 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 8, No. 1, April, 2004 pp. 29-36 Breaking the Cycle of Unsafe Abortion in Africa Charlotte Hord1 and Merrill Wolf1 1Ipas, 300 Market Street, Suite 200, Chapel Hill, North Carolina,
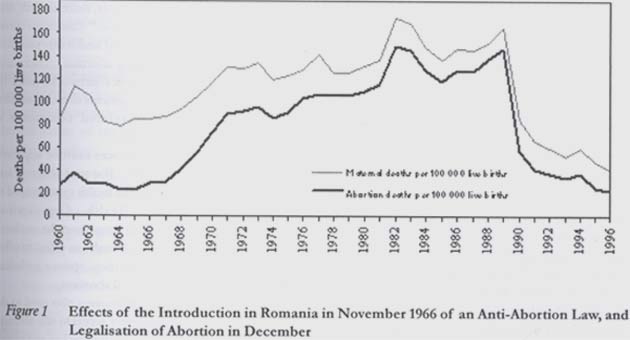
USA. Code Number: rh04006 Abstract Globally, nearly half of all maternal deaths from unsafe abortion occur in Africa. Abortion-related deaths and injuries are especially tragic, because when properly performed, abortion is one of the safest of all medical procedures. Factors contributing to this neglected public health crisis include inadequate health care resources and infrastructure, restrictive laws and policies, stigma, and women's lack of empowerment. Actions needed include making high quality abortion care more available and accessible, especially at the primary care level and to the full extent permitted by law. Others include removing medically unnecessary policy and legal restrictions on abortion; and better informing health care professionals, women and communities about the impact of unsafe abortion and the circumstances under which abortion can be legally obtained. (Afr J Reprod Health 2004; 8[1]:29-36) Key Words: Unwanted pregnancy, abortion, reproductive health, women's health, women's rights, Africa, pregnancy termination, maternal mortality Résumé Rupture du cycle de l`avortement à risqué. Dans le monde entier, presque la moitié de tous les décès maternels occasionés par l`avortement à risque se produisent en Afrique. Les décès et les blessures liés à l`avortement sont particulièrement tragiques, parce que quand il est bien fait, l`avortement est une de plus sûre de toutes les procédures médicales. Parmi les facteurs qui contribuent à cette crise négligée de santé publique sont les ressources et l`infrastructure de soin médical peu adéquates, les lois et les politiques restrictives, le stigmate et le manque de pouvoir économique chez les femmes. Parmi les mesures nécessaires sont la mise en place du soin d`avortement qui sera plus disponible et plus accessible, surtout au niveau du soin primaire et jusqu`au point autorisé par la loi. En plus, il faudra supprimer la politique médicale inutile et les restrictions légales sur l`avortement, mieux informer les professionnels de soin de santé, les femmes et les communautés sur l`impact de l`avortement à risque et sur les circonstances sous lesquelles l`avortement peut être légalement obtenu. (Rev Afr Santé Reprod 2004; 8[1]:29-36) Introduction Despite decades of rhetoric by the international community, maternal mortality - or deaths of women related to pregnancy and childbirth - remains stubbornly and unacceptably high in many of the world's poorest countries. In fact, the disparity between levels of maternal mortality in developing and industrialised countries is greater than for any other health indicator.1 In wealthy countries, widespread, though hardly universal, access to high quality obstetric and related care ensures that pregnancy and motherhood are safe experiences for most women. But inadequate access to such services continues to pose a serious threat to the lives and well being of their poorer sisters in developing countries, with lack of access to such care being the rule rather than the exception in most settings. One important contributor to pregnancy-related deaths, especially in the developing world, is unsafe abortion, which alone among all causes of maternal mortality is almost entirely preventable. That the world community and national and local authorities have not devoted more attention and resources to this phenomenon bespeaks the pervasive stigma surrounding not only abortion but also broader issues of sexuality, reproduction and women's empowerment. Globally, the taboo surrounding HIV/AIDS has diminished at least enough to support increasingly effective efforts to address the pandemic, but a terrible silence still shrouds the tragedy of unsafe abortion. Especially in Africa, it is time to replace that silence with bold speech and action. This paper outlines the scope of the problem of unsafe abortion on the African continent including its consequences for women, families, communities and societies. We then enumerate several priorities for action, underscoring that the solutions to this problem are well-known, practical and affordable, and that if the lives and health of women are valued, African countries have no time to waste in applying these proven approaches. Unsafe Abortion: A Critical Reproductive Health Problem The World Health Organization (WHO) defines unsafe abortion as a procedure for terminating unwanted pregnancy that is performed by someone lacking the necessary skills or in an environment lacking minimal medical standards or both.2 This rather clinical definition obscures the reality of unsafe abortion, which in many cases is gruesome and always tragic. Those 25 words do not begin to convey the desperation felt by women and girls who, facing unwanted pregnancies and left with no better option, too often resort to crude methods and unskilled practitioners to resolve their intensely personal dilemmas. When properly performed, abortion is one of the safest of all medical procedures. In countries where women have access to safe services, they run a very low risk of death from unsafe abortion; less than one per 100,000 procedures.3 Nevertheless, unsafe abortion is an extremely common occurrence, with often deadly results especially in Africa. It is a significant contributor to the larger problem of global maternal deaths, of which Africa suffers a disproportionate burden. An African woman who reaches reproductive age has triumphed over many childhood threats but still faces numerous risks. According to the World Health Organization, one in 11 girls in East Africa will have her life cut short or her health harmed by a pregnancy-related cause, compared to one in 4000 in Western Europe. In Africa overall, the statistics are not much better; an average of one in 16 African women will die during pregnancy or childbirth. Considered another way, African women face a risk of death from pregnancy-related causes that not only is many times greater than that faced by women in developed countries, but also is significantly higher than the risks that women in other developing regions confront.4 In Africa, as globally, unsafe abortion is a leading cause of maternal deaths, accounting for a global average of 13% of fatalities related to pregnancy.5 WHO estimates that of a worldwide annual total of 46 million abortions, 19 million are unsafe.3,6 The vast majority of these unsafe procedures, about 95%, occur in developing countries.5 And the greatest percentage, more than one quarter of the total or about 4.2 million unsafe abortions each year, occur in Africa.6 According to 1995 estimates, nearly 100% of all abortions in Africa are performed illegally.7 Clearly, if the region's predominantly restrictive abortion laws are meant to prevent abortions from happening, they are not working. Country-based studies show much higher estimates for annual numbers of abortions than is evident from global or regional averages. In Nigeria, for instance, where abortion is permitted only to save the life of the woman, there are an estimated 610,000 abortions performed each year.8 Many of these abortions are undoubtedly performed unsafely, as evidenced by hospital-based studies in Nigeria that report that between six and 51% of maternal deaths are caused by unsafe abortion.9 These figures indicate that there are 25 abortions per 1,000 women aged 15-49 years, a rate much higher than most Western European countries and close to the 1995 US rate of 23 abortions per 1,000 women of childbearing age.8 African women also face the highest risk of death from abortion-related complications. WHO estimates that around the world nearly 70,000 women die every year from complications of unsafe abortion.3 This translates to approximately 190 deaths per day; about the equivalent of a fatal jumbo jet crash with nearly 400 people on board every two days year round. How does death on such a massive daily scale not raise a global outcry? The only possible explanation is that societies do not value the lives or contributions of women enough to raise the alarm. Unfortunately, this lack of response may also reflect the fact that the primary victims of unsafe abortion are not only women but African women. More than 40% of all deaths due to unsafe abortion globally occur in African countries.5 Every year, about 34,000 African women die from this totally preventable cause.5 Importantly, this figure is widely acknowledged to be a gross under-estimation. Beyond the tens of thousands of deaths already mentioned, unsafe abortions take their toll on women, families and communities. Experts estimate that for every woman who dies from unsafe abortion, many more suffer serious, often long-term, injuries and disabilities. Potential complications of unsafe abortion include uterine perforation, haemorrhage and infection, sometimes leading to pelvic inflammatory disease and partial or total infertility. A large proportion of unsafe abortion occurs among adolescents who have not yet had children. As a result of trying to terminate unwanted or mistimed pregnancies, many forever sacrifice that experience and compromise their social standing and prospects in societies that very highly value motherhood and children. Children, especially young children, of women who are hurt or killed by unsafe abortion suffer as well. Studies show, for instance, that among infants whose mothers die, fewer than 10% will live beyond their first birthday.10 When women die from unsafe abortion, communities lose productive as well as beloved members, and health systems incur tremendous preventable expenses. Underlying Reasons Effectively addressing unsafe abortion requires understanding why it is so alarmingly prevalent on the African continent. If we look closely, the explanation is not surprising. This neglected public health crisis reflects numerous factors that contribute to other health problems in the region, and many that are unique to this sensitive topic. They include inadequate health care resources and infrastructure, restrictive laws and policies governing provision of abortion, and political and social stigma surrounding abortion, exacerbated by women's low social status and lack of empowerment. Lack of access to adequate health care underlies many health problems on the African continent. In the case of abortion, limited access to contraceptive information and services, as well as to broader information about reproductive physiology and reproductive health, contributes to the high incidence of unintended pregnancy, which obviously is a precursor of unsafe abortion. In Africa overall, only 13% of married women use modern contraception, according to the Population Reference Bureau11, and usage is much lower in several countries in the region. The many competing health priorities, most notably the HIV/AIDS pandemic, which confront African health systems certainly are one reason modern contraceptive methods are not more available in Africa. Somewhat ironically, another is their longstanding dependence on foreign donor governments and organisations for contraceptive programmes and supplies. Because few African governments allocate significant resources of their own to this crucial component of reproductive health care, family planning programmes lack the sustainability that is so important to ensuring long-term consistent use of effective methods, and the supply of such methods is subject to fluctuation, depending on the shifting policies and priorities of the donor nations. For example, after the US government reinstituted the Mexico City Policy, or Global Gag Rule in 2001, leading family planning providers in Kenya and Ethiopia took a principled stand and refused to accept its restrictions. The policy prohibits foreign non-governmental organisations (NGOs) that receive US family planning funds from being involved in any abortion-related activities including counselling, referral and even discussion of abortion as an option, even with their own money. As a result, these organisations lost not only significant portions of their funding but also contraceptive commodities that had previously been donated by the United States. According to a recent report on the impact of the Gag Rule, by 2002 it had resulted in an end of shipments of US-donated contraceptives to 16 countries and to leading family planning agencies in another 13.12 Policies that impose medically unnecessary conditions on who may obtain and use contraceptives and abortion also contribute to unintended pregnancy and unsafe abortion. Examples include: • Requiring women to obtain approval for abortion from a specialist gynaecologist, as in Zambia, although gynaecologists are usually not available in rural areas. • Requiring women to wait several days before being permitted to undergo an abortion. • Requiring a married woman to obtain the consent of her spouse or requiring a minor girl to notify or obtain the consent of a parent prior to an abortion. • Restricting advertising about contraception or abortion services, preventing women from obtaining much needed information about the availability of this care. Unmarried adolescents are particularly likely to be refused contraceptive methods either by dint of health system or facility policy, or simply because health workers who serve as gatekeepers disapprove of sexual activity by young people. In addition, failure to integrate family planning counselling and service delivery with post-abortion care creates a missed opportunity to help women who are obviously vulnerable to unwanted pregnancy avoid repeating the experience. Experience shows that providing contraceptive counselling to women following abortion care is very effective in increasing contraceptive use rates and, more importantly, reducing repeat unwanted pregnancies. Health care professionals have a responsibility to extend contraceptive services and counselling to all people including unmarried adolescents. Making emergency contraception widely available is especially important and is becoming a challenge in some countries, where anti-abortion activists incorrectlyclaim it is a form of abortion. But while it is critically important to expand the availability and accessibility of effective contraception in Africa, we must also remember that even with universal access to modern contraception, unintended and unwanted pregnancies will still occur as a result of contraceptive failure, rape and incest. Women's lack of autonomy in matters related to sex also contributes to unwanted pregnancy, given many women's inability to make their own decisions about using contraceptives and the prevalence of sexual coercion and violence. Girls as young as 9-11 years old have been known to become pregnant through rape. Accordingly, health systems also need to be prepared to meet women's need for life-saving post-abortion care for com-plications of unsafe abortion and for safe pregnancy termination, for legally approved circumstances. Notably, every African country legally permits abortion in at least some circumstances, but continent-wide even where legally permitted, safe abortion is scarcely available or accessible to women. Ensuring that post-abortion care and legal abortion, to the full extent of the law, are accessible requires training and equipping a range of health care providers to perform up-to-date uterine evacuation methods. Shortages of trained, equipped providers at every level of the health system lead many women to unskilled personnel who often practice in substandard conditions or, in determined desperation, to take matters into their own hands by trying a variety of methods to self-induce abortion. The root causes of such shortages include medical education institutions' failure to provide health care professionals with adequate opportunities to be trained in uterine evacuation and other relevant skills, as well as policies and laws that restrict who can perform uterine evacuation. Either by law or custom, many health systems permit only doctors to perform this simple procedure despite a growing body of evidence that with proper training and supervision, nurses, midwives and other health workers can provide safe and effective abortion care.3,13,14 In addition, many African health systems continue to rely on the outdated technique of dilation and curettage (D & C) or sharp curettage as the principal method for uterine evacuation. This practice is inconsistent with international clinical norms including those recently articulated by the World Health Organization, which specify vacuum aspiration and medical or pharmaceutical abortion as the preferred methods of early abortion.3 Manual vacuum aspiration (MVA) is especially suitable for use in low-resource and rural settings, and its use has the potential to save African health systems significant amounts of money.15 Application of this technique has been hindered in part by USAID's refusal to support purchase or distribution of MVA instruments, a policy that African health leaders should oppose and which the US government should reconsider in the interest of saving women's lives. Laws that place undue restrictions on who can obtain abortions are another significant factor in abortion-related mortality and morbidity. Although every African country legally permits abortion in at least some circumstances, these circumstances are typically limited to threats to the woman's life and, in some countries, cases of rape and incest. Africa's generally restrictive abortion laws are inherited from colonial powers that have long since liberalised their own laws. Prof. Fred Sai perceptively noted many years ago: The laws against abortion are mainly old laws, and it is worth recalling that part of the rationale for most 19th century abortion laws was to save women from quacks and unsafe and experimental surgery. That these same laws or their derivatives should now lead to the very opposite situation, given the safety and efficacy of currently available technologies, is a cruel irony. Liberalising restrictive abortion laws has been shown to result in dramatic decreases in maternal mortality when safe services are made available. In Romania, for example, after abortion was legalised in 1990, maternal mortality fell dramatically and immediately, almost completely due to significant reductions in the number of unsafe abortions (Figure 1). Although important implementation challenges remain, South Africa's post-apartheid liberalisation of its abortion law has already led to the increased availability of safe abortion services and a decrease in abortion mortality.16 It is time for African leaders to recognise that legal restrictions on abortion do not prevent abortions from occurring; they only ensure that those procedures will be unsafe. In addition to health system constraints and restrictive laws, a third important contributor to deaths and injuries from unsafe abortion in Africa is the pervasive social stigma that surrounds the topic. Not only abortion but sexuality itself remains largely a taboo in African societies. Furthermore, by and large, African women still lack autonomy and cannot make their own decisions about how to manage their fertility or about other fundamental issues in their lives. Lack of empowerment characterises women in many, if not most, sectors of African society, which helps explain why unwanted pregnancy is not just a problem of adolescents or poor women or other marginalised groups. Rather, all women, young, old, married, single, poor or rich are susceptible to unwanted pregnancy and unsafe abortion. The US-based Alan Guttmacher Institute estimates that on average every woman in the world will have at least one abortion during her reproductive years.17 Studies from a number of African countries between 1985 and 1996 show that women terminate pregnancies for a number of important reasons. While most African countries permit abortion only to save the woman's life or protect her health, studies show that these reasons are insufficient to meet women's needs. Women choose abortion most frequently because:17,18 • They are too young or want to postpone childbearing • They want no more children • They cannot afford to raise a child • They are unmarried or still in school • Their partner does not want the pregnancy or there is a problem with the relationship • They become pregnant due to rape or incest In most cases, abortion, safe or unsafe, offers the only option. Whether a woman lives in a place where safe abortion is available and accessible has the strongest influence on the quality and outcome of that experience. While all women are at risk of unwanted pregnancy, and most abortions occurring in developing countries are among women who are in married or other stable relationships17, certain populations are more vulnerable to unsafe abortion. As noted above, as a group, adolescents have least access to comprehensive reproductive health information and services so that sexually active young people are often thwarted in their efforts to act responsibly. Other marginalised women, for example, refugees and recent immigrants, suffer similarly. And in Africa as in every other country, poor women are much less likely than those with wealth and social connections to find a solution to unwanted pregnancy that does not put their lives at risk. Typically, women with resources can safely terminate unwanted pregnancies either by paying fees charged by private but clandestine providers or by travelling to a place with more liberal laws and more accessible services. Priority Actions to End Unsafe Abortion What can we do to end this unacceptable situation of so many African women and girls dying from the entirely preventable cause of unsafe abortion? What makes unsafe abortion unique among causes of maternal mortality and, in truth, among a wide range of health crises currently facing the world is that we know exactly how to address it. Solutions to the problem of unsafe abortion are well-known, practical and affordable even for resource-poor African nations. What is needed is the political and personal will to apply them. A number of effective approaches to the problem of unsafe abortion lie within the purview of health systems. Again, when performed in hygienic conditions by properly trained medical professionals, abortion is one of the safest of all medical procedures. To bridge the gap between that fact and the reality of tens of thousands of African women losing their lives to unsafe abortion, we need first to see abortion care as part of a continuum of reproductive health needs. We cannot end unsafe abortion without first expanding the availability and accessibility and improving quality of family planning, post-abortion care, safe abortion care, and related sexual and reproductive health care services. Expanding these services to the primary level, where most women live, is a key objective. Physicians in most developing countries are scarce. For example, in Gambia and Tanzania, there are only four physicians for every 100,000 people.19 This means nurses, midwives and other categories of health care providers must be involved in providing abortion services, and not just physicians. Logistics networks must be improved throughout health systems to make sure that the supply of abortion-related equipment is uninterrupted and sustainable. The quality of these services must be improved along with their accessibility. For post-abortion and induced abortion care, African health systems need to comply with World Health Organization recommendations and move away from the outdated D & C technology and instead make an effort to offer women a choice of safe abortion options including vacuum aspiration and medical abortion. African health and legal systems also need to do more to ensure that women have access to safe abortion services to the full extent permitted by law and to link abortion care with other aspects of sexual and reproductive health. Brazil offers an instructive example of what can be done along these lines. There, protocols and procedures are now in place that help women who have experienced sexual violence to obtain appropriate health care including legal abortion, bringing health, judicial and social services resources together in service of women's needs.20 As experience from other countries clearly shows, liberalising abortion laws can have an important impact on increasing women's access to safe pregnancy termination services. Decriminalising the procedure, as recommended in paragraph 106(k) of the Beijing Platform for Action from the Fourth World Congress on Women - that is, removing abortion from penal codes and regulating it through health codes and guidelines, as is common for all other health proce-dures - may also help reduce deaths and injuries of women from unsafe abortion. A review of international developments in abortion law between 1988 and 1998 reveals that countries are moving away from using criminal law to punish certain behaviours and instead extending the legal indications for abortion to preserve women's health and welfare, sometimes using a human rights rationale for the changes.21 Moreover, there is much that can be done even without altering the existing legal approach to abortion in African countries. Many health care providers, judges and lawyers are not familiar with their own countries' abortion laws; we must make sure all relevant professionals and all women know the circumstances in which abortion is permitted by law. Better knowledge and implementation of existing laws would go a long way toward reversing the tragic toll of unsafe abortion. Better publicising the conditions under which abortion is currently permitted and making abortion available to the full extent of existing laws can have numerous benefits, including: • permitting services to be visible, accessible and affordable for all women • helping health professionals feel protected in providing compassionate abortion services • allowing women to choose among providers • better enabling women to take legal action when their rights are violated Because the communities in which women live so strongly influence perceptions and experiences of abortion, action at the community level is also critical. To prevent unsafe abortion, we must work within communities to address the problems of unprotected sex and unwanted pregnancy. Steps needed include helping women and girls understand how they get pregnant and giving them the information, skills and ability to manage their fertility in a way that works for their lives. This requires putting more emphasis on educational efforts, advocacy and raising community awareness of the importance of allowing women to make these choices for themselves. Community education about the dangers of unsafe abortion is also important. Broad actions need to be taken to empower women in every aspect of their lives but especially in control of their reproductive lives. Women must be able to make their own fertility decisions and have access to and know where to find safe abortion services in their communities. Men must get involved and learn to support the women in their lives in reproductive health and choice issues. Lawyers and doctors must understand what the abortion law says and when they have an obligation to provide safe services, and their professional associations ought to take an active role in ensuring that they have this information. Health care professionals also have a responsibility to serve as advocates in this area. Their participation in community awareness building about the availability of contraceptives and the indications for which abortion is legally allowed is essential. Conclusion Preventing abortion mortality and morbidity in countries where they remain high is a matter of good public health policy, is based on good medical practice and is an important part of initiatives to make pregnancy safer. It is also essential to efforts to pro-mote development and to safeguard women's human rights. For these and other reasons, we need to build a future where women can make independent and safe reproductive choices so that they have the opportunity to improve their future and the future of their families. Actions such as those suggested above require increased commitment, action and resources by key stakeholders at all levels: government, parliamentarians, the legal system, health care professionals and community leaders. But African health care profes-sionals and policymakers are the principal witnesses to the tragic failure to provide for women in this fundamental area of their lives. We challenge them in particular to find their role in this effort and to be silent no longer. References
© Women's Health and Action Research Centre 2004 The following images related to this document are available:Photo images[rh04006f1.jpg] |
| |||||||||

{kind=link}