 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
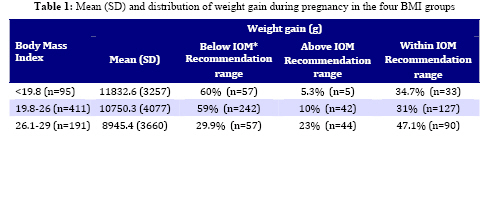
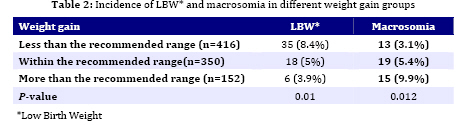
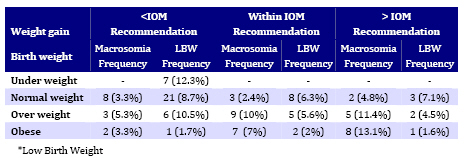
Iranian Journal of Pediatrics, Vol. 19, No. 1, March, 2009, pp. 18-24 Gestational Weight Gain and Fetal Birth Weight in Rural Regions of Rasht/Iran Zahra Panahandeh, MD 1. Department of Community Medicine, Guilan University of Medical Sciences, Rasht, Iran Received: 23/04/08; Revised: 10/06/08; Accepted: 19/12/08 Code Number: pe09003 Abstract Objective:Proper nutrition during pregnancy is essential for optimal fetal growth. Investigation of the relation between pregnancy weight gain and birth weight in rural regions of Rasht, center of Guilan Province in Iran, was the purpose of this study. Key Words: Low birth weight; Macrosomia; Pregnancy; Body mass index Introduction It is proved that proper nutrition during pregnancy is essential for optimal fetal growth and development. Poor maternal nutritional status leads to many complications for both mother and baby[1,2]. The Institute of Medicine (IOM) issued its weight gain guidelines for maternal weight gain during pregnancy in 1990. These guidelines are based on pre-pregnancy body mass index (BMI)[3,4,5]. According to these recommendations women who are underweight before pregnancy should gain more and overweight women should gain less weight during pregnancy[1,4]. In some studies, association between pregnancy weight gain within the IOM's recommended ranges and the best outcomes for both mothers and infants have been shown. Based on these observational studies, we can conclude that maternal weight gain strongly correlates with birth weight. They found that pregnancy weight gain below the recommended range was associated with low birth weight (LBW= birth weight less than 2500 g) and preterm birth, and weight gain above the recommended range was associated with birth weight more than 4000 g or macrosomia, cesarean delivery and postpartum weight retention[1,3,4,6,7]. However, it seems that many pregnant women are not aware of these guidelines and also many healthcare professionals may not be aware of specific nutritional recommendations on how to achieve a healthy pregnancy outcome[1]. In an observational study in urban health centers in Rasht, north of Iran, 60% of women with normal weight and 56.7% of the underweight women had weight gain less than the lower cutoffs of IOM recommendations[8]. In Iran, pregnant women regularly attend local health centers in rural regions. However, relatively little is known about maternal weight gain and fetal outcome based on the IOM guidelines in this country. The aim of this study was to investigate the relation between pregnancy weight gain and fetal birth weight based on IOM recommended weight gain in rural regions of Rasht, center of Guilan province in north of Iran. Subjects & Methods In this cohort study, prenatal data of 954 pregnant women were recorded by rural health workers. These women regularly attended rural health centers of Rasht for prenatal care and delivered between April 2005 and March 2006. Women over 18, with singleton full term pregnancies (delivering after 37 weeks of gestation) were included. The subjects having high risk pregnancies, any underlying systemic disorder such as anemia, hypertension, diabetes mellitus, or complications of pregnancy were excluded from the study. Information about maternal age, educational level, working status, pre-pregnancy weight, height, total weight gain during pregnancy, and birth weight were recorded for analysis. Maternal height and weight and birth weight of newborns were measured using Seca scale accurate to 1 cm and 0.1 kg, respectively. Total pregnancy weight gain was defined as the difference between the final recorded maternal weight at the last prenatal visit and the maternal pre-pregnancy weight recorded at the first prenatal visit in the local health center. The first visit was not later than the first month of pregnancy. BMI [weight(kg)/height(m2)] was calculated from maternal pre-pregnancy weight and height data. According to the Institute of Medicine (IOM) recommendations the subjects were stratified based on their pre-pregnancy body mass index into four groups: BMI <19.8 kg/m2 (underweight women), BMI 19.8-26.0 kg/m2 (women with normal weight), BMI 26.1-29.0 kg/m2 (overweight women) and BMI >29.0 (obese women).Based on the IOM guidelines, underweight women should be advised to gain 12.5 to 18.0 kg, women with normal weight to gain 11.5 to 16.0 kg, overweight women to gain 7.0 to 11.5 kg, and obese women to gain minimally 6.8 kg[8]. According to the total pregnancy weight gain, women were categorized as less than, within and above the IOM recommended weight gain in the four BMI groups. Because the IOM did not recommend an upper limit of weight gain for obese women, if weight gain of obese women was at least 6.8 kg, but did not exceed the upper limit (11.5 kg) for overweight women, they were classified as meeting the IOM recommendations. Neonatal birth weight less than 2500 g was considered as LBW and above 4000 g was considered as large baby or macrosomia[4]. We used SPSS 11.5 software for statistical analysis. Statistical methods were the Chi-square test, independent t-test, Pearson correlation and logistic regression with 95% confidence intervals (CI). In logistic regression we controlled for potential confounders, including maternal age, maternal height, pre-pregnancy weight, pre-pregnancy BMI, maternal education, maternal occupation, and pregnancy weight gain according to the recommended range (less than, within and above the recommended guidelines) for prediction of low birth weight. Samples enrolled in this study received the standard prenatal care and the study was approved by the Committee of Investigations at the Medical Faculty of the Guilan University of Medical Sciences. Findings A total of 918 women met our inclusion criteria. The subjects were between 18-45 years old with mean age of 26.45±5.43 years. Among them, 95.4% were housewives and 4.6% were employed. Most women (90.6%) were intermediately educated (with a 6-12 year education), 5.2% were less educated (educated <6 years) and 4.2% were highly educated (educated >12 years). Results of our study showed that 10.3% of women were underweight (BMI <19.8), 44.8% were women with normal weight (BMI=19.8-26), 20.8% were overweight (BMI=26.1-29) and 24.1% were obese (BMI>29). Average of total pregnancy weight gains was 10166.5±4009.5 g and 45.3% of women gained weight less than, 38.1% within, and 16.6% higher than the IOM recommended weight gain. Table 1 (table 1 con't) shows means and distribution of weight gain during pregnancy in the four BMI groups. Pearson correlation showed a negative relation between pre-pregnancy body mass index and total pregnancy weight gain (r=-0.22, P=0.01). The rate ofmaternal weight gain during the entire pregnancy was significantlycorrelated with birth weight (r=0.10; P<0.01) and also there was a significant positive correlation between pre-pregnancy BMI and birth weight (r=0.11; P<0.001). More than 50% of underweight women and women with normal weight and almost 30% of overweight and obese women gained weight less than the IOM recommended weight gain. Rate of weight gain more than IOM recommendations in overweight and obese women was higher than underweight women and women with normal weight. In our study, 7.1% of neonates were less than 2500 g (with LBW) and 5% were more than 4000 g at birth. Mean weight gain of women with an infant with LBW was significantly less than mean weight gain of women who had an infant with a birth weight more than 2500 g (P=0.002). Results in Table 2 show that women who gained weight less than the recommended weight had higher rate of neonate with LBW compared with women who gained weight according to or above the IOM recommendations (P=0.01). Women gaining weight above what is mentioned in IOM guidelines had higher rates of macrosomia than women gaining less than or within the mentioned weight gain in IOM guidelines (P=0.012). Results in Table 3 show that the incidence rate of LBW in underweight women who gained less than what should be according to IOM guidelines was 12.3%, and none of them with a weight gain within or above the recommended weight gain by IOM had a low birth weight neonate; also, none of these women had an infant with a birth weight more than 4000 g. Moreover, in women with normal weight, overweight women and obese women, the incidence of LBW decreased when these women gained weight within or above the recommended range, but the incidence of macrosomia increased in subjects who gained weight above what is mentioned in the IOM recommendations (not significantly). In this study, results from the logistic regression analysis showed that the only predictor for low birth weight was the pregnancy weight gain less than what should be according to IOM guidelines and odds ratio (OR) for LBW in the women who gained weight less than the recommended range was 2.79 (CI=1.16 -6.73, P0.02). Discussion In this cohort study, we evaluated gestational weight gain and birth weight in a sample of normal pregnancies with singleton term births in rural regions of Rasht, north of Iran. Previous studies support that pre-pregnancy BMI and gestational weight gain influence infant birth weight and play significant role in adverse pregnancy outcomes including LBW and macrosomia[9-13]. Results of our study showed that although close to half of women (45%) entered pregnancy with high BMIs (BMI >26), 23% of the overweight (BMI=26.1-29) and also 28% of the obese subjects (BMI >29) gained weight above the IOM recommendedrange, which likely increased their risk of obesity and itsassociated chronic diseases and also macrosomia[14]. Although birth weight markedly improved in overweight groups when weight gain increased from below than the IOM recommended range to within it, rate of LBW was slightly decreased, and macrosomia increased when they gained weight more than the recommended range (11.5 kg). It had been shown that a large weight gain increased the risk of delivery complications such as cesarean delivery even in the absence of macrosomia[5], so these women should gain weight within the recommended range. Findings of our study also indicated that obese women should not gain more than 7 kg, because this would increase the incidence rate of macrosomia without significant decreasing of the incidence of low birth weight (Table 3). Results of other studies support the need to balance gestational weight gain against the risk of LBW and macrosomia among underweight and obese women, respectively[14,15], and women at extremes of the pre-pregnancy BMI and prenatal weight gain, such as women with a low BMI and under recommended weight gain[13,16], and also women with high BMI and more than recommended weight gain are at higher risk for adverse birth outcomes as indicated by birth weight[16]. Results of our study showed that one-tenth of the women in the study were underweight and 45% were with normal weight when became pregnant, but like another study in urban health centers of Rasht[8], thevast majority (60%) of the underweight women and women with normal weight gained weight less than the recommended range, which likely increased the risk of LBW. Although findings of our study showed that a weight gain within and above IOM recommended range in underweight women led to a reduced incidence of LBW and did not increase the rate of macrosomia, previous studies have shown that gaining weight more than the IOM recommended rangeincreases the risk of being overweight after pregnancy[17,18]. In this study, a large weight gain in women with normal weight increased the rate of birth weight more than 4000 g, but the incidence of LBW did not decrease (Table 3). In other researches, the frequency of complications was lowest in the groups with normal weight and withthe recommended IOM weight gain[19,20]. Therefore, our results suggest that in women with normal weight, weight gain should not exceed the IOM recommended weight gain. Some limitations to our study should be considered when interpretingthese results. We analyzed the incidence of LBW and macrosomia in four BMI groups based on their total weight gain during pregnancy, but because we excluded complicated pregnancies from this study, the small sample sizes for analyses of birth weight less than 2500 g and more than 4000 g reducedour ability to detect differences in these variables when subjectswere stratified by BMI and weight-gain category. In our study, women who gained weight less than the recommended weight during pregnancy, regardless of their pre-pregnancy weight, were at greater risk of low birth weight (P=0.01), and this is similar to the results of previous studies[6,21-23]. There was a significant difference between mean weight gain of women with low birth weight and mean weight gain of other women who had an infant with a birth weight more than 2500 g (P=0.002). Our findings showed that pre-pregnancy BMI and total gestational weight gain were positively associated with infant birth weight (P<0.001 and P<0.01, respectively), and weight gain less than what is recommended in the IOM guidelines was the only predictor of LBW (P=0.02). It was shown in an observational study that if women were advised about physical activity and dietary habits from their physicians or other health care professionals during pregnancy, it was possible to limit maternal weight gain to the recommended range[22]. In rural regions of Iran, pregnant women are regularly visited by local health workers and healthcare providers who recommend them to be on a healthy diet and gain appropriate weight during pregnancy. However, to gain appropriate weight in pregnancy, they need to give women the tools and direction to do so properly. Conclusion Pregnancy weight gain less than the IOM recommendations range is a predictor of LBW, regardless of the pre-pregnancy BMI. All pregnant women should receive adequate advice concerning pregnancy weight gain during prenatal visits. Acknowledgment We thank Health Deputy of Guilan for their support for data collection and Monirosadat Hosseini for coordinating health workers in our study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences,All rights reserved. The following images related to this document are available:Photo images[pe09003t1b.jpg] [pe09003t3.jpg] [pe09003t1a.jpg] [pe09003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}