 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 1, January-March, 2011, pp. 39-44 Tuberculin Reactivity in School Age Children; Five-year Follow-up in Iran Mitra Hemmati, MD; Keyghobad Ghadiri, MD, and Mansour Rezaei, PhD Infectious Disease Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran * Corresponding Author; Address: Imam Reza Hospital, Kermanshah, Iran E-mail: k_ghadiri@yahoo.com Received: Mar 12, 2010; Final Revision: Jun 26, 2010; Accepted: Sep 17, 2010 Code Number: pe11007 Abstract Objective: Tuberculosis
(TB) is an important infectious disease worldwide. Tuberculin skin
test (TST) is the standard test for diagnosis of tuberculosis infection; Bacillus
Calmette-Guerin (BCG) vaccination
at birth has effects on this test. The aim of this study was to determine
the prevalence of positive TST cases among 7- to 11-year-old primary
school children and also to follow test-positive individuals for a
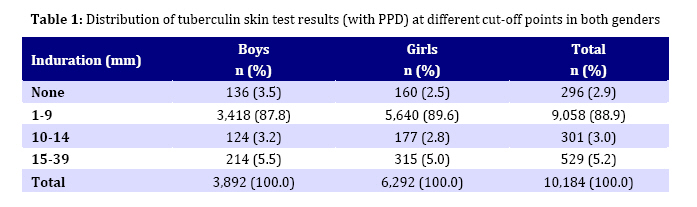
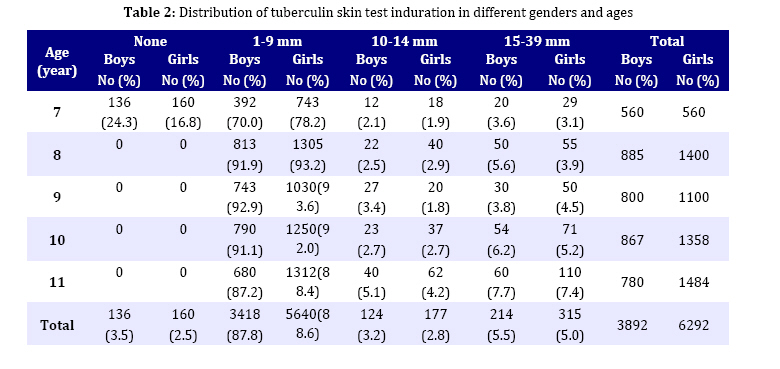
five-year period. Key Words: Tuberculin Test; BCG; Vaccine; PPD; Tuberculosis Introduction Tuberculosis (TB) continues to be an important public health problem worldwide and according to World Health Organization reports there were about 8.8 million new cases and 1.6 million deaths from the disease in 2005. Without treatment, about two-thirds of smear-positive pulmonary cases die within five to eight years[1]. According to East Mediterranean Regional Office (EMRO) records, the estimated incidence of tuberculosis in Iran in 2004 was 13-24 per 100.000[2]. The notification rate of TB in Iran is estimated to be less than 70%[2,3]. This means that considerable numbers of patients are missed in the early stages of disease. Tuberculin Skin Testing (TST) has been used for a long time as a diagnostic test for latent tuberculosis infection and at present it remains the only routinely available method for the diagnosis of tuberculosis. It is an easily applied and low cost test that can determine annual risk of tuberculosis infection[4]. TST positivity differs among Bacillus Calmette-Guerin (BCG) vaccinated and unvaccinated populations[5,6]. Tuberculin-positive children from high prevalence countries are regularly given treatment for latent TB infection in the United States[7]. Such treatment is seldom recommended in the absence of other risk factors like recent contact with smear positive pulmonary TB in young children or immunodeficiency conditions because about 90% of patients who developed TB in some countries were infected ten years before[8,9]. However, infection with mycobacterium other than Mycobacterium tuberculosis and previous BCG vaccination also cause reaction to tuberculin, though in a BCG vaccinated patient positive skin tests with indurations of ≥10 mm are more likely to be the result of tuberculosis infection rather than vaccination[10-12]. In many countries BCG vaccination is regularly performed[13]. Iran is an example where for the past 40 years, BCG vaccine has been given to all newborns with a coverage rate of about 99%. Partly as a result of widespread neonatal BCG vaccination, the 15 mm cut-off point for purified protein derivative (PPD) test has been consistently used in our study. The purpose of our study was to determine the rate of TST positivity and prevalence of TB infection in 7- to 11-year-old children and determine active TB disease during a five-year period in Kermanshah in western Iran. Subjects and Methods Primary school children (age range 7-11 years) were eligible for this study which was done in Kermanshah, Iran from January to May 2002. Selection of the subjects was achieved using cluster random sampling. In each school a classroom from each grade (grades 1-5) was selected. Then, all the students of selected classrooms were evaluated. Using this method, a total number of 10.184 students (3.892 boys and 6.292 girls) were studied TST was performed by intradermal injection of 0.1 ml of 5 tuberculin units (5TU) of PPD from Mycobacterium tuberculosis that was supplied by Razi Institute administered by Mantoux technique. After 72 hours the result for the biggest diameter of indurations (in millimeters) was recorded by trained healthcare workers. The tuberculin positive rates at the cut-off points of ≥10 and ≥15 mm for different sexes and ages were recorded. The results of the tuberculin skin test were interpreted in the context of the patient's risk of M. tuberculosis infection and cut-off point ≥15 mm was considered as tuberculosis infection. Those who had a positive test were followed for five years. In addition to TST results, additional data was collected using school records and checklists. The data were age, sex, history of BCG vaccination, presence of BCG scar, risk factors of tuberculosis infection such as close contact with a person who has active pulmonary tuberculosis, or immune-compromising conditions. Students with positive TST were given the option of being examined by the study physician. History and physical examination were performed to determine the presence of symptoms of TB disease and chest radiography to exclude active TB disease. During the five-year period of follow-up, periodic history taking, physical examinations, and if necessary chest radiography and sputum examination were done in TST-positive cases. For comparison of categorical variables, the chi-squared test was used. To assess the independent effects of sex and age on the positive tuberculin response at different cut off points, multiple logistic regression model was used. A P-value of <0.001 was considered statistically significant. Findings Positive TST results were observed in 830 students; 529 (5.2%) cases had an induration equal to or more than 15 mm and the remaining 301 (2.96%) cases had an induration of 10-14 mm. Skin test indurations ranged from 0 to 39 mm (Table 1). The mean induration in males measured 8.7mm, slightly more than 7.8mm induration in females (P=0.1, Table 1). At the cutoff point ≥5 mm, 40.3 percent (95% CI: 39.3-41.2) of girls had positive tuberculin test compared with 43.8 percent (95% Cl: 42.8-44.8) of boys and at the PPD5 induration 10 mm, 7.9 percent (95% CI: 7.4-8.4) of girls and 8.7 percent (95% CI: 8.2-9.2) of boys had positive TST. At the cut-off point ≥l5 mm the corresponding rates of TST positivity were 5.1 percent (95% CI: 4.7-5.5) and 5.5 percent (95% CI: 5.1 - 5.9) respectively (P=0.014). A significant linear trend was found between the rate of TST positivity and age at all cut off points which persisted when the two sexes were analyzed separately. By using trend chi-squared test, we found that increasing age was significantly associated with positive TST reactions (P<0.001) (Table 2), About 99.2% of participants had history of BCG vaccination at birth and 96% of them had BCG scar. Of 529 children with TST ≥15 mm, 480 (90%) cases presented for follow up after one year and 457 (86%) cases after two years, but only 290 (55%) subjects completed the five-year follow-up. They did not have any risk factors for TB such as close contact with a person with active pulmonary tuberculosis, or immune-deficiency conditions. After 5 years, no new case of active TB was detected. Further evaluation was done using the medical records of TB Registry of Kermanshah Province that records all forms of TB in the province. According to these records, none of the studied children in this study had been diagnosed as active tuberculosis. Discussion Our study found the rate of 8.15% TST positivity with no new case of active tuberculosis detected within 5-year follow-up. Mass school screening in New York[14] and Boston[15] showed less than 3% and 5.1% to 8.9% rates of TST positivity, respectively. In Southeast Asian teenagers, this rate was 55%[16]. Pong et al found rates of 12.8 and 24 percent in two American high schools[17]. At cut-off point of ≥5 mm, about 40% of our patients had positive TST. This is in contrast to the observation by Sakha et al in Tabriz, where only 4.66% of children had such a rate[18]. In south Iran[4] and Kerala, India[19] this rate has been reported as 6.1% and 5% respectively, which are lower than ours. According to the current findings, there were no significant differences between TST positivity rate between boys and girls at any induration cut-off point. This observation is similar to two former studies from San Diego[17] and Canada[20] being in contrast to a report from Hong Kong that showed female predominance regarding TST positivity[12] and two other reports which showed male predominance in Norway and Philippines[21,22]. It was observed that increasing age after 9 years is significantly associated with increasing rate of TST positivity at cut-off point of ≥15 mm in both genders. This finding resembles those of San Diego[17] and Hong Kong[23] studies but is in contrast to some other studies that have shown reduction in the tuberculin response in younger children who had been vaccinated at birth[24,25]. This might mean that reduction in the BCG effect has either stopped or been masked by a higher rate of tuberculin conversion due to tuberculosis infection or exposure to non-tuberculosis mycobacterium in our cases. In this study BCG vaccination coverage rate was 99.2% and 96% of children had BCG scar. However, in a report from Delhi, India[26] BCG vaccination coverage was 90% in urban and 84.7% in rural areas. According to Kumar study, about 81% of the children had BCG scar[19]. In Sri Lanka, despite having 97% BCG scar, 80% had tuberculin anergy (0-l mm) and there was no correlation between scar size and Mantoux response[25]. Mean tuberculin indurations in our study were 8.7mm and 7.85mm in male and female respectively; this is in contrast to a Turkish study with 2.7±2.96mm in 5-7 years age group[5]. The lifetime risk of tuberculosis reactivation for a person with a positive tuberculin skin test is usually estimated to be 5 to 10 percent, half of which is in the first year after infection[23,27,28] . In our study school children with positive PPD ≥15 mm were followed for 5 years and no active TB disease was detected. No case of active TB also was recorded in the TB registry of Kermanshah Province. If we assume that the lifetime risk of tuberculosis reactivation for a person with a positive tuberculin skin test usually is 5 to 10 percent and half of which occurs in the first year[27,29,30] we should have detected many cases of active TB. The great majority of infants who have received BCG vaccination would lose reactive skin test by 5 years of age[31] and reactions of ≥10mm induration are in favor of mycobacterial infection than vaccination or other mycobacterial infections[32,33]. So at the cut-off point of ≥15 mm among school children in this study, reaction is due to infection with Mycobacterium tuberculosis but none of them developed active disease. We conclude that the developing of disease is less than 5 to 10% in Kermanshah, Iran. In a study in Singapore, 17% of school children who were vaccinated at birth had a TST ≥10mm at 12 years of age. These children were followed for 4 years and found to have a 5 to 48-fold increased risk of developing TB disease when compared with children whose TST had been <5 mm at 12 years of age[34]. Among school children incidentally found to have a tuberculin reaction at 20mm or more, the annual incidence of active TB was as high as 341 per 100.000[35]. Even in low-prevalence areas, TB has been diagnosed in 55% of immigrants within the first 5 years of arrival. In many countries with high TB prevalence, neonatal BCG vaccination is regularly performed, this may have effect on tuberculin skin test but results of our and other studies[12,36] suggest that the effect of BCG on tuberculin response may be more complex than was previously assumed. Parents of the students, who did not complete follow-up, when contacted by phone, said they believed their child did not have any particular disease and there was no need for presentation to physician. Conclusion We found TST positivity rate of 8.15% in 7- to 11-year-old students, and during 5 years follow-up no case of active disease was diagnosed. Acknowledgment The authors declare that there is no conflict of interest and confirm that informed written consent was obtained for publication of the manuscript. We acknowledge the ethic committee of Kermanshah University of Medical Sciences, Kermanshah Education and Training Organization, Mr. Amirhosain Hashemian, and healthcare workers for their assistance. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11007t2.jpg] [pe11007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}