 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 393-398 Etiology and Outcome of Non-traumatic Coma in Children Admitted to Pediatric Intensive Care Unit Fariba Khodapanahandeh, MD; Najmeh Ghasemi Najarkalayee, MDDepartment of Pediatric, Rasool Akram Hospital, Iran University of Medical Sciences, Tehran, IR Iran * Corresponding Author; Address: Pediatric Ward, Rasool Akram Hospital, Sattar Khan Ave, Niyaesh St, Tehran, IR Iran, E-mail: fariba.khodapanahandeh@gmail.com Received: Nov 10, 2008; Final Revision: Mar 06, 2009; Accepted: Jun 05, 2009 Code Number: pe09047 Abstract Objective: Non-traumatic coma is a relatively common condition in children that may cause considerable mortality and morbidity. The purpose of this study was to determine clinical presentation, etiology and outcome of non-traumatic coma in children. Key Words: Non-traumatic coma; Morbidity; Epilepsy; Meningitis Introduction Non-traumatic coma (NTC) is a common cause of morbidity and mortality in children. Episodes were defined on the basis of a Glasgow Coma Score (GCS) of less than 12 for more than six hours[1,2]. Many acutely ill children are not fully conscious because pathologic processes may affect the parts of the central nervous system that mediate consciousness; alteration in the state of consciousness is a common feature of many different conditions. Many of these children make a full neurological recovery. However, depending on the underlying etiology non-traumatic coma may cause considerable mortality and morbidity in pediatric age group[2,3,4] Considering the fact that acute non-traumatic coma is a common problem in pediatric practice accounting for 10-15% of all hospital admissions, it makes a heavy demand on intensive care units[5]. Etiology of coma and clinical status at the time of presentation are likely predictors of outcome[2,6,7]. Outcome of non-traumatic coma was classified based on several prospective population based studies[2,3,7]. A better understanding of causes and outcome is essential to help to improve the approach and to plan rational management of non-traumatic coma. In a retrospective cross sectional study we reviewed the etiology, clinical signs and outcome of non-traumatic coma in a pediatric intensive care unit. Subjects and Methods In a cross sectional retrospective study files of 150 children aged between 1 month and 14 years admitted with non-traumatic coma to the pediatric intensive care unit of Rasool Akram Hospital over a period of 5 years (2002-2007) were reviewed. Coma was defined as significant depression of consciousness level as a GCS of less than 12 for more than 6 hours. In those less than 5 years of age modified GCS was used. GCS is checked routinely by our physicians and nursing staff in every child with altered level of consciousness. Children who presented with coma as a final stage of malignant diseases and those due to head trauma were excluded from the study. Presenting symptoms, historical, clinical and laboratory data were collected. The etiology of coma was determined on the basis of history, clinical signs, physical examination and relevant laboratory investigations (lumbar puncture, neuroimag-ing, metabolic work-up). Presenting manifestations were classified as CNS related, non CNS and organ specific. Etiology was classified into infectious, epilepsy, metabolic, intoxication, accidents, shunt dysfunction (secondary to congenital brain malformation), others (acute disseminated encephalomyelitis, vasculitis, hypertensive encephalopathy). Outcome was determined by patients' death or neurological condition at the time of discharge. Assessment of clinical neurological status included cranial and peripheral motor and sensory neurological examination, including cerebellar function performed for all children. Neurological outcome was divided into four groups:
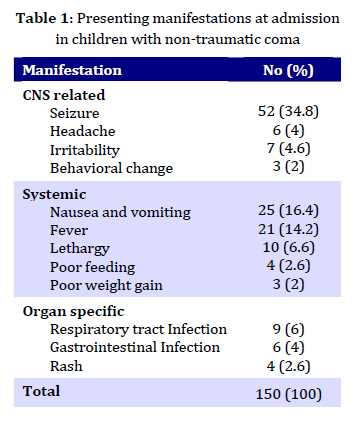
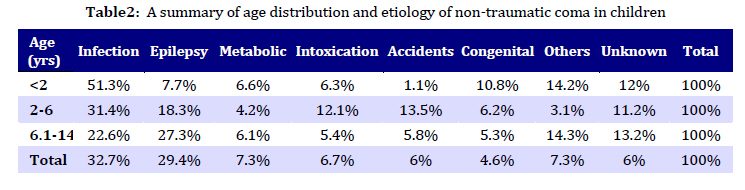
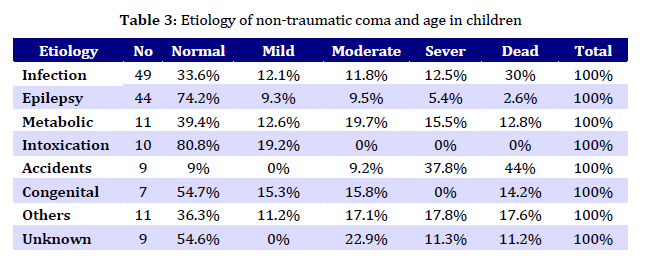
In assessing the effect of age on etiology and mortality, children were divided into three age groups: less than 2 years; 2-6 years; and 6.1-14 years of age. Statistical analysis was conducted using Statistical Package for Social Sciences (SPSS). Descriptive statistics expressed as mean and standard deviation. Chi-Square analysis was performed to test for differences in proportions of categorical variables between two or more groups. The level of P<0.05 was considered as being significant. Findings A total of 150 patients were included in the study. There were 63 (42%) boys and 87 (58%) girls. The mean age of patients was 2.47 years (range 1 month - 14 years ±2.35). There were 62 (41.3%) patients under the age of 2 years, 61 (40.6%) between 2 and 6 years and 27 (18%) between 6 and 14 years. Clinical manifestations at admission to PICU were divided into three groups: CNS specific, systemic and other organ related symptoms (Table 1). Systemic presentations were particularly evident in children less than 2 years of age (P=0.009) compared to other age groups. Infection (meningitis, encephalitis, respiratory and systemic) was the commonest cause of non-traumatic coma accounting for 49 (32.7%) cases followed by epilepsy (causing prolonged seizure activity leading to status epilepticus) as the second common etiology with 44 (29.4%) cases. Other etiologies were metabolic (diabetic ketoacidosis, inborn errors of metabolism) 11 (7.3%), intoxication (opiate, narcotics) 10 (6.7%), accidents (drowning, electrical shock, suffocation, etc) 9 (6%), shunt dysfunction secondary to congenital brain malformation 7 (4.6%), others (ADEM, vasculaitis, hypertensive encephalopathy) 11 (7.3%) and unknown causes 9 (6%). Infection and congenital etiology were significantly more common in children younger than 2 years of age (P=0.002 and P=0.009 respectively), whereas accidents and intoxications occurred more prominently in those between 2 and 6 years of age (P=0.004). Epilepsy causing prolonged seizure and altered level of consciousness was more common in children older than 6 years (P=0.008). Table 2 shows a summery of age distribution and etiology of non-traumatic coma. Outcome: 25 (16.6%) patients died and 125 survived. Of the 125 survivors 82 were discharged with normal neurological examination, 9 had mild disability, 18 were moderately disabled and 16 were severely disabled. There was a significant association between etiology and mortality. Accidents and infectious etiology had higher mortality compared with other groups (P<0.001 and P=0.02 respectively). Mortality was 25% (14 of 26) among those less than 2 years, 11.4% (7 of 61) among 2-6 years and 14.8% (4 of 27) among 6.1-14 years. Table 3 shows neurological outcome by etiology for all children.Discussion Consciousness requires normal functioning of both hemispheres as well as the ascending reticular activating system (ARAS). ARAS is a somewhat diffuse and poorly circum-scribed group of neurons that lie in the reticular formation of the brain which extends from the lower medulla to the midbrain and diencephalon. Coma is produced by disease or conditions that cause bilateral cerebral cortical dysfunction, or both. Childhood coma is a non-specific consequence of a variety of serious pathologic processes[8]. A practical classification for the etiology of coma in children produces three categories: infectious or inflammatory, structural, metabolic or toxic[9]. Infection was the commonest cause of non-traumatic coma in our study. The importance of infection as an etiology of non-traumatic coma is also supported by other studies[2,3,6,7]. The importance of infective etiologies in children is in sharp contrast to adult hospital based series where degenerative and cerebrovascular patholo-gies predominate[10]. Epilepsy causing prolonged seizure activity was the second commonest cause contributing to almost one third of cases of non-traumatic coma in our study. The result is compatible with the series from Britain and Nigeria[2,5]. In contrast, it was seen in only 5-10% of cases in some other studies[3,7]. Clinicians managing children in non-traumatic coma are often concerned that the illness may be the presentation of previously unrecognized inborn error of metabolism. In the present study 5 of 11 children in metabolic group had diabetic ketoacidosis. Two children had been diagnosed of metabolic disease prior to admission. In only four children the inborn error of metabolism was suspected as a result of the presenting episode of coma. In addition, three patients in unknown group had suspected metabolic causes for coma. Unfortunately, the exact type of inborn error of metabolism was not clear in our patients. The percentage of patients with metabolic disease in present study was comparable to other studies[2,7]. Systemic symptoms (nausea and vomiting, fever, lethargy, poor feeding, poor weight gain) occurred significantly in children less than 2 years old. This finding was compatible with other studies[2,3,7]. The overall mortality of 16.6% in present study was lower as compared to other pediatric hospital based series, 26% from Nigeria[6] and about 35% in India and Malaysia series[3,7]. Our mortality rate was slightly higher than UK study of 12%[2]. Although mortality following non-traumatic coma was high in these studies but it is considerably lower than reported adult hospital data where mortality rates of 60% and neurologically intact survivor rates of 10% are seen[10] In the present study incidence and outcome of coma was not associated with gender. Other studies did not show any significant difference in the incidence of coma between the two sexes either[2,6,7]. However, earlier studies[11] had shown a greater mortality in male (42%) compared to female children (20%). Mortality rate among children under 2 years was significantly higher in our study. Other studies also showed that mortality was higher in younger children[2,3]. In our study accidents and infectious etiology showed higher mortality rates compared to other etiology groups. In the study by Arun Bansal et al[3] infectious etiology resulted in highest death rate followed by toxic metabolic etiology. Study from Malaysia[7] also reported highest death rate in infectious group. Among survivors of infectious disease in our study only one third had normal outcome and the remainder left hospital with some degree of disability. This is compatible with Wong, Bansal and Sofiah studies[2,3,7]. In contrast, some earlier studies revealed that 60% to 75% of the infectious group had a good outcome compared with 36% and 47% respectively in the metabolic group[12-14]. Non-traumatic refractory increased intracranial pressure is a leading cause of morbidity and mortality in these children and decompressive craniotomy with or without opening the dura is an effective and lifesaving technique that should be considered[15,16]. Because of the retrospective nature of our study it was not possible to provide information on cognitive and adaptive outcome among survivors. Forsyth et al[13] have highlighted significant cognitive dysfunction following non-traumatic coma in childhood, and provided further support for the hypothesis of increased vulnerability of very young brains to cognitive malfunction following brain injury. Pediatric non-traumatic coma is an important health problem making significant demands of intensive and high dependency care resources. It can result from a wide variety of primary etiologies, posing a diagnostic challenge on medical staff. A better understanding of the causes and outcome of this heterogeneous group of children will aid a design of protocols for their investigation and management. Conclusion The present study demonstrated that infection was the commonest cause of non-traumatic coma. Accidents and infection etiology had higher mortality compared to other groups. Systemic presentations at admission were particularly common in children under 2 years of age. Acknowledgment The study was approved by the research committee of Iran University of Medical Sciences. We would like to thank nursing staff of the pediatric intensive care unit of Rasool Akram Hospital for their love and endless devotion to critically sick children. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09047t2.jpg] [pe09047t1.jpg] [pe09047t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}