 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
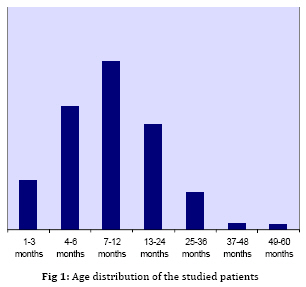
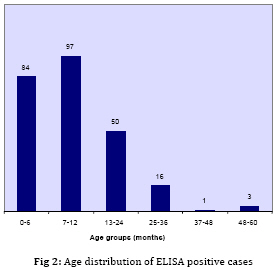
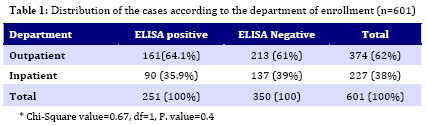
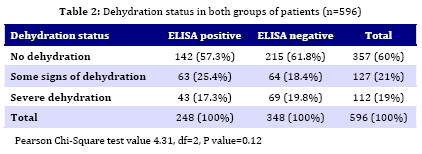
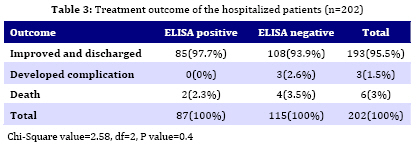
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 107-116 Severity of Rotavirus Diarrhea in Children: One Year Experience in a Children Hospital of Bangladesh Selim Ahmed1, MBBS, FCPS, MPH; ARM Luthful Kabir1, MBBS, FCPS; Aminur Rahman2, MBBS, DCM, MMed; Maleeha Hussain3, MBBS, M Phil; Soofia Khatoon1, MBBS, FCPS, MHPed; Abdul Hannan1, MBBS, FCPS 1. Department of Pediatrics, Institute of Child and Mother Health, Matuail, Dhaka, Bangladesh Received: Sep 03, 2008; Final Revision: Jan 02, 2009; Accepted: Feb 05, 2009 Code Number: pe09017 Abstract Objective:This study was conducted to determine the hospital prevalence, clinical severity and treatment outcome of rotavirus versus non-rotavirus diarrhea in children attending a secondary level children hospital of Bangladesh. Key Words: Rotavirus; Diarrhea; ELISA; Gastroenteritis Introduction Rotavirus is the leading cause of diarrhea hospitalization among children worldwide[1]. In 2000-03, six causes accounted for 73% of the 10.6 million yearly deaths in children younger than age 5 years; of which diarrhea was responsible for 18% of total deaths[2]. As of 31 March 2006, the World Health Organization estimated that globally 527,000 (475,000-580,000) child deaths occurred during 2004 due to rotavirus infection[3]. National estimates of rotavirus attributable deaths among children under five years of age ranged from 122,270 (India) to fewer than 5 deaths (58 countries). Twenty-three percent of all rotavirus deaths under five years of age occurred in India. Six countries (India, Nigeria, the Democratic Republic of the Congo, Ethiopia, China and Pakistan) accounted for more than half of all Rota deaths under age five in 2004[3]. Several different groups of viruses have been shown to be responsible for high incidence of acute viral gastroenteritis among children during their first few years of life. Four major categories of viruses are now recognized as clinically important including rotavirus, astrovirus, adenovirus and calcivirus[4]. Rotavirus is the single most important etiological agent causing severe dehydrating diarrhea across the globe. Each year, rotavirus causes approximately 114 million episodes of gastroenteritis requiring only home care, 25 million clinic visits, 2.4 million hospitalizations and 610,000 deaths in children under five years of age. This means that by the age of 5 years, almost all children will experience an episode of rotavirus gastroenteritis, 1 in 5 will require a clinic visit, 1 in 50 children will require hospitalization, and approximately 1 in 250 will die from rotavirus disease [5]. A 10-year hospital-based survey of rotavirus diarrhea conducted in Hong Kong linked rotavirus to 26% of all diarrhea-related admissions and 6% of all admissions in children under 5 years of age. Based on this, the annual cost of rotavirus attributed admissions to the hospital for children less than 5 years old was estimated to a national cost equivalent to ~ US$ 1.2 million per year[6]. After pneumonia, diarrhea is the second commonest cause of infection-related death in under five children of Bangladesh. During the year 2001-2004, between 5756 and 13,430 children died from severe rotavirus gastroenteritis each year[7]. While overall deaths from diarrhea are declining in Bangladeshi children, the proportion of diarrhea deaths due to rotavirus have actually increased and this pathogen now alone accounts for about 40% of all diarrhea deaths [7]. Detection of the rotavirus in diarrhea is necessary in assessing the clinical severity as well as providing an estimate of rotavirus diarrhea within a community. This is particularly contextual in Bangladesh, where diarrhea is still contributing a significant proportion of mortality and morbidity in under five children and where rotavirus diarrhea is claimed to be on the rise[7]. Till date,International Centre for Diarrheal Disease Research, Bangladesh (ICDDR,B) has conducted many studies on various strains of E. Coli diarrhea, Shigellosis, Entamoeba and others in children diarrhea [8, 9, 10, 11], few data are available on the prevalence and characteristics of rotavirus diarrhea in communities encompassing urban, peri-urban and rural population. Every year, there are some seasonal peaks of diarrhea in Bangladesh and ICDDR,B alone has to treat more than 100,000 patients a year[10]. The data on clinical characteristics and treatment outcome of rotavirus diarrhea are likely to be helpful for the medical professionals and health care providers working at the grass root levels who have the tendency to refer any acute watery diarrhea with or without vomiting to ICDDR,B or to other secondary/tertiary level hospital for “better management”. This study was intended to explore the clinical severity, nature of disease and to observe the treatment outcome of both Rota and non-rotavirus diarrhea in children of Bangladesh, and to see the justification of such a huge referral of diarrhea cases to higher centers. Subjects and Methods This cross sectional study was carried out in the Institute of Child and Mother Health (ICMH) between July 2005 and June 2006. ICMH is a secondary level children hospital, located at the outskirts of the capital city at a peri-urban location. Majority of the children attending this hospital belong to low to middle income families residing in the peripheral regions of the capital city and adjacent districts. Since this institute is the only secondary level health care centre in this area, majority of the children of the vulnerable section of the population suffering from diarrhea and other illnesses are likely to attend to this hospital. This gave a unique opportunity to identify rotavirus in the diarrhea of children in these communities. Children in the age group of 1 months to 5 years suffering from acute watery diarrhea and whose parents gave consent to participate in the study were enrolled. Diarrhea was defined according to WHO i.e. three or more loose stools in 24 hours. Diarrhea patients attending the outpatient department (OPD) or admitted in hospital (inpatient department or IPD) were included. Treatment in IPD or OPD was determined by the state of dehydration, vomiting, and presence or absence of other systemic illness. Information of socio-demographic condition, water and sanitation, personal hygiene, food habits, diarrhea related symptoms and physical signs were recorded in a pre-tested questionnaire. The dehydration status was assessed and classified according to WHO guideline which is followed in the Integrated Management of Childhood Illness (IMCI) training. The classifications were “no signs of dehydration”, “some signs of dehydration” and “severe dehydration” equivalent respectively to “mild”, “moderate” and “severe” dehydration in clinical practice. Stool specimen collection: Two samples of stool were collected from each patient. The analyzable samples were collected in containers containing 10% phosphate-buffer-solution. The other samples, designated as master samples, were kept standby in need of further advanced analysis. The samples were preserved at – 80 degree C until use. Sample analysis: From the pool of analyzable specimen, rotavirus antigen was detected once in a week using commercial ELISA kits (Rotaclone, Meridian Diagnostics, Inc., Cincinnati, Ohio, USA). According to the manufacturer’s documents supplied with the commercial kits, it is considered to have a 100% relative sensitivity, 97.2% relative specificity and a 97.7% relative agreement. The manufacturer’s instructions were followed during ELISA tests. Analyzed samples were marked as ELISA positive and ELISA negative. Follow up: The hospitalized patients were followed up till last days in hospital. The patients enrolled from OPD were followed up either by ensuring repeated follow up visits to hospital (patients living nearby) or by telephone call. Information about vomiting, purging, fever, thirst and physical activities were obtained and recorded as follow up tools. End of diarrhea was considered when stool consistency became “normal” according to the parents perception. Statistical analysis: Data were entered and analysed using statistical SPSS (ver 15.0). Chi square and Student’s t tests were performed to determine the significance of difference observed between two different groups of patients. In cases where the expected value for a cell was <5, Fisher’s exact test was used. For nonparametric data, comparison between two groups was assessed by a Mann-Whiteny U test. P values <0.05 were considered statistically significant. Ethical issues: The research proposal was ethically cleared by the Ethical Review Board of ICMH. A verbal consent was taken from either parent of the enrolled child prior to interview and collection of stool samples. Findings Throughout the study period, we enrolled 656 patients of which 55 (11.92%) were dropped out because of missing in follow up. All the dropped out cases were recruited from OPD and were assigned home treatment. Broad classification of the cases after ELISA tests: Among 601 stool samples tested for rotavirus antigen, 42% were ELISA test positive and 58% were ELISA negative. Accordingly, cases were designated as “ELISA positive “and “ELISA negative” for the purpose of description. Age: The mean age (±SD) of the studied patients was 12 ±9.9 months; the median being 9 months. For convenience of analysis, patients were categorized into 4 inhomogeneous groups (Fig 1). Around 90% patients in both groups suffered from diarrheal disorder within first two years of life. In ELISA positive group, second half of infancy had the peak of Rota viral diarrhea (Fig 2). Sex: Overall male predominance was observed in both ELISA positive and ELISA negative groups. The M: F ratio in ELISA positive group was 1.3: 1 and that of ELISA negative group was 1.5:1. Although male children were seen to suffer more from diarrhea, this difference in sex was not statistically significant (P=0.5). Department of patient enrollment: Of 601 finally enrolled cases, 62% cases were enrolled from OPD and 38% from IPD. Among the ELISA positive samples, the OPD/IPD distribution was 64% and 36% respectively (Table 1). Diarrhea-related selective clinical symptoms and their severity: Fever: Fever was present in 58.4% of ELISA positive and 51.9% of ELISA negative cases. The grade of the fever was categorized as “mild” (37.7-38.5 °C), “moderate” (38.6-39.5 °C) and “severe” (>39.6 °C) according to the narration of the parents and temperature record of the OPD and hospitalized patients. In about half of each group (49.7% in ELISA positive and 50.3% in ELISA negative group), fever was mild. Vomiting: In 383 (63.7%) patients, there was history of vomiting. The vomiting was either preceded or followed by diarrhea. Unprovoked and spontaneous vomiting was significantly higher in ELISA positive cases (P=0.001). In 40.7% cases of ELISA positive and 40.8% of ELISA negative cases, vomiting stopped within 48 hours of onset. Frequency of purging: Over half (55.6%) of ELISA positive cases, there were 6-10 motions per day. This figure was significantly higher (P=0.04) in comparison to ELISA negative cases. Dehydration: In 57.3% of ELISA positive and 61.8% cases of ELISA negative patients, there was no sign of dehydration (which is equivalent to mild dehydration in clinical practice). Some signs of dehydration (clinically moderate dehydration) were observed in 25.4% ELISA positive and 18.4% of ELISA negative group. In less than one fifth cases in both groups, dehydration was severe requiring hospitalization and intravenous fluid (Table 2). So far dehydration status was concerned; there was no statistically significant difference in the grade of dehydration between two groups (P=0.12). Duration of diarrhea: The mean duration of diarrhea was 4.6 (±5.3) days in all cases; the median being 3 days. The difference of duration of diarrhea between two groups was insignificant (P=0.7). Duration of hospital stay: The mean duration (±SD) of hospital stay of the admitted patients was 4.7 (±4.3) days. It also showed no significant difference between the two groups (P=0.8). Treatment outcome of the admitted patients: Almost all cases (97.7%) of ELISA positive diarrhea recovered uneventfully without any complication. This figure for ELISA negative diarrhea was 93.9% (Table 3). The difference was insignificant (P=0.3). Death: There were 6 deaths in the series; 2 in ELISA positive group and 4 in ELISA negative group. All these unfortunate children had associated severe protein energy malnutrition along with diarrhea. Again this difference in death between two groups was not significant (P=0.3). Discussion Worldwide, diarrhea related mortality has decreased, mainly because of better therapeutic interventions along with provision of safe drinking water, improvement of sanitation and popularization of primary health care activities [12,13]. Many studies across the world have shown the important role of rotavirus as a cause of diarrhea in children both in developed and developing countries[14-21]. We conducted this study to estimate the diarrheal disease burden due to rotavirus infection amongst under five years-old children with diarrhea in Bangladesh. Our study showed a rotavirus prevalence of 42% in children with diarrhea attending the Institute of Child and Mother Health. Similar results on rotavirus prevalence were obtained from other studies in home [22, 23] and abroad [24, 25]. In our study, 92% of rotaviral diarrheas were identified in the age group of less than 2 years. This result is comparable to the findings of other studies [15, 20]. In our study, the highest (38.6%) prevalence was seen in children from 7-12 months of age. The same picture of age predisposition was observed in some studies from Bangladesh [23, 26] and in other places [19,20] but is different from other study where rotavirus diarrhea has been demonstrated mainly in children under six months old[27]. The highest prevalence during the second half of infancy can be explained by the declining immunity incurred through breast feeding [29] and starting “oral phase” of the normal developmental milestones in children when babies put almost everything into mouth. The male preponderance (60%) in rotavirus diarrhea obtained in our study is also quiet similar in other studies [21, 30,31, 32]. The explanation to this male predominance remains unclear, and this difference bears no statistical significance. Majority of rotaviral diarrhea cases attended and treated at OPD. A similar scenario was also noticed in an Indian study [33]. This indicates that majority of the rotavirus diarrhea were not clinically severe enough to be hospitalized. Like our study, significant association of nausea and vomiting with rotavirus diarrhea is also evident in some other studies [21, 34,35]. In our study, majority of both Rota and non-Rotavirus diarrhea patients had either mild or moderate dehydration. This is similar to what is seen in other study [33]. In only one-sixth of cases, the dehydration was severe requiring hospitalization for intravenous fluid of which majority recovered uneventfully. Total 6 patients died; 2 (2.3%) in ELISA positive and 4 (3.5%) in ELISA negative groups. All these unfortunate children had severe malnutrition along with diarrhea. There was no statistically significant difference in the treatment outcome of both groups. Despite maximum effort, we failed to enroll all diarrhea patients attending the hospital during the study period. Unwillingness of the parents not to participate not motivated to spend a bit longer time in hospital and hospital holidays were the main causes for this failure. Conclusion As the pioneer country of discovering Oral Rehydration Solution (ORS) by ICDDR,B, the results of this study is expected to encourage the health care professionals in terms of diagnosis and treatment plan of rotavirus diarrhea in Bangladesh. Despite high prevalence, rotavirus diarrhea can successfully and confidently be managed at home and in the oral rehydration corner of small hospitals. The results of this study are expected to reduce the number of referral of diarrhea patients from rural centers to secondary/tertiary level hospitals which almost always remain over-occupied. Moreover, treatment of diarrhea at home and nearby hospital can save many working hours of the parents, who must accompany the ailing children. Acknowledgment We acknowledge the cooperation of the Ethical Review Board of IMCH and the personal contributions of AUM Mohsin, M Quamrul Hassan, SM Shanwaz-Bin-Tabib, Shafiuddin Ahmed, Tania Islam and Shahnaj Akhter in this study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09017t2.jpg] [pe09017t1.jpg] [pe09017t3.jpg] [pe09017f2.jpg] [pe09017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}