 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
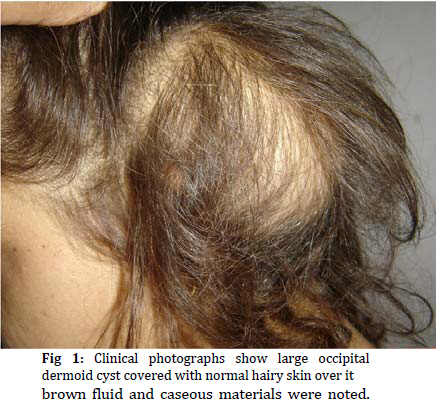
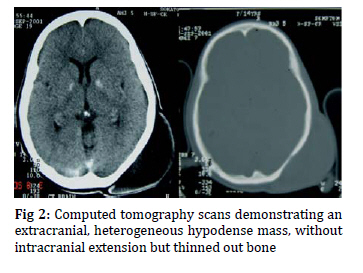
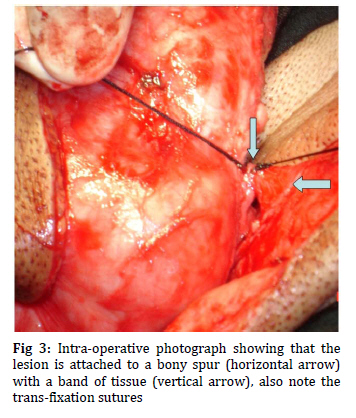
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp.439-441 Giant Asterional Dermoid Cyst with Dermal Sinus; a Case Report Amit Agrawal*1, MCh; Sudhakar Ratanlal Joharapurkar2, MS; Vinay Vasudev Shahapurkar1, MS1. Department of Surgery, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Wardha, India * Corresponding author; Address: Department of Neurosurgery, Datta Meghe Institute of Medical Sciences, Sawangi (Meghe), Maharashtra, India, E-mail: dramitagrawal@gmail.com Received: Sep 03, 2008; Final Revision: Dec 01, 2008; Accepted: Jan 23, 2009 Code Number: pe09057 Abstract Background: Dermoid cyst with dermal sinus in occipital region is extremely rare occurrence and still rarer in asterion region. We report a case of dermoid cyst with dermal sinus at the asterion probably the second case of world literature and discuss the findings. Key Words: Congenital; Dermoid cyst; Dermal sinus; Occipital; Asterion Introduction Dermoid cysts can occur anywhere along the midline of the cerebrospinal axis and anterior fontanel is being the commonest [1,2]. Dermoid cyst with dermal sinus in mid-occipital region is extremely rare occurrence [3,4] and still rarer in the lateral occipital (asterional) region[4]. These Dermoid sinuses occur due to the focal segmental adhesions between the superficial and neural ectoderm[5]. Later on the displaced cellular elements with cutaneous commitments become trapped between the dermis and the developing neural tube[6], resulting to a persisting tract lined by stratified squamous epithelium [7]. We report a case of dermoid cyst with dermal sinus at the asterion probably the second case of world literature and discuss the findings. Case Presentation 16 year-old female patient with mental retardation and inability to speak since childhood presented with history of progressive increasing swelling since childhood more so over last two years at the left side of occipital region. Local examination showed a giant, non-tender, soft, fluctuant, no-pulsatile, non-transilluminant swelling with healthy overlying skin over left side of occipital region (Fig 1). Swelling was freely mobile over the bone but it was fixed to skin. CT scan showed an extracranial hypodense mass, without intracranial extension but thinned out occipital bone on left side (Fig 2). The elliptical incision over scalp incision was marked followed by elevation of the galea above the cyst. The cyst was then dissected from the underlying tissue carefully and we found a bony spur that was not seen on CT scan and an attachment of cyst wall to it (Fig 3). During the procedure the general surgical team noted a cerebrospinal fluid (CSF) leak. As it was a very small communication we took a transfixation suture and excised. Cyst could be excised completely. After opening the cyst yellowish brown fluid and caseous materials were noted. Skin was closed without tension. Histological examination showed the cysts contained keratin debris, hair follicles, and some sweat and sebaceous glands, bordered by well-differentiated squamous epithelium suggestive of dermoid cyst. The patient has been on regular follow up with no recurrences. Discussion Cranial dermal sinus tracts are congenital lesions that originate from the midline scalp at the external occipital protuberance, at the nasion or along the nasal dorsum, or in the posterior parietal midline[4]. Dermal sinus with associated dermoid cyst arising in the lateral occipital region (asterion) is extremely rare [4]. Because of their location, these lesions can be confused with meningocele, sebaceous cysts, lipomas, cephalhematoma, lymphangioma or hemangioma[8,9,10]. Detailed and careful clinical examination supplemented with computed tomography (CT) and magnetic resonance imaging (MRI) imaging are effective for the preliminary diagnosis of such lesions and facilitate total removal, however the histopathology will confirm the diagnosis[4,5]. As in present case, the complete surgical resection with removal of the cyst wall will prevent the recurrence[3,4]. As we used in our case the recommended surgical technique is blunt dissection of the tumor from the underlying tissues including the dura mater or cranium through a curvilinear skin incision[3,4]. Extreme caution during surgical excision is advised particularly when these lesions are located in the vicinity of a sinus, the connection with the cranial venous confluence and unanticipated penetration can lead to rapid and fatal exsanguination [3]. In present case although the lesion was attached to the dura, however there was no apparent connection with the sinus. In present case the basal ganglionic calcification might be an incidental as this is now being diagnosed with increasing frequency, and it was not possible to establish a clinico-pathological correlation [11,12]. Conclusion Dermoid cysts over occipital region are the benign skin lesions and when excision is contemplated, careful attention must be paid during exploration. Failure to recognize intracranial communication in such lesions may result in fatal consequences [3]. In present case communication was in the form of small dermal sinus with a bony spur. Pre-operative suspicion of such a connection helped us to identify the underlying defect intra-operatively and facilitated safe excision. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09057f3.jpg] [pe09057f1.jpg] [pe09057f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}