 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
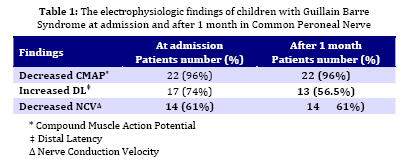
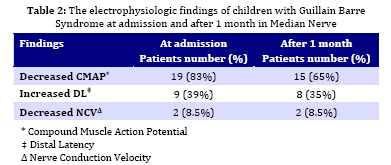
Iranian Journal of Pediatrics, Vol. 19, No. 1, March, 2009, pp. 52-58 Acute Inflammatory Demyelinating Polyneuropathy in Children; Clinical and Electrophysiologic Findings Farhad Mahvelati Shamsabadi1, MD; Parvaneh Karimzadeh1, MD;Seyed-Hasan Tonekaboni1, MD; Javad Ghorobi2, MD 1. Department of Child Neurology; Shahid Beheshti University of Medical Sciences, Tehran, IRIran Received: 31/05/08; Revised: 15/12/08; Accepted: 04/01/09 Code Number: pe09008 Abstract Objective: The aim of this study was to evaluate the electrophysiologic findings of Guillain Barre Syndrome (GBS) in children and their relation with clinical progress of the disease. Key Words: Guillain Barre Syndrome; Electrophysiologic evaluations; Acute flaccid paralysis; Acute inflammatory demyelinating polyneuropathy Introduction Guillain Barre Syndrome (GBS) is an acute polyradiculopathy which is quite common in all ages. With the gradual eradication of poliomyelitis due to immunization, it is now the most frequent cause of acute flaccid paralysis in most countries[1,2]. The diagnosis of GBS was based on clinical features[3], supported by features of electrophysiologic study. The best method of diagnosis of this syndrome is nerve conduction study. Specific evaluations of the syndrome in children have not been so far performed[4]. The electrodiagnostic findings in these patients include acute demyelinating neuropathy, acute axonal neuropathy, or a combination of these two[5,6,7]. Most of our knowledge of Guillain Barre variants has come from studies in several western series. However, different populations around the world would have different clinical and paraclinical findings. Determining these differences would be the first step in the further understanding of pathogenesis and help in identification of the risk factors for the development of the disease. There are few studies on pediatric GBS in Iran[8-11]. In this study, we evaluated the frequency of electrophysiologic findings of the disease [including distal latency (DL), nerve conduction velocity (NCV), compound muscle action potential (CMAP)] in children with GBS and then evaluated the relation between each of these findings and the severity of the disease. The relation between the disease prognosis and denervation is another factor in electromyography (EMG) which was evaluated, as well. Subjects and Methods All 23 1-15-year-old children with GBS who were referred to Mofid hospital between January 2005 and January 2007 were enrolled in this study. Patients fulfilled the clinical criteria for GBS[3]. All patients were reviewed clinically by a child neurologist. The electrodiagnostic evaluations were performed 2 times with a 1-month interval (the first evaluation was performed at admission). This was done to define the electrodiagnostic findings in the very early state and to follow the evolution of electrodiagnostic abnormalities. This 1-month interval was chosen based on previous studies[5,12]. For the children with cardiovascular problems or in need of ventilator, we had to wait before the primary evaluations, because the room we performed the evaluations in, was situated on the first floor and the ICU was on the 3rd floor and moving the patient was potentially dangerous. Averagely, the first evaluation was performed on the first 10 days after the initiation of the symptoms (range 2 to 30 days). The second evaluation was performed 4 weeks later (28±4 days). The severity of the disease is defined by disability scale of Hughes and colleagues as; G0, complete health; G1, least clinical findings; G2, the patient walks 5 meters independently; G3, walks 5 meters with help; G4, cannot walk 5 meters without help; G5, needs ventilator; and G 6, death[13]. Electrophysiological studies are performed with a four-channel intelligent nerve-induced electromyography machine (Phasis, Italy). The evaluations were carried out by a child neurologist and an experienced specialist in physical medicine. Nerve conduction studies were performed on 3 nerves; common peroneal nerve, median nerve (motor nerves), and sural nerve (sensory). Regarding the approximately symmetric involvement of the disease in the patients, all evaluations were performed on the right side of the body. Three factors were recorded for motor nerves: NCV, CMAP, and DL. The evaluations were performed with the standard method of surface electrode on the forearm and calf. For sural nerve, only DL was evaluated. F wave was also evaluated only in the lower extremity regarding its latency. CMAP amplitudes were measured from baseline to negative peak. The ratio of proximal to distal CMAP amplitude was also calculated. An amplitude drop of more than 20% with a negative peak duration increased by less than 15% was considered to be sufficient to define conduction block[14]. F response latencies were measured as the minimal latency in a series of 3 to 10 responses (owing to the level of cooperation of the patients). The results and particularly an absent F response was not considered when the amplitude of the M response was less than 20% of the lower limit of normal. Conduction study results from individual nerves were expressed as percentage of standard values for each nerve and each age, including conduction velocities and amplitude as percentages of the lower limit of normal (mean-2SD), distal latencies and F response latencies as percentages of the upper limit of normal (mean+2SD). Age matched normal data reported by Parano and colleagues were considered as reference values[15]. Based on the results of electrodiagnostic studies, the pattern of GBS was `classified as demyelinating or axonal, using criteria adopted from Ho et al in their study of GBS patients in China[16]. Needle EMG was done in all patients for any denervation potentials and motor unit action potentials changes in Tibialis anterior and Extensor digitorum muscles. Major treatment modalities including IVIG, ventilation, and cardiovascular support were considered for all patients. Plasmapheresis was used in 1 patient who was resistant to IVIG and steroid treatment. Pulse of methyl prednisolone was also used for resistant patients with the dose of 20 mg/kg/day for 5 days. Physiotherapy was performed after the plateau stage and convalescence. Data were processed using the SPSS statistical package (version 11.05). Data were analyzed by the X2 or Fisher's exact test if frequencies were small, or McNemar's test for paired data. Continuous variables were analyzed using Student's test or ANOVA, with P<0.05 considered significant. All patients gave their written consent for participation in the study. The study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences. Findings During the two-year study period, 23 patients (13 males, 10 females) were diagnosed as GBS. Mean age of the patients was 7.5±1.85 years (range 1 year to 15 years). Of 23 patients evaluated, 5 (21%) patients required assisted ventilation for an average of 6 days (G5). 15 patents (65%) were graded as G4. The mean hospitalization was 12 days. No deaths occurred. The first electrophysiologic evaluation was performed 4 days after the admission in most of the patients. One patient experienced recurrence 6 months later, needed respirator again and got better with intravenous immunoglobulin (IVIG) and plasmapheresis. Of 15 patients who were followed for 9 months after their admission, 2 had the chronic form of GBS and steppage gait. However, this did not impediment them from doing their daily chores. They were administered 0.5 mg/kg prednisolone for 1 to 2 months. Most of our patients had the severe degrees of the disease (G4 and G5) which is because our center is a tertiary and referral center with equipped ICU which generally admits extremely sick patients. The most common findings in the first examination included: decreased CMAP (22 patients in common peroneal nerve and 19 patients in median nerve), increased DL (17 patients in common peroneal nerve and 9 patients in median nerve), increased latency of F wave (or lack of F wave) in 16 patients, and decreased NCV (14 patients in common peroneal nerve and 2 patients in median nerve) (Table 1). After one month, the results were: decreased CMAP (22 patients in common peroneal nerve and 15 patients in median nerve), increased DL (13 patients in common peroneal nerve and 8 patients in median nerve), increased latency of F wave (or lack of F wave) in 15 patients, and decreased NCV (14 patients in common peroneal nerve and 2 patients in median nerve) (Table 2). The interesting finding was that the sensory conduction was normal in sural nerve in 78% of the patients and increased to 83% after 1 month. No significant differences were found between the electrodiagnostic findings of the first evaluation and the second one. The symptoms of denervation were evident in 30% of the patients in the first and second evaluations (7 of 23 patients). However, there was no significant relation between denervation and severity of the disease. But, in 7 patients with denervation signs in EMG, the period of the disease was longer than the patients without denervation. In 16 patients without denervation signs, clinical findings improved averagely 2 months after initiation of the disease (range, 2 weeks to 3 months), but in denervated patients, the mean was 7 months. In 2 patients with chronic GBS and 1 case of recurrence, the evaluations showed denervation of the muscles. Discussion The studies performed on electrophysiologic findings in children with GBS are few[4-10]. Such studies have been performed so many times in adults and it was thought that the results were the same in children. In 2 different studies by Bradshaw and Delanoe, the electrodiagnostic findings are more or less the same as ours[4,5]. However, in some studies on GBS, the electrophysiologic findings due to demyelinization (including decreased CMAP, increased DL, increased latency of F wave, and decreased NCV) were less common[12,17]. Jafarzade-Esfahani and co-workers studied 83 patients with GBS in Iran. They reported that 72% of patients showed demyelinating sign in their NCV studies[11]. In Barzegar study in Azerbaijan province on 112 children with GBS, he found demyelinating type of GBS in about 60% of the patents[10]. In other studies, the incidence of demyelinating type of GBS was 69% in Japan[19], 70% in Argentina[20], 65% in Turkey[21], 69% in Pakistan[22], 35% in China[23], and 90% in North America[24]. The percentage of cases with the demyelinating type in our study (69%) was lower than in western countries and higher than that of Chinese population. It is however consistent with figures of the demyelinating type of GBS, observed in the neighboring countries and the Latin American regions. These findings suggest that the incidence of the demyelinating type of GBS varies considerably among countries. It may be due to different genetic background and environmental exposures. The average duration of hospital stay in our patients was 12 days, comparable to that previously reported and relevant to pathologic type of GBS[11,25,26]. The percentage of our patients requiring ventilatory assistance was 21% which was comparable to those between 21% to 43.1% reported in literature[3,27,28]. In Barzegar study, it was 10.7% and in Jafarzade Esfahani study it was 10.8%[10,11]. Our center is a tertiary and referral center with equipped ICU which generally admits extremely sick patients and this may be the reason for higher percentage of our patients requiring ventilatory assistance. The most interesting finding of our study was the normal sensory nerve conduction in sural nerve in 78% of the patients. This rate was measured to be 30% in Bradshaw’s study and exactly 78% in the study by Delanoe[7,12]. However, it has been suggested in the mentioned study that the changes in sensory nerve conduction is more prevalent in median nerve in comparison with the sural nerve. This study showed that reduction in sensory conduction velocity was delayed to week 5, but at this stage most of the children had achieved almost complete clinical recovery. So sensory conduction velocity is not a good indicator of early stage of GBS and can't help to early diagnosis of GBS. The other interesting finding was insignificant changes in electrophysiologic findings of the patients after 1 month. The primary aim of this study was to define the electrodiagnostic criteria for a very early diagnosis of GBS in children, at stage when clinical diagnosis may be difficult. A consensus for early diagnosis of GBS has not been established. Albers and colleagues proposed that the diagnosis of acute demyelinating polyneuropathy be based on one classic criterion for primary demyelination in only two nerves during the first 2 weeks of illness[29]. Meulstee and collaborators also proposed only one criterion for primary demyelination in at least two nerves but, in addition, included criteria for polyneuropathy with 11 variables including typical signs of axonal neuropathy[30]. For these authors, three abnormal variables must be observed in at least two nerves for the diagnosis of polyneuropathy. We suggest that during the first week of an acute illness in a child without any other previous neurological deficit, if three nerves show signs of demyelination with at least four abnormal variables are highly suggestive of acute demyelinating polyneuropathy. These abnormal variables include: reduction in motor conduction velocity, conduction block, prolonged distal latency, absent F wave or prolonged minimum F wave latencies, reduction in sensory nerve conduction velocity, diminution of CMAP and/or SNAP amplitudes. We concluded that from the first days of the disease, the electrodiagnostic results are helpful in the diagnosis of the disease which is in accordance with the findings of the study by Delanoe and others[5,29,31]. In previous studies, 2 findings were related to the poor prognosis of the disease; fibrillation potentials and CMAP[14,32-34]. The above mentioned studies had evaluated all age groups. In another study, neither of these factors was considered to be important in the prognosis of the patients[4]. In our study, such a relation did not exist between CMAP and process of the disease but fibrillation potentials in EMG showing axonal injury resulted in prolonged process of improvement and recurrence in 1 case. Barzegar and Arami in two separate studies in Azerbaijan province (in Iran) showed that axonal damage was significantly related to a worse recovery[10,35]. In Arami study, reduction of CMAP amplitude has been described as a risk factor for worse outcome and this is in contrast to our study result[35]. This may be due to different age group of patients in their study (range 6 years to 79 years) and ours. Our study provides an initial basis for further electrophysiological studies in pediatric GBS. A rigid, uniform protocol should answer questions about the importance of electrodiagnostic tests in early diagnosis of GBS, the value of serial studies, the relationship of electrodiagnostic data to clinical status and the usefulness of these data itself as a primary outcome measure. Our study has nonetheless, some limitations. This study was limited by small numbers of cases. Moreover, we do tests in only few nerves. Further multi-institutional studies on more children suffering from GBS are needed. We recommend to examine more nerves (including motor and sensory nerves) in four limbs. Conclusion The process of GBS and its complications are more benign in children. Electrodiagnostic evaluations are helpful at the primary stages of GBS for diagnosis. Fibrillation potentials and positive sharp waves showing denervation and axonal injury are presentative of longer duration of the disease. Denervation potentials was not significantly related to the severity of the disease, but has resulted into recurrence and prolonged sickness. This study showed that low mean CMAP which predict a poor outcome in adult GBS, may not apply to childhood GBS. Acknowledgment The study was approved and funded by the Research Committee of Shahid Beheshti University of Medical Sciences. We would like to thank Dr M Ghofrani, Dr B Jafroudi, Dr E Azargashb, and Mrs S Aghamohammadi for their precious help in this study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences,All rights reserved. The following images related to this document are available:Photo images[pe09008t2.jpg] [pe09008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}