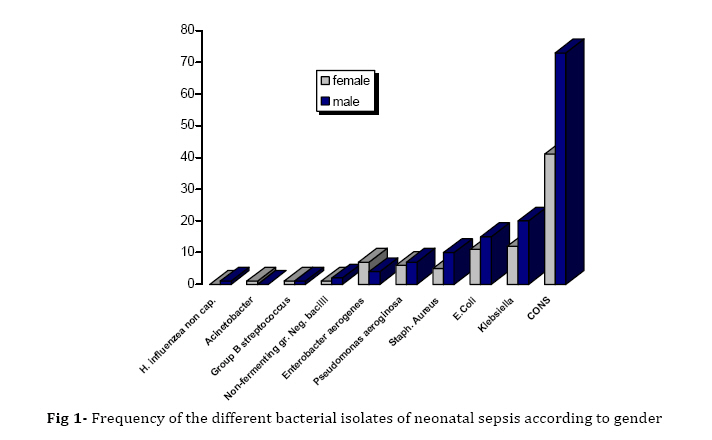
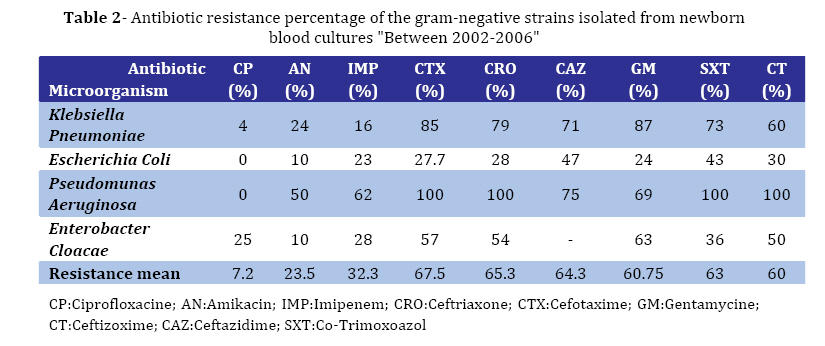
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 237-243 Coagulase Negative Staphylococcus; the Most Common Cause of Neonatal Septicemia in Urmia, Iran Shahsanam Gheibi1, MD, Pediatric Gastroenterologist; Zahra Fakoor1, MD, Neonatologist; Mohammad Karamyyar1, MD, Pediatric Infectious Diseases Specialist; Javad Khashabi1, MD, Pediatrician; Behrooz Ilkhanizadeh2, MD, Pathologist; Farzin Asghari-Sana3, MSc, Microbiologist; Hashem Mahmoodzadeh1, MD, Pediatric Nephrologist; Amir Human Majlesi1, Pediatrician 1. Department of Pediatrics, Urmia University of Medical Sciences, IR.Iran Code Number: pe08037 Abstract Objective: A prospective study to determine the prevalent bacterial agents of neonatal sepsis and their antimicrobial susceptibility in Imam Khomeini teaching hospital, Urmia, from Oct 2002 to Nov 2006. Key Words:Septicemia;Neonatal sepsis; Antibiotic sensitivity; Coagulase negative staphylococcus Introduction Sepsis neonatorum is the term used to describe any systemic bacterial infection documented by a positive blood culture in the first month of life[1]. Neonatal septicemia remains one of the important causes of mortality and morbidity despite considerable progress in hygiene, introduction of new and potent antimicrobial agents and advanced measures for diagnosis and treatment[2]. Up to 10% of infants have infections in the first month of life[3] which are responsible for 30-50% of total neonatal deaths in developing countries[4]. Neonatal sepsis can be classified into two relatively distinct illnesses based on the postnatal age at onset. Early-onset sepsis occurs in the first 7 days of life, is usually a fulminant and multisystemic infection; and has a higher case fatality rate than late-onset sepsis. Late-onset sepsis is usually more insidious but may have an acute onset[1]. Bacterial pathogens of neonatal septicemia may vary from one country to another and within a country from one hospital or region to another[5]. These organisms may even vary at different times within the same place[6,7]. In developed countries Group B streptococcus (GBS), E. coli and Listeria monocytogenes are the most common causes of neonatal sepsis, however, in developing countries, these bacteria are replaced by gram-negative bacilli, Coagulase negative staphylococcus (CONS) and others[8]. Over the last two decades most of the organisms have developed increased drug resistance and management of the patients is becoming a major problem[9]. Identification of the etiology is important since it can induce a change in management policy[5]. For effective management of neonatal septicemia with appropriate antibiotics that would minimize the risk of severe morbidity and mortality besides reducing the emergence of multi-drug resistant organisms by rational antibiotic use, study of bacteriological profile and their antibiotic sensitivity pattern plays a significant role[1,10]. The present study was carried out to determine the bacteriological profile with antibiotic sensitivity pattern of neonatal sepsis in our hospital. Subjects & Methods This was a prospective cross- sectional study of 2325 out born newborns with symptoms and signs suggestive of neonatal sepsis (poor feeding, respiratory distress, fever, hypothermia, gastrointestinal and/or central nervous system symptoms) that were admitted during a 50-month period (October 2002 - November 2006) in neonatal ward of Imam Khomeini teaching hospital, Urmia, Iran. The ethics committee of university approved the study. Early onset neonatal sepsis (EONS) and late onset neonatal sepsis (LONS) were defined as illnesses appearing from birth to seven days and from eight to twenty-eight days postnatal respectively. Infections that occurred at least 48h post hospitalization were assumed to have been acquired and considered hospital infections. Two blood cultures, complete blood count (CBC), erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), blood sugar, electrolytes, cerebrospinal fluid (CSF) and urine analysis/culture and chest X-ray were attained in all cases of suspected neonatal sepsis. Standard procedure of sample collection and culture was undertaken with aseptic precautions. For blood cultures two samples of 1 ml blood[1] were taken from two different sites, inoculated in trypticase soy agar, incubated at 35-37˚C and examined daily for evidence of bacterial growth. Sensitivity of the bacterial isolates to different antibiotics was determined using standard disc diffusion (SDD) method[11]. When growth appeared, the culture was inoculated into a blood agar plate and a gram-stained smear was examined. Antibiotic sensitivity was tested for ampicillin, gentamycin, amikacin, oxacillin, vancomycine, ceftriaxone, cefotaxim, ciprofloxacin, ceftizoxim, ceftazidim and imipenem. Blood cultures positive for corynebacterium sp, bacillus sp, streptococcus viridans and coagulase negative staphylococcus generally were considered to be contaminants, except when two positive blood cultures and/or evidence of a true infection based on clinical course and laboratory data existed. For all of other pathogens, infection was confirmed by the presence of the organisms in even one blood culture. After taking blood samples, the therapy was empirically started with ampicillin and gentamycin intravenously. Specific antibiotic therapy was given after the culture report was available. Findings Among 4827 newborn admissions 2325 neonates screened for sepsis, there were 258 (11%) positive blood cultures. Thirty-one single positive blood cultures for CONS were excluded as contamination. Sixty- three (27.7%) neonates had LONS and 164 (72.2%) EONS. In the 36 episodes of proven nosocomial infection (primary negative blood culture followed by secondary positive blood culture at least 48 h post hospitalizations); gram-negatives were the commonest (66%) organisms. Among this group pseudomonas spp. has been found to be predominant pathogen (33%) and the rest included Klebsiella (22%), Enterobacter species (5%) and E.coli (5%). The CONS was responsible for 27 percent of nosocomial infections. The bacterial etiologies of EONS and LONS for term and preterm newborns are shown in Table 1. Eighty-five newborns were female and 142 were male; the male: female ratio was 1.67:1. A total of 63.9% patients were premature (145/82). CONS was the commonest cause of both early (48.8%) and late onset (69.8%) neonatal sepsis followed by Klebsiella, E coli and Staphylococcus aureus (Fig 1). The gram positive strains showed high degree of resistance to commonly used antibiotics such as ampicillin (87.5%), cefotaxim (50.15%), Ceftriaxon (42.5%) and gentamicin (38%). Low resistance to vancomycine (10%), ciprofloxacin (21.5%) and imipenem (26%) was seen in this group of bacteria. There was high sensitivity to ciprofloxacine (92.8%), amikacin (76.5%) and imipenem (67.7%) among gram negative organisms and comparatively high resistance to cefotaxim (67.5%), ceftriaxone (65.3%) and ceftazidim (64.3%). The sensitivity patterns of gram-negative strains are given in Table 2. Discussion In Urmia, there is no previous prospective study of the etiology of neonatal sepsis. Since the bacterial pathogens responsible for neonatal sepsis tend to change over time, and most of the organisms have developed increased drug resistance, this study was conducted to determine the frequency and patterns of antimicrobial resistance of microorganisms associated with sepsis cases among newborns in Urmia city, Iran, during a four-year period. In the present study, the overall sepsis rate of 4.7 percent of all admissions fall within the range quoted in the literature[9]. Of the 2325 neonates screened for sepsis, there were 258 (11%) positive blood cultures, which is quite low as compared to other studies[2,4,12,13]. Low blood culture isolation rate in this study might be due to several reasons, e.g. administration of antibiotics before blood collection either to the mother or to the baby[14], or the possibility of infection with viruses, funguses or anaerobes[15], which cannot be ruled out. Some of these patients may have metabolic disease[16,17], inappropriate blood sampling or culture technique[18]. Moreover, negative blood cultures do not exclude sepsis. We found that EONS was more common than LONS which is compatible with other reports from Iran, India and Pakistan[6,10,15,19,20], but in contrast with a report from Bangladesh, Australia and Tehran, that LONS was more common[2,21-24]. Gram-positive organisms constituted the major group of isolates (62.1%) from neonatal septicemia cases. Among this group CONS was the commonest cause of both early and late onset neonatal sepsis(54.6%) and the rest included staphylococcus aureus (6.6%) and group B streptococcus (0.9%). The predominance of gram positives corroborates the findings of other workers[20,25-31]. Other authors[7,20,24,28] have reported increasing trend of CONS in neonatal sepsis, even in our hospital in 2001 it has been reported to be 30%[25]. Pro-inflammatory responses to S. epidermidis are dependent on gestational age in preterm infants[32], thus the predominance of neonatal sepsis in preterm newborns in our study may be one reason to this finding.The variance of bacteriologic growth is not clear but it may be the population difference with regard to the maternal colonization rate, nosocomial acquisition of bacteria by the mother and the neonate, genetics of the immune response in selected population groups[6]. A comparatively low incidence of Group B streptococcus, unlike in western countries[33,34], has been observed in our study, which correlates well with the findings from Nigeria, Bangladesh, Pakistan and other sites in Iran[2,6,35,36]. This highlights the importance of local epidemiology of neonatal sepsis to formulate antibiotic policy[6]. The results of antibiotic sensitivity (Table 2) revealed that minority of gram negative isolates were sensitive to ceftriaxone, cefotaxime and ceftazidine; whereas majority of Gram positive isolates showed sensitivity to vancomycine, ciprofloxacine and imipenem. These findings were compatible with other studies[9,14,37]. The antimicrobial sensitivity pattern differs in different studies as well as at different times in the same hospital[12]. This is because of emergence of resistant strains as a result of indiscriminate use of antibiotics. The high resistance rates found in this study may be associated with the frequent use of antimicrobial drugs for both prophylactic and therapeutic treatment of hospitalized newborns[14]. In view of the above facts the strategy of antibiotic usage in neonates should be reviewed periodically even in the same hospital. Therefore, the appropriate empiric regimen seems to consist of vancomycine + amikacin until culture results arrive. Also in Karachi in view of the isolation of highly antibiotic resistant organisms, vancomycin in combination with amikacin or a carbapenem is suggested to be the drug of choice for empirically treating neonatal sepsis[38]. The main shortcoming of this study is the lack of MIC values. Conclusion CONS and Klebsiella Pneumoniae together with E.Coli are the leading causative agents of neonatal sepsis in our unit. They were resistant to commonly used antibiotics, thus due to antibiotic sensitivity results, appropriate initial empirical antibiotic therapy for neonatal sepsis should be replaced. Every unit should carefully follow the bacterial spectrum and resistance patterns of microorganisms responsible for neonatal infections to design a specific empirical antibiotic regimen for unit. Acknowledgment We gratefully acknowledge Urmia University of Medical Sciences for the financial support. We thank Mrs. Haji-mohammadian, and Mrs. P. Hashemi, Miss R. Poorakbar, and Mr. Y. Sharifi for their assistance in data collecting and preparation of this manuscript. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08037t1.jpg] [pe08037f1.jpg] [pe08037t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}