 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
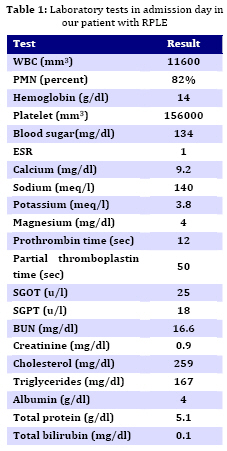
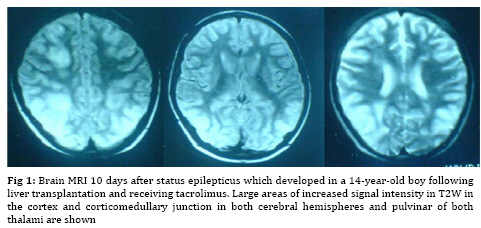
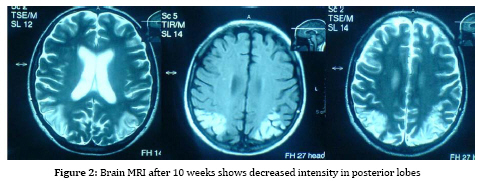
Iranian Journal of Pediatrics, Vol. 19, No. 1, March, 2009, pp. 69-74 Status Epilepticus as a Presenting Sign of Reversible Posterior Leukoencephalopathy Syndrome in a Liver Transplant Recipient Mohammad-Mehdi Taghdiri1, MD; Ali Amanati, MD1; Seyed-Mohammadali Musavi MD1 1. Department of Pediatrics, Hamadan University of Medical Sciences, Hamadan, IR Iran Received: 26/12/07; Revised: 12/08/08; Accepted: 15/11/08 Code Number: pe09011Abstract Background: Reversible posterior leukoencephalopathy syndrome (RPLE) is an increasingly recognized disorder, most commonly associated with immunosuppressive and cytotoxic agent, malignant hypertension and toxemia of pregnancy. Neurological symptoms are headache, mental and visual disturbance, and seizures. Brain MRI findings are symmetrical bilateral hyper intense areas of occipital and parietal lobes in T2–weighted magnetic resonance (MR) images. This finding is reversible with prompt successful treatment which may take days to weeks for full reversal. Key Words: Reversible posterior leukoencephalopathy; Status epilepticus; Immunosuppressive; Liver transplantation; Tacrolimus Introduction Neurological complications of liver transplantation occur in 20% to 60% of patients. Almost one half of them manifest by seizures and other half with tremor, headache, distonic reaction, detached retina, transient enuresis and fatigue[1,2,3]. Etiologically they can be categorized into problems related to the underlying disease, problems related to the transplant procedure, side effect of immuno-suppressive drugs and neurological complications arising from immuno-suppression[4]. Seizures are predominantly associated with opportunistic infections or neurotoxic effects of immunosuppressant drugs. Reversible posterior leukoencephalopathy syndrome (RPLE) is one of these effects on central nervous system (CNS). Drugs which can develop RPLE are: cyclosporine-A, tacrolimus (FK506), interferon-(IFN-), cisplantin, cytarabine, intra venous immune globulin (IVIG) and erythropoietin. Conditions which can develop RPLE are hypertensive encephalopathy, eclampsia, drug with-drawal (clonidin)and acute glomerolo-nephritis[4,5]. The pathogenesis of RPLE is not overwhelm of normal auto regulatory mechanisms, leakage of cerebral arterioles and toxic damage of blood brain barrier or vascular endothelium [4,5,6]. Only a few cases of RPLE syndrome with status epilepticus have since been reported in literature. We report a case of possibly RPLE with status epilepticus to the best of our knowledge. Case Presentation The patient was a 14-year-old boy admitted for recurrent tonic clonic generalized seizures with duration of 1-3 minutes who did not recover consciousness between the post-ictal periods, lasting more than 30 minutes. He had no other symptoms except headache experienced 8 hours before seizures. A history of seizures either before or post transplantation was absent. The patient had been known as cryptogenic cirrhosis since he was 7 years old. He had splenomegally and a history of recurrent bleeding of esophageal varicosis. He had successfully undergone liver transplantation 32 days before admission. He had been discharged 12 days after liver transplantation on tacrolimus, prednisolone, aspirin, amlodipine, co-trimoxazole and fluconazole. He had not shown any symptoms since admission. Physical examination revealed an unconscious patient responding to painful stimuli with a pulse rate of 90/min, blood pressure 120/80 and axillary temperature of 37. No meningeal signs or focal neurological deficit on CNS examination was present. There was no papilledema on fundoscopy. Cerebro-spinal fluid (CSF) analysis was in normal limits and CSF culture and polymerase chain reaction (PCR) for herpes virus were negative. Table 1 shows laboratory tests at admission. Brain magnetic resonance images (MRI) after 48 hours showed high signal lesions in biparietal and right frontal white matter. Brain MRI after 10 days revealed large areas of increased signal intensity in T2–weighted magnetic resonance imagesin the cortex and corticomedullary junction in both cerebral hemispheres and pulvinar of both thalami (Fig. 1). Occipital lobes and cerebellar hemispheres were also involved. Brain MRI after 10 weeks showed symmetrical large hypersignal area of occipital lobes (Fig. 2). In T2–weighted MRI, cortex and superficial white matter of both occipital lobes with extension to the posterior aspect of parietal lobes were involved. Immediately after admission, prompt assessment was performed and treatment begun without delay. To stop proloned seizures we administered diazepam, phenytoin and Phenobarbital and displaced tacrolimus by cycolsporine. Seizures recurred after one hour, but with lower frequency. Therefore we continued infusion of midazolam, the patient was resistant to this treatment. After adding sodium valproat to regimen the seizures stopped and several minutes thereof patient obtained full consciousness and completely recovered. He received parenteral anticonvulsant therapy for the next 48 hours succeeded by oral therapy. The patient was discharged with sodium valproate, prednisolone, cyclosporine, anti-biotics and amlodipine after six days. On follow up 10 weeks later he was asymptomatic. Discussion The seizures following liver transplantation can arise from many etiologies. They are categorized as follows: (A) Problem related to the underlying disease: lingering effect of hepatic failure due to preexisting hepatic encephalopathy[3,7]; (B) Problems related to the transplant procedure: initial encephalopathy, major fluid and electrolyte shifts, raised intracranial pressure, side effect of drugs[4], vascular accident and air embolus[8]; (C) Complications of immu-nosuppressive drugs and cytotoxic agents: cyclosporine, tacrolimus[4], azathioprine, mycophenolat, cisplantin, cytarabin, INF-, IVIG and erythropoietin [5]; (D) Compli-cations arising from immunosuppression: infection[4, 9], side effect of drugs used for treatment of infections (imipenem, fuscarnet) [4], and post transplant liver disease (PTLD)[10, 11]. The first two categories do not applicable to this patient because of their presentation in a few days after surgery. In addition, the patient had no history of encephalopathy or seizures before liver transplantation, there was no metabolic abnormality and no evidence of raised ICP or focal neurological signs. In most patients seizures are associated with toxic levels of immunosuppressive drug or with opportunistic infections[3,4,12]. Acute CNS infectious are less probable in our patient because of normal CSF analysis (WBC=0, RBC=0, protein and glucose in normal limits), CSF culture and CSF PCR were negative. On the other hand, CNS infections usually occur 1-6 months post liver transplantation (Timetables for CNS infections are provided)[8, 12]. In addition, sudden onset of seizures without fever in an asymptomatic patient and rapid recovery are in contrast with CNS infection. Other causes of acute encephalopathy such as acute disseminated encephalomyelitis (ADEM) did not explain the course of the disease. ADEM is a monophasic syndrome characterized by the rapid onset of neurologic signs and symptoms after viral or bacterial infections or vaccinations, with a triad of focal neurologic deficit, ataxia and alteration in mental state. Our patient had no risk factors for ADEM and no focal neurologic signs or movement disorder and ataxia. He had normal deep tendon reflexes (DTR) which should be exaggerated in ADEM[13,14]. RPLE is the first line diagnosis for our patient. RPLE was diagnosed in patients who fulfilled all the following criteria: (1) neurological symptoms and signs, such as seizure, extremity weakness or mental change; (2) risk factors for RPLE, such as treatment with cyclosporine, eclampsia, and history of hypertension (acute sustained rise in diastolic pressure more than 100 mmHg); (3) absence of other possible causes of encephalopathy; (4) reversible course, that is, signal changes of acute encephalopathy found during symptom manifestation were no longer observed on follow-up MRI, or clinical symptoms and signs resolved completely after treatment[15]. RPLE occurs in some patients receiving tacrolimus. Both mild and major neurological adverse effects have been reported in patients receiving this drug.Mild neurological symptoms including headache, paresthesia, tremor, sleep disturbances, photophobia, and dysesthesia have been reported in 40% to 60% of patients, and major neurological complications such as confusion, seizures, cortical blindness, encephalopathy, and coma, occur in 5% to 8% of patients receiving the drug[16]. The term RPLE emphasizes its location and relatively reversible nature. This complication is more common when high doses are used, but there is no specific blood level that separates affected and unaffected patients receiving the drug[4, 16]. The onset of RPLE is acute to sub acute and most patients have minor symptoms just hours before the seizures[5, 9]. One study reports that most seizures are single episode and easily controlled[7]. CSF in RPLE is usually normal or may have mild elevation in protein[4,5,10]. Imaging changes are hyperintensity on T2–weighted or hypointensity on T1–weighted MRI, which is seen in bilateral occipital and parietal lobes and rarely may involve frontal lobes, brain stem, midbrain, pons, medulla oblongata, cerebellum and basal ganglia[3,5,16]. Calcarine /paramedian occipital lobes are spared [5,6]. Imaging findings are reversible with prompt successful treatment (which may take several days to weeks for full reversal), and if treatment is not promptly initiated, may progress to infarction or hemorrhage[16]. In retrospective view, this patient was asymptomatic before seizures and on clinical examinations he had no focal neurological deficit, hypertension or metabolic abnormalities. Fever, meningeal signs or prodromal symptoms of infectious disease were absent and seizures occurred 32 days after liver transplantation. These findings suggest less probability of infections or other causes as an etiology. On the other hand, history of tacrolimus therapy and typical images on MRI and rapid recovery of clinical symptoms and rapid obtainment of full consciousness after a few hours, suggest RPLE as a more probable cause of seizures. The significant findings of this patient were widespread involvement of the brain on MRI and difficult response to treatment with benzodiazepins, phenobarbitals and phenytoin, and finally good response to Na- valproate. According to criteria discussed earlier our patient fulfilled these criteria and so the management based on RPLE. To treat RPLE blood pressure should be controlled if increased, offending agent (immunosuppressant, cytotoxic) discontinued or decreased in dosis if administered, hypomagnesaemia if present (usually associated with cyclosporin) treated, and seizures treated with anticonvulsants as well. Note that most of anticonvulsants interfere with the metabolism of immunosuppressive agents thus increasing their dosage[4]. Benzodiazepins, gabapentin and valproate are the drugs of choice[17]. The differential diagnoses of RPLE are vascular accident (infarction, hemorrhage and venous thrombosis), infections (encephalitis, meningitis) or an inflam-matory/autoimmune process (post infectious encephalomyelitis or vasculitis)[5,16]. Regarding prognosis, most patients recover completely with prompt treatment within hours (12-24 h) to days; imaging findings may persist for weeks[5]. Reversible posterior leukoencephalopathy syndrome as side effect of tacrolimus is very rare (only 31 cases of immunosuppression-associated leukoencephalopathy in liver transplant recipients reported in the literature are related to tacrolimus therapy until 2003)[18]. In 58% of published cases immunosuppression associated leukoen-cephalopathy occurred within 30 days after transplantation. Liver transplant recipients seem to develop these lesions earlier than other organ transplant recipients, with a mean time of onset of 9 days after transplantation[18]. Conclusion During the early post transplantation period any neurological disturbance, even a minor one, should alert the clinician as it might be a warning sign of a coming seizure and it may be RPLE syndrome. References
The following images related to this document are available:Photo images[pe09011f2.jpg] [pe09011f1.jpg] [pe09011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}