 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
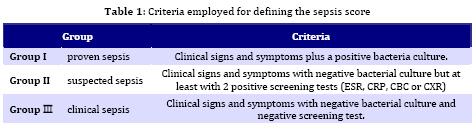
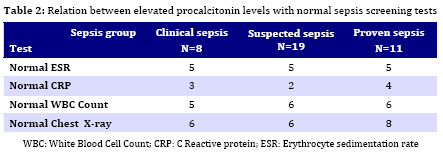
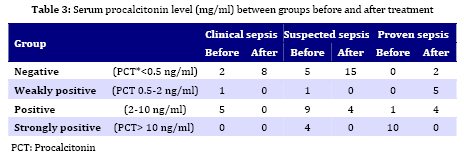
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 117-122 Procalcitonin as a Marker of Neonatal Sepsis Yadolla Zahedpasha*1,2, MD; Mousa Ahmadpour-Kacho1, MD; Mohmoud Hajiahmadi3, PhD; Mohsen Haghshenas1,2, MD 1. Department of Pediatrics, Babol University of Medical Sciences, Babol, IR Iran Received: Sep 01, 2008; Final Revision: Dec 15, 2008; Accepted: Jan 14, 2009 Code Number: pe09018 Abstract Objective: Early diagnosis of neonatal sepsis and appropriate treatment decreases the mortality and morbidity of these infants. The aim of this study was to assess the role of procalcitonin (PCT) as a marker in the early diagnosis, treatment and follow-up of neonatal sepsis. Key Words: Neonatal sepsis; Procalcitonin; Marker; Infection; Infancy Introduction Neonatal sepsis is one of the major health problems throughout the world; every year an estimated 30 million newborns acquire infection and 1-2 millions of them die[1]. Since the clinical signs and symptoms of sepsis in neonates are non-specific and associated with high (28-50%) morbidity and mortality, early suspicion and treatment before blood culture confirmation of it is crucial[2]. An inflammatory marker such as C-reactive protein (CRP) does not reliably differentiate between the systemic inflammatory response and sepsis[2,3]. Procalcitonin (PCT), a precursor of calcitonin is a 116 amino acid protein secreted by the C cells of thyroid gland in normal situation but its levels may increase during septicemia, meningitis, pneumonia and urinary tract infection[3,4]. This marker also is produced by macrophage, and monocyte cells of various organs in severe bacterial infection and sepsis[5,6]. The results of recent studies suggest the usefulness of PCT for early diagnosis of neonatal sepsis [7-19], although other investigations have observed lack of accuracy for this marker [20, 21, 22]. Since a kit for quantization of PTC is available for rapid quantitative measurement, we carried out this study to evaluate the serum level of PTC on neonatal sepsis in relation to our classification of neonatal sepsis. Subjects and Methods This prospective study was conducted on neonates admitted for sepsis work up to newborn service and neonatal intensive care unit (NICU) at Amirkola Children's Hospital in Babol, North of Iran. This department provides health service for more than one million people living in the west of the province Mazandaran. Sepsis work up including complete blood count (CBC), blood culture, erythrocyte sedimentation rate (ESR), CRP, urine analysis (UA), urine culture (UC), chest X-ray, cerebro spinal fluid (CSF) analysis and culture was performed in all neonates. Three distinct groups were defined; proven sepsis, suspected sepsis and clinical sepsis (Table 1). Exclusion criteria were administration of antibiotic therapy prior to admission, birth asphyxia, aspiration syndromes, laboratory finding suggestive of inborn error of metabolism and congenital anomalies. The sample size was calculated 30 neonates when considering confidence interval 95% power 80% and error in serum PCT estimation of 0.1 nanogram. Before starting the antimicrobial therapy, blood samples (sample 1) for complete blood count, CRP, ESR, PCT and culture were collected. This procedure was repeated at day 5 after treatment with antibiotics (sample 2). CSF, urine, tracheal and gastric aspirate cultures were obtained. Serum PCT level was measured using quantization immuno-luminometry method by lumitest kit (Brahms Diagnostic, Berlin, Germany). In this assay a PCT level of ≥0.5 ng/ml was accepted as pathological. PTC level 0.5-2 ng/ml, 2-10 ng/ml and >10 ng/ml considered as weakly positive, positive, and strongly positive, respectively. The study protocol was approved by the ethical committee of Babol University of Medical Sciences. Informed parental consent was obtained for all infants. We used SPSS version 15 for statistical analysis. Correlation between variables and statistical differences were analyzed using Fisher exact, ANOVA, Monte Carlo and Wilcoxon tests. P values of <0.05 were considered to be significant. Findings Thirty-eight neonates were eligible for the study. These neonates are classified into three groups; proven sepsis (11 neonates), suspected sepsis (19 neonates) and clinical sepsis (8 neonates) according to the study protocol. The mean gestational age, birth weight and the sex of the patients in these three groups were similar (P-value 0.096). Early onset sepsis was confirmed in 25 (65.8%), late onset sepsis in 9 (23.7%) and nosocomial sepsis in 4 (10.5%) patients. Causative pathogens and site of involvement were as follows: CSF in one patient positive for Escherichia coli, blood culture in nine patients positive for Staphylococcus, Escherichia coli and Klebsiella; urine in two neonates for Staphylococcus and Escherichia coli; and culture of the tip of chest tube was positive for Pseudomonas. Table 2 shows the results of sepsis screening tests including PCT in relation to three classified groups of patients. It neonates with proven sepsis in spite of negative result for sepsis screening test, the result of PCT was positive. This result was seen also in some patients with clinical sepsis. Table 3 shows the serum concentrations of PCT in the studied groups. Comparison of serum PCT level before and after treatment reveals significant changes in clinical sepsis (P=0.001) and proven sepsis (P=0.003) groups of patients. Discussion In the present study the PCT levels were remarkable high in neonates with proven sepsis and the levels dropped dramatically after treatment with antibiotics. Also in some cases of proven and suspected sepsis the levels of PCT were high in spite of negative results for other sepsis screening tests. Previous studies had shown high PCT levels in all neonates with proven or clinically diagnosed various types of neonatal sepsis[8,2,22,24,25]. In a recent study Koksal et al concluded that serum procalcitonin level was superior to serum CRP level in terms of early diagnosis of neonatal sepsis, in detecting the severity of the illness and in evaluation of the response to antibiotic treatment[26]. In our study the serum PCT level was high in most of the patients before the initiation of therapy, but there was not a significant correlation between the serum PCT level and the type of sepsis. In Koksal study, unlike our study, the level of serum PCT had a significant difference between the four study groups (no sepsis, probable sepsis, highly probable sepsis and possible sepsis). This difference may be due to the small sample size of our study. The serum PCT level in our study decreased significantly in all three sepsis groups which were most evident in proven sepsis group and like the same finding reported in other studies[26, 27, 28]. Athhan et al in their study revealed that at 7th day of therapy neonates who had achieved clinical recovery had a significant decrease of procalcitonin levels compared to the initial values (P=0.000)[29]. This finding was reported also by Viallon and coworkers in 50 patients presenting with bacterial meningitis at day 2 after appropriate antibiotic treatment[30]. Carol et al in their study showed that procalcitonin is more sensitive than the CRP in the diagnosis of septicemia, meningitis and urinary tract infection [28]. In our study there were four cases of culture positive sepsis accompanied with elevated levels of procalcitonin while the CRP level was not high (Table 2). Kawezynski and Piotrowski analyzed inflammatory parameters in 48 newborn infants suffering nosocomial sepsis admitted to the intensive care. They obtained samples for PCT and CRP levels just at time of onset of the signs and 24 hours later. At the onset of gram negative sepsis 14 of 17 contaminated newborns had significantly increased PCT and CRP levels, but at the onset of gram positive sepsis only 18 from 31 neonates with positive blood culture had increased CRP level and 28 of them had elevated concentration of serum PCT. These differences were statistically significant[31]. The usefulness of PCT was assessed by Lopez Sastre and their colleagues as a marker of neonatal sepsis of nosocomial origin in neonates admitted to the 13 neonatology services of 13 acute-care teaching hospitals in Spain over one year. They concluded that serum PCT concentration showed a moderate diagnostic reliability for the detection of nosocomial sepsis from the time of infection17. Four of all culture positive neonates in our study had nosocomial sepsis and all of them had elevated PCT levels. One of the limitations of the present study was the shortage of culture positive neonatal standard for sepsis to determine the sensitivity and specifity. For this reason we classified the neonatal sepsis into three groups and assessed the PCT level in relation to the class of sepsis before and after treatment. Conclusion The PCT concentration in our study was elevated in culture positive neonates and decreased with appropriate antibiotic therapy. In some cases of culture positive babies other sepsis screening tests were negative but the level of PCT was elevated. These findings support the usefulness of the PCT to establish an early diagnosis of neonatal sepsis. Acknowledgment The authors would like to thank Dr. R. Alizadeh for his statistical assistance, Dr. E. Aalaei, Dr. A. Mirfazeli, Mrs. Mazloomi and Ms. Jahangir for their help in patients' enrollment. We also give our special thanks to Professor Roushan for his comments on editing this manuscript. Our institutional review committee of ethical research approved the study. This study was fully funded by a research grant of Babol University of Medical Sciences, Iran (Grant number 191351523). References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09018t2.jpg] [pe09018t3.jpg] [pe09018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}