 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
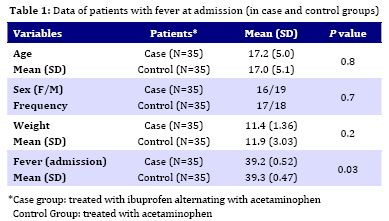
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 164-168 Alternating Ibuprofen and Acetaminophen in the Treatment of Febrile Hospitalized Children Aged 9-24 Months Nader Pashapour 1, MD;Ali A Macooei1, MD;Sariyeh Golmohammadlou2, MD 1. Department of Pediatrics, Urmia University of Medical Sciences, Urmia, IR Iran Received: Aug 12, 2008; Final Revision: Dec 13, 2008; Accepted: Jan 13, 2009 Code Number: pe09026 Abstract Objective: Recently, studies reported the emergence and increasing popularity of the alternate use of acetaminophen and ibuprofen. The aim of the present study was to compare the clinical effectiveness of acetaminophen alone with an alternative regimen of acetaminophen and ibuprofen in hospitalized infants aged 9-24 months with fever of non bacterial origin. Key Words: Acetaminophen; Ibuprofen; Antipyretic; Fever; Infant Introduction Fever is one of the most common complaint and signs of illness in office-based primary care pediatric practice, accounting for 19% to 30% of visits[1]. Although most experts consider fever a beneficial physiologic response to the infectious process, often it leads to patient irritability and stress as well as parental anxiety[2]. Acetaminophen is very widely used as an antipyretic owing to its availability and good safety[3]. Ibuprofen, like acetaminophen is an effective antipyretic and is well tolerated. There is no evidence of a difference with acetaminophen in the short term adverse effects, has good gastrointestinal tract absorption feature, reaching peak plasma concentration in one hour; the maximum temperature reduction peaks within 30 minutes[4]. In addition, studies of parental knowledge of fever exposed unfounded fears (Fever phobia) and misconception forced many parents and some physicians to inappropriate care[5]. New studies reported the emergence and increasing popularity of the alternative use of acetaminophen and ibuprofen[6,,7]. The aim of the present study was to compare the clinical effectiveness of acetaminophen alone with an alternative regimen of acetaminophen and ibuprofen in hospitalized infants aged 9-24 months with fever of non bacterial origin. Subjects and Methods This study was performed between March 2006 and December 2007, in 2 pediatric center in Urmia, which are tertiary level and affiliated to Urmia University of Medical Sciences. The study was approved by Research Center Board and the Ethics Committee of the University. Eligible cases were febrile hospitalized patients aged between 9 and 24 months, whose rectal temperature was ≥38.5oĊ. Exclusion criteria included any of the following: intolerance or major complications of the administered drug such as abdominal pain, vomiting, hypothermia, acute or chronic renal and hepatic disease, asthma, metabolic disease, bleeding disorder, convulsion, children with concurrent or previous intake of antibiotics and antipyretics, clinical or laboratory evidence of bacterial infection, and cases that did not complete the study. We chose non bacterial infection to limit scope of fever. Stool analysis, stool culture, cell blood count (CBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), chest x-ray, electrolytes, blood sugar, blood urea nitrogen and creatinine were evaluated in all cases. In this clinical trial study, patients were randomly separated into two groups. Written consent was obtained from parents. Infants of case group received 10 mg/kg ibuprofen alternating with 15 mg/kg acetaminophen every four hours. Infants of control group received 15 mg/kg acetaminophen every four hours. Temperature of patients of the two groups was taken at admission, 2, 4, 5, 7, and 8 hours after drug administration. According to sample size calculation formula, for this study twenty patients would be sufficient to detect an assumed difference of 30% between groups in the reduction of fever. Chi-square and t-test were used to compare the probability of sex, age and temperature difference between case and control groups. Findings During the study period, of the 76 cases, 7 cases were excluded because the parents did not want to continue participating in the study. The case groups consisted of 19 males and 16 females and in control group there were 18 males and 17 females. Mean age on admission was 17.2±5.0 months (CI 95% 15.5-18.9) for case and 17±5.0 months (CI 95% 15.3-18.7) for control group. Mean temperature on admission was 39.25˚C (CI 95% 39.1-39.4) and 39.31˚C (CI 95% 39.15-39.40) for case and control group respectively. Mean weight on admission was 11.4 (CI 95% 10.9- 11.9) for case and 11.9 kg. (CI 95% 10.0- 13.0) for control group. Both groups had comparable clinical characteristics at admission including age, weight and temperature (Table 1). As Table 2 shows, there is significant difference between two groups in lowering fever at 4, 5, 7 and 8 hours after treatment was initiated, but there is no significant difference at 2 hours after drug was administrated. Major complications of administrated antifebrile drugs were not observed in patients. Discussion The aim of this study was evaluation of clinical effectiveness of acetaminophen alone, in comparison with an alternative regimen of acetaminophen and ibuprofen. As data of Table 1 shows, there was no significant difference between the two groups regarding distribution of age, sex, weight and degree of fever at admission. So any significant difference in reduction of fever could be attributed to the method of treatment. As Table 2 shows, there was no significant difference between the two groups in reduction of fever after two hours of antipyretic administration. Analysis of results at 4 hours post-treatment revealed that reduction of fever in group two which received ibuprofen (10mg/kg) was significantly less than the group treated with acetaminophen (15mg/kg). Meta analysis of seventeen double blind, randomized controlled trials in children who received ibuprofen and acetaminophen to treat fever, revealed that ibuprofen (5-10mg/kg) was a more effective antipyretic than acetaminophen (10-15mg/kg) at 2, 4 and 6 hours post-treatment[8]. Robertson disagrees with aforementioned results and believes there is not enough evidence to support that ibuprofen more effectively reduces fever[9]. Results of a study by Autert et al to find effect of the kind of drug on parent’s opinion revealed that in spite of equivalent efficacy and tolerability of ibuprofen at a dose of 10 mg/kg and paracetamol at a dose of 15 mg/kg, parents’ opinion was in favor of ibuprofen. Parents' positive opinion about ibuprofen, helped allay their anxiety over the treatment of their child[10]. In this study comparison between two groups at 5, 7, 8 hours after treatment, showed significant lower temperature in the case group (Table 2). Parallel to our results, another study was conducted to compare the antipyretic benefit of acetaminophen or ibuprofen monotherapy with an alternating regimen of both drugs in young children aged 6 to 36 months. Researchers concluded that an alternating treatment regimen of acetaminophen (12/5 mg/kg per dose) and ibuprofen (5 mg/kg per dose) every 4 hours for 3 days, regardless of the initial loading medication, is more effective than monotherapy in lowering fever in infants and children[11]. Another study entitled as “Alternating ibuprofen and acetaminophen in treatment of febrile children”, was conducted on patients aged 6 months to 14 years with rectal temperature ≥38.8. Researchers concluded that a single dose of ibuprofen and acetaminophen was superior antipyretic regimen than ibuprofen monotherapy[12]. Oral route was selected for administration of antipyretic drugs in this research. Nablusi et al designed a study to compare the antipyretic effectiveness of two rectal acetaminophen doses (15 mg/kg) and (35 mg/kg), to standard oral dose of 15mg/kg. They concluded that standard oral, rectal and high dose rectal acetaminophen had similar antipyretic effectiveness[13]. There are not enough articles on alternating acetaminophen and ibuprofen use in febrile children. The short duration of monitoring and of follow-up was the limitation of our study. In spite of results of this study; we do not recommend alternating regimen in clinical practice until further studies confirm the results. Conclusion An alternating treatment of acetaminophen (15 mg/kg) and ibuprofen (10 mg/kg) 4 hours later is more effective than acetaminophen monotherapy in lowering fever at 5, 6, 7 and 8 hours after administration in 9 to 24 month old infants. At four hours after drug intake ibuprofen reduces fever better than acetaminophen. Further studies are needed to confirm this conclusion. Acknowledgment Authors would like to thank members of University Council of Research and Ethics Committee of the University for their guides in all stages of the study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09026t2.jpg] [pe09026t1.jpg] |
| |||||||||

{kind=link}
{kind=link}