 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 20, No. 2, Apri l-June, 2011, pp. 151-158 Bubble–CPAP vs. Ventilatory–CPAP in Preterm Infants with Respiratory Distress Bahareh Bahman-Bijari1, MD; Arash Malekiyan1, MD; Pedram Niknafs1, MD, and Mohammad-Reza Baneshi2, PhD
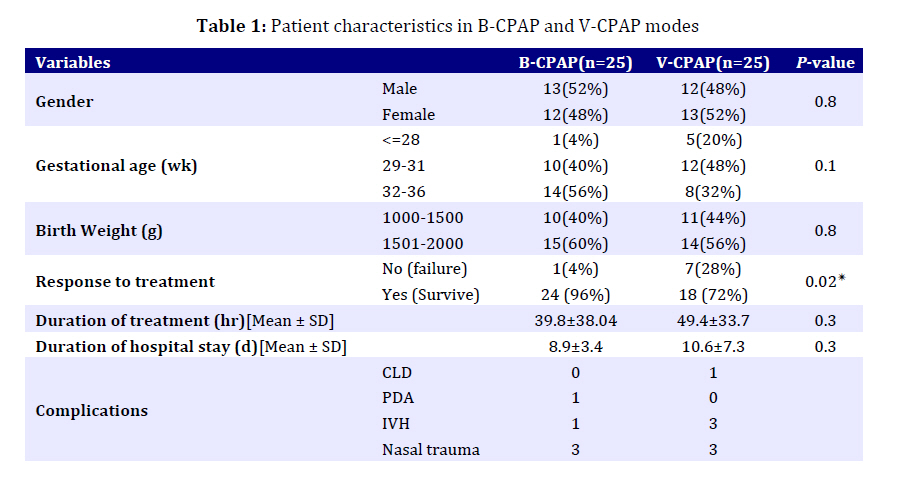
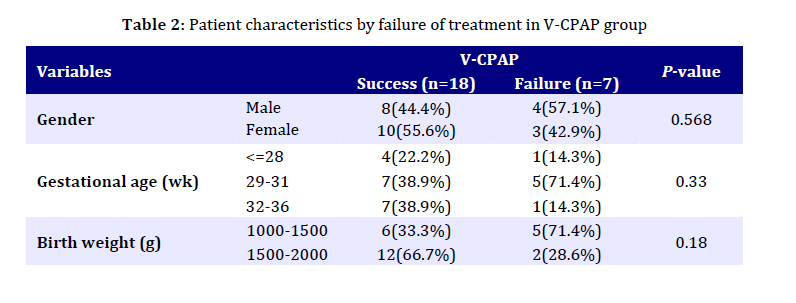
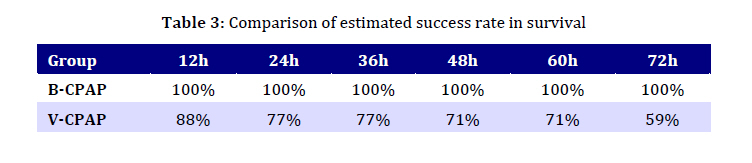
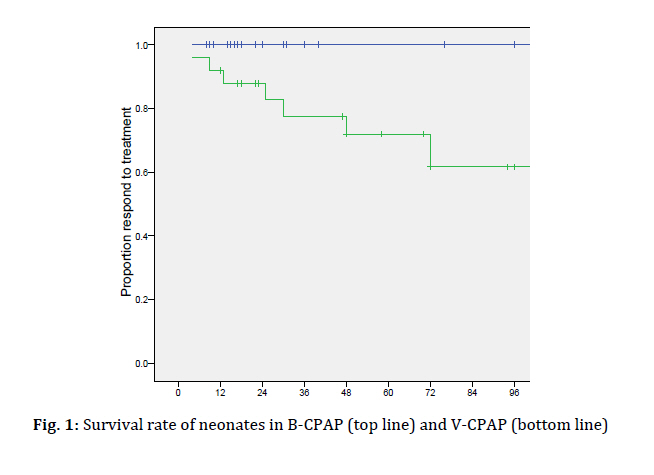
Received: Jun 23, 2010; Final Revision: Nov 28, 2010; Accepted: Jan 10, 2011 Code Number: pe11027 Abstract Objective: Application of Continuous Positive Airway Pressure (CPAP) in neonate with respiratory distress is associated with reduction of respiratory failure, reduced complications and mortality. Bubble CPAP (B-CPAP) and ventilator-derived CPAP (V-CPAP) are two most popular CPAP modes. We aimed to determine whether B-CPAP and V-CPAP would have different survival rate and possible complications. Key Words: Continuous Positive Airway Pressure; Bubble CPAP; Ventilator-derived CPAP; Respiratory Distress Introduction Neonatal respiratory failure is a serious clinical problem[1–3] associated with high morbidity, mortality, and cost[4–6]. The major risk factor is low birth weight[7,8], which is more prevalent among the poor, and the uninsured[9–12]. The standard method of management for respiratory failure is supportive care with mechanical ventilation and high concentration of inspired oxygen. A study in the United States reports a mechanical ventilation rate of 18 per 1,000 live births and the total cost of $4.4 billion for treating respiratory failure[13]. There is increasing enthusiasm for non-invasive respiratory support of preterm infants. Devices used to generate CPAP include conventional ventilators, the “bubbly bottle” system and the infant flow driver[14]. The Infant flow driver has been shown to be a feasible device for managing respiratory distress syndrome in preterm infant[15]. CPAP is used in infants with respiratory distress and apnea[16,17]. CPAP supports the breathing of preterm infants in a number of ways. It splints the upper airway and reduces obstruction and apnea, assists expansion of the lungs, and prevents alveolar collapse[14]. Underwater bubble CPAP (B-CPAP) and ventilator-derived CPAP (V-CPAP) are two of the most popular CPAP modes, and they use different pressure sources. In V-CPAP, a variable resistance in a valve is adjusted to provide resistance to the flow of air[18]. In B-CPAP the positive pressure in the circuit is achieved by simply immersing the distal expiratory tubing in a water column to a desired depth rather than using a variable resistor[19,20]. Lee et al[19] demonstrated the superiority of B-CPAP as compared to V-CPAP in premature infants. Teresa et al[21] showed that the use of B-CPAP is a potentially useful practice among very low birth weight infants with RDS. Although these two different pressure sources for CPAP delivery have been used for three decades, surprisingly there are no large randomized trials of B-CPAP vs conventional management with mechanical ventilation, a fact that reflects the common dilemma in clinical research. Conducting a large trial too early risks failure due to both inadequate knowledge of optimal treatment strategy to design the trial correctly and lack of expertise in the use of the new technique/device[22]. What is clear, however, is that in resource-limited settings B-CPAP is an effective and inexpensive way to provide respiratory support that appears to be at least as good as the respiratory support generated by far more expensive equipment[23]. Whether B-CPAP has any advantages over standard CPAP remains to be determined. The objective of the present study was to compare the survival rate of neonates with respiratory failure treated with application of B-CPAP vs V-CPAP and to study any possible complications caused by these methods. Subjects and Methods This study was conducted at a level III neonatal care unit of Afzalipoor Hospital between June 2009 and May 2010 in Kerman University of Medical Sciences. The aim of this study was to compare the effectiveness of B-CPAP and V-CPAP in the treatment of neonates with respiratory distress syndrome. All of the patients were inborn (gestation 28 to 36 weeks). All consecutively born preterm infants with birth weight between 1000 and 2000 grams who had respiratory distress and a Silverman-Anderson retraction score[24] of 6 and 7 were included. Babies were excluded if there was significant morbidity apart from RDS including cardiac disease (not including patent ductus arteriosus [PDA]), congenital malformation including congenital diaphragmatic hernia, tracheoesophageal fistula, and cleft lip/palate, and babies who had either respiratory distress secondary to severe asphyxia (Apgar score£3 at 1 and 5 minute or pH£7.12), cardiovascular or respiratory instability because of sepsis, anemia, or severe intraventricular hemorrhage (IVH) on admission. Setting the power and type-one error at 80% and 5%, we have estimated that the total number of patients required was 50 (i.e., 25 per treatment group). To randomly assign patients into treatment groups, the minimization technique was applied with respect to baby's gender and birth weight (£1500 vs >1500 grams). By implementing this method, we balanced the gender and weight distribution in treatment groups. In both groups CPAP was implemented nasopharyngeally. Indication for CPAP included (i) FiO2 >0.4 to maintain PaO2 ≥60 mmHg associated with pH<7.25; and (ii) PaCO2 <50 mmHg[25]. The Fisher and Paykel Bubble-CPAP (BC161, New Zealand. UK) involves a source of gas flow (6-8 L/min), an air oxygen blender (Biomed Devices Belendez. USA), humidifier (MR410, Fisher & Paykel Health Care. New Zealand), and a respiratory circuit. The expiratory hose is inserted in a bottle of water. CPAP level delivered is equivalent to the distance that the distal end of expiratory tubing is underwater, which was submerged under 5 cm of water to obtain 5 cm H2O of CPAP in our study. The Bear 750 PSV (Bear Medical System, Inc. US) Ventilator-derived CPAP also provided base flow of gas at a rate of 5 L/min; however, its hose was connected to the exhalation valve of the ventilator. The pressure tube was connected to the Y-piece and the pressure was adjusted at 5 cm H2O. CPAP was considered to be successful if the respiratory distress improved and the baby could be successfully weaned off CPAP. The criteria for weaning was absence of respiratory distress (minimal or no retractions and respiratory rate between 30 and 60 per minute) and SpO2>90% on FiO2 <30% and PEEP <5 cm of water. Mechanical ventilation was considered for failure of CPAP; i.e., in babies with PaO2 <50mmHg or PaCO2 >60 mmHg and pH<7.25 with FiO2 >0.6; or those with clinical deterioration (increased respiratory distress) including severe retractions on PEEP >7 cm of water; or prolonged (>20 seconds) or recurrent apneas (>2 episodes within 24 hours associated with bradycardia) requiring bag and mask ventilation[26,27]. Infant variables evaluated included birth weight, gestational age, Apgar score at 1 minute, delivery room management (oxygen, bag and mask, intubation), chest X-ray, arterial blood gas, FiO2 requirement and treatment with surfactant (Survanta). The main outcome of this study was survival rate. We applied survival analysis to compare the survival rate in the treatment groups at different time points. By definition the survival function is the probability of observing a survival time greater than some stated value X. This indicates that being event free all the way to the end of Xth year depends on no event in any of the preceding years, and also none in the Xth year, so this method considers aging information. To display the results graphically, Kaplan-Meier curves were plotted. The Log-Rank test was applied to compare survival curves across treatment groups. We also compared treatment options in terms of duration of oxygen therapy, duration of hospital stay, and hospitalization costs. We reported the incidence of neonatal morbidities in 2 treatment groups: pneumothorax, PDA by echocardiography (Spacelabs Medical. USA), IVH by cranial ultrasonography (Accuvix10) performed by our neonatologist who was blinded to failure as an outcome which was typically performed on admission day, day 7, and when the baby failed each mode of treatment, severe IVH (grades III-IV), chronic lung disease (CLD), and trauma to nasal septum and nostrils. Independent sample t and Chi-square tests were used to compare continuous and categorical variables between treatment groups, respectively. All analyses were performed using SPSS version 15 at a significance level of 0.05. The study protocol was approved by the local ethical committee of Kerman University of Medical Sciences (Ethic Code: K-88-235). All parents signed informed consent forms before participating in the study. This study has been registered in Iranian Registry Clinical Trail (IRCT.ir) (Irct ID: IRCT13890208325 0N2). Findings As summarized in Table I, the B-CPAP and the V-CPAP groups had comparable demographic characteristics. Bubble-CPAP proved to be effective in 24 (96%) babies; only 1 baby required mechanical ventilation on the 6th day. Ventilator-derived CPAP was effective in 18 (72%) patients. A total of 25 babies received surfactant (Survanta): 12 in B-CPAP and 13 in V-CPAP group with no significant difference. A total of 4 neonates had IVH: 1 in B-CPAP group and 3 in V-CPAP group. None of the babies developed pneumothorax. Nasal trauma was seen in 12% of patients, but this did not include trauma to septum; the only complication was minimal nostril lesions all of which had improved before discharge. Mean treatment duration in B-CPAP was not statistically significantly different from V-CPAP (39.8h vs 49.4h). Focusing on patients who responded to treatment, the mean duration of treatment for the two groups was 35.5±31.92h and 57.5±33.99h respectively and the difference was statistically significant (P=0.04). Also, we found a significant difference between B-CPAP and V-CPAP for the mean duration of hospital stay (8.7±3.3 vs 11.9±7.8 days, respectively). The characteristics of patients who did not respond to V-CPAP are given in Table 2. Neither sex nor birth weight influenced the response to treatment. No similar analysis was performed for the B-CPAP group since only 1 patient did not respond to the treatment applied. We also compared the survival rates between the two treatments every 12 hours (Table 3). In the first 3 days, the estimated survival rate in the B-CPAP group was 100%. However, in the V-CPAP group a decrease in survival rate was seen. In the first 24 hours the difference between survival rates was about 25% (100% in B-CPAP vs 77% in V-CPAP), indicating the vital importance of the first hours of management of patients. The survival rate of neonates who received V-CPAP was 59% at the end of the 3rd day and remained constant afterward (Fig 1). The Log-Rank test confirmed a significant difference between the survival curves. It should be noted that when we developed a multifactorial Cox regression to adjust the treatment effect in the presence of other variables, the model did not converge to a solution. This was because only one event occurred in the V-CPAP group. The mean duration of hospital stay and treatment time were similar in the 2 treatment groups in neonates weighing <1500g (P-values =0.84 and 0.63, respectively); however, the mean duration of hospital stay and treatment time of neonates weighing >1500 g were significantly longer in the V-CPAP group (25.26±17.09 h and 7.2±2.6 d in B-CPAP vs 47.2±30.24 h and 9.5±2.9 d in V-CPAP). The mean cost of hospitalization in the B-CPAP and V-CPAP groups was $947.3±726 and $1436.7±934, respectively, and the difference was significant (P=0.04). Discussion The main goal of this study was to compare the effectiveness of and complications associated with B-CPAP and V-CPAP. The role of CPAP in treating the neonatal respiratory distress was already well known. Different modalities of ventilators and systems producing CPAP have provided opportunities to compare these methods. Our findings showed that the failure rate associated with B-CPAP was lower than that associated with V-CPAP, which was inconsistent with the results of the study carried out by Tagare et al[28]. Likewise, Lee[19] showed that B-CPAP was significantly more effective than V-CPAP. On the other hand, the studies by Morley[29] and Pillow[30] demonstrated that B-CPAP increases the respiratory effort in the neonate more so than V-CPAP. We observed only one single failure in the B-CPAP group in our study; we did not investigate the cause for this failure. However, in the study by Ammari[31] the CPAP failure observed was associated with positive pressure ventilation at delivery and severe RDS. Also, Urs[26] noted that the chance for success was limited to patients with mild to moderate RDS. In our survey the hospital stay and treatment in neonates weighing more than 1500 g differed between the B-CPAP and V-CPAP groups and this was not shown in patients weighing less than 1500 g. In another study[32] the positive effect of B-CPAP was seen in neonates weighing more than 1250 g, and in the study by Tagare[28] the hospital stay was longer in the B-CPAP mode than V-CPAP. B-CPAP delivers mechanical oscillatory vibrations that simulate waveforms produced by high-frequency ventilation (HFV)[19,33]. Accordingly, B-CPAP may possess the characteristics of CPAP and HFV at the same time. It has been reported that hemodynamics is better preserved during HFV than during conventionally controlled mechanical ventilation[34,35], and also when using B-CPAP[36]. In this study we did not investigate the hemodynamic changes in the two groups but that may be why we saw fewer IVH cases among those who were under B-CPAP. Several studies have shown that the “Columbia approach”[37,38], in which B-CPAP is used early in the course of respiratory distress in both premature and term-gestation infants, can effectively lower the incidence of CLD[39-41]. At Columbia University, the early initiation of nasal prong B-CPAP in combination with a tolerance to elevated PCO2 levels has been shown to reduce the incidence of CLD to <5% in infants weighing less than 1500 g[42], consistent with our findings. The mean cost of hospitalization was lowered by using B-CPAP in our study. Lanieta et al[43] have successfully demonstrated the usefulness of B-CPAP in a developing country, and have also reported the cost effectiveness of B-CPAP. Pieper et al[44] have shown the importance of CPAP in the absence of neonatal intensive care and also the improved outcome in neonates treated with CPAP prior to transfer to a tertiary unit. The small sample size of this study does limit its applicability. A multicenter randomized controlled trial is needed to further confirm these findings. Conclusion Based on our results B-CPAP seems to be superior to V-CPAP in terms of treatment of RDS in preterm infants due to fewer complications, shorter hospital stay, and lower cost. The simplicity and low cost of B-CPAP compared with V-CPAP makes it an attractive option in resource-poor setups. Acknowledgment The authors thank the research Deputy of Kerman University of Medical Sciences for the financial support. The authors also wish to thank the personals of NICU of Afzalipour Hospital for their assistance. Conflict of Interest: None References
Copyright 2011 - Iran Journal of Pediatrics The following images related to this document are available:Photo images[pe11027f1.jpg] [pe11027t2.jpg] [pe11027t3.jpg] [pe11027t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}