 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
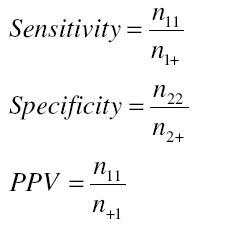
African Journal of Reproductive Health, Vol. 12, No. 3, Dec, 2008, pp. 35- 48 Original Research Article Determinants of Post-Partum Maternal Mortality at Queen Elizabeth Central Hospital, Blantyre, Malawi: A Case-Control Study 2001-2002 Kanyighe, C.1, Channon, A.2,3 , Tadesse, E. 1, Madise, N.2,3 , Changole, J. 1 Bakuwa, E. 1, Malunga, E1 and Stones, R.W.2,4 1Queen Elizabeth Central Hospital, Blantyre, Malawi. Code Number: rh08036 ABSTRACT The aim of this research is to identify the clinical, demographic and service-based determinants of postpartum maternal mortality within Queen Elizabeth Central Hospital, Blantyre, Malawi, during 2001 and 2002. The study uses a case-control design using all postpartum maternal deaths in 2001 and 2002 as cases, with analysis conducted using conditional logistic regression. The results indicate that the mothers’ reason for admission into hospital and the outcome of the birth were significantly related to maternal death when analysing all potential explanatory variables in one model. A group of high-risk mothers can be identified using these factors. If these criteria were applied as a predictive tool in the clinical setting the resulting sensitivity and specificity would be over 85%. Identification within the hospital setting of a group of very high-risk mothers in whom serious complications are aggressively managed in a coordinated way across the medical specialties may reduce maternal mortality. RĖSUMĖ Les déterminants de mortalité maternelle post-partum à Queen Elizabeth Hospital, Blantyre, Malawi : Etude de contrôle de cas 2001 – 2002 Cette recherche a pour but d'identifier les déterminants cliniques, démographiques et à base de service de mortalité maternelle postpartum à Elisabeth Central Hospital, Blantyre, Malawi, pendant 2001 et 2002. L'étude utilise une conception de contrôle de cas utilisant toutes les morts maternelles postpartum en 2001 et 2002 comme des cas, avec l'analyse conduite utilisant la régression logistique conditionnelle. Les résultats indiquent que la raison pour laquelle la mère est admise dans l'hôpital et le résultat de la naissance ont été significativement rapprochés de la mort maternelle en analysant toutes les variables potentielles explicatives dans un modèle. Un groupe de mères à haut risque peut être identifié utilisant ces facteurs. Si ces critères ont été appliqués comme un outil prophétique dans l'arrangement clinique, la sensibilité résultante et la spécificité seraient plus de 85 %. L'identification dans le cadre d'hôpital d'un groupe de mères à haut risque dont des complications sérieuses sont agressivement gérées d'une façon coordonnée à travers les souvenirs médicaux peut réduire la mortalité maternelle. KEY WORDS: Postpartum Maternal Mortality; Case-control; High-risk Groups; Malawi Introduction In 1996, the Malawi Safe Motherhood Programme (SMP) was established with the aim of reducing the national maternal mortality rate (MMR) and neonatal mortality rate (NMR) by 50% by the year 2000. Yet, despite the elaborate strategies and activities designed to meet this aim, the situation appears to have worsened. In 1992 the Malawi Demographic and Health Survey (MDHS) reported a MMR of 620 per 100,000 live births1 . However, by the year 2000 the MDHS reported a MMR of 1120 per 100,000 live births2 indicating an 80% increase in only 8 years. The 2005 MMR estimate for Malawi was 1,100 (95% CI: 720, 1500), showing that there has been little progress3. Within the Queen Elizabeth Central Hospital (QECH) in Blantyre, the hospital used within this study, the MMR was 476.9 per 100,000 live births in 19924 but had risen to 1027 deaths per 100,000 live births by 20005. That the figures from QECH mirror the national trend is unsurprising as QECH is the major referral hospital in the southern area of Malawi. Causes of maternal death are often multifactor and involve complex interactions between medical, obstetrical and social factors. Studies conducted in various areas of Malawi between 1987 and 1994 showed that, in order of importance, the main immediate causes of maternal deaths were obstetric haemorrhage, puerperal sepsis, obstructed labour/ruptured uterus, complications during and after abortion and eclampsia6 . The increase in the overall mortality rate of women aged 15 to 49 between 1992 and 2000, from 6.5 to 11.3 per 1000, is also presumed to be due to HIV/AIDS7 . Pregnancy related mortality due to HIV/AIDS can be caused directly through an increase in puerperal sepsis, or indirectly through anaemia, tuberculosis and meningitis. These indirect causes of death may be aggravated by pregnancy8 . Safe motherhood programmes may be adversely affected by HIV because HIV-related illnesses increase crowding in health facilities and affect the quality of maternity services. In a survey at QECH, HIV/AIDS was directly responsible for 18.6% of all maternal deaths, and indirectly involved in 58.0% of deaths9 . Conversely however, in a study conducted in the Congo, HIV/AIDS was seen to confer a positive effect on survival chances during pregnancy. It is thought that this is because extremely sick women are unable to conceive, and therefore only the healthier HIV positive women are able to get pregnant, leading to the observed beneficial effect when compared to women who are HIV negative10 . Within QECH, the quality of health care services deteriorated greatly over the five years prior to the study. Staffing levels diminished to as much as one third of the stated targets in some departments. This, coupled with the worsening economic environment which affected procurement of essential drugs, equipment, commodities and supplies, servicing and maintenance of equipment as well as staff deployment and retention adversely affected care levels within the facility.While in safe motherhood programming as a whole the risk based approach in antenatal care has been abandoned as lacking predictive value, in extremely resource constrained settings there is potential benefit in being able to identify the groups of mothers who are at most risk of dying before, during and after childbirth. This study aims to partly address this need by studying the factors that are associated with post-partum maternal mortality within QECH. As a result of this study the highest risk mothers will be able to be identified and can therefore be targeted effectively when they are admitted to the hospital. Methodology The study is a retrospective casecontrol study conducted at the main national teaching and referral hospital in Malawi, QECH in Blantyre, from 2001 to 2002. Maternity capacity is 250 beds, and the hospital handles approximately 30-40 deliveries per day, both self-referred and referred from other health facilities, including districts in surrounding Blantyre. Due to the relatively rare nature of maternal death, a case-control study was selected as the research design. This method allows the analysis of all maternal death cases, as opposed to alternative study designs where some cases will not be available for analysis. Cases Every pregnancy-related death which occurred in the maternity department was recorded and thoroughly discussed at a departmental mortality audit held fortnightly. Information regarding the pregnancy, abortion, labour and delivery and any noticeable health problems the patient might have had, treatment or intervention and events leading to maternal death were discussed. The maternal death questionnaires used to obtain the information for this study were completed by the study committee after each meeting. Controls Controls for the study were selected from postpartum mothers who delivered at QECH during January 2001 to December 2002. Cases and controls were matched only by age group i.e. 15-19, 2024 etc. Four controls for each maternal death were selected within the same week/month that the death occurred, two from before and two from after the death. The mothers who were selected as controls were those in the same age group who had given birth closest in time to the mother who died. The study committee was involved in scrutinizing the controls’ files and questionnaires for the selected mothers were completed and checked. The same format of the questionnaire was used for both cases and controls to obtain consistency. No socioeconomic information was routinely collected from either cases or controls and thus a comparison of characteristics between the two groups in order to assess similarity was not possible. In a case-control study, both cases and controls need to be selected from the same population in order for accurate conclusions to be drawn from the analyses. As the controls were only selected from postpartum women it was required that maternal deaths which occurred before and during labour were excluded from the analysis of the determinants of maternal death. This excluded all women who died due to abortion, ectopic pregnancy and any other antenatal mothers from the casecontrol portion of this study, amounting to about 50.2% of the maternal deaths in the hospital during the period of the study. Statistical Methods An initial investigation of the maternal deaths in QECH between 2001 and 2002 was conducted using all recorded maternal deaths. Frequencies and percentages of maternal deaths during the period of study within derived categories of mother’s age, parity and the reason for admission to the hospital were calculated. For the case-control study, four different models were formed to investigate distinct areas of interest. Table 1 displays the potential explanatory variables used in the formation of the different models. These models relate to (a) medical, (b) service and (c) demographic factors. The number of days that the patient stayed in hospital was classified as both a medical/clinical factor and a service-based factor, and was tested for inclusion in both models. The fourth model that was constructed used all potential variables. For all four models multivariate modeling on the matched data set was conducted using conditional logistic regression. Logistic regression was seen to be appropriate as the outcome variable, maternal death, is a binary outcome. Conditional logistic regression was used as opposed to unconditional logistic regression due to the small number of cases analysed. Also, using unconditional logistic regression for a matched case control study leads to biased estimates11 . Forward selection was used to generate each of the models. Once the final model in each category had been chosen, odds ratios were calculated. The reference category was selected to be the group who were least at risk of dying, except where there was a clear alternative category to use. Confidence intervals for these odds ratios were calculated. This analysis was conducted using the STATA software package version 8.0 (StataCorp, College Station, TX). Finally, to assess if the factors that are seen to be significantly related to maternal death are able to identify highrisk mothers the sensitivity, specificity and positive predictive value (PPV) of using each factor separately to predict maternal death was calculated. Sensitivity is defined as the percentage of maternal deaths that would be correctly identified if a specific factor was used to predict death, while specificity is the percentage of those who survived who did not have a specific factor. Finally, the PPV is the percentage of women who died if they suffered from the different factors listed. A full explanation of the calculation of these terms is shown in the appendix. Table 1: Potential explanatory variables for the medical/clinical, service based and demographic models studying the causes of maternal death in QECH
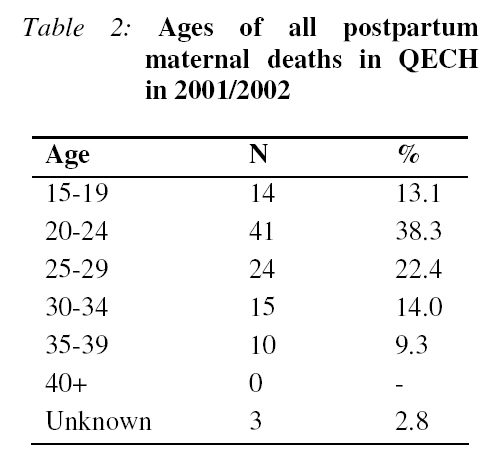
Results In the two years of the study, the hospital recorded 209 maternal deaths. In 2001 there were 98 deaths giving an institutional MMR of 1116.68 per 100,000 live births, whilst in 2002 there were 111 deaths giving an institutional MMR of 1112.3 per 100,000 live births. Of these maternal deaths, 55 were due to abortion and 39 were antenatal mothers, 8 mothers died in labour and 107 died in the postpartum period. The age distribution of those who died in the postpartum period is shown in Table 2. Medical/Clinical Factors Associated with Maternal Death For the 107 postpartum mothers who died, the clinical factors leading to their deaths were identified. These factors were then grouped into obstetrical, medical, anaemia and HIV/AIDS related categories. Many cases were seen to have multiple causes of death, and so were placed in more than one category. Direct obstetrical problems accounted for the largest proportion of deaths (76.6%), whilst HIV/AIDS was involved in 29.0% of maternal postpartum deaths. The diagnosis of HIV/AIDS was made after a clinical assessment, as HIV testing was not available at the time of the study. The two other causes of death identified are medical problems, related to 53.3% of deaths, and anaemia, related to 40.2% of deaths. The conditional logistic model relating to medical and clinical factors showed that the condition of the patient on admission, the reason for admission, the outcome of the birth and the number of days spent in hospital were all significantly related to maternal death. Condition on admission was categorized into:
Table 3 shows that if a woman was admitted in a critical condition they were 17 times more likely to die (95% Confidence Interval 3.05-93.09) than if they were admitted in a stable condition. Regarding the reason for admission, patients who had a postpartum infection had odds of dying which were 100 times higher (95% CI 5.06-1964.83) than those who were admitted due to a labour related problem. If the outcome of the pregnancy was a stillbirth or a neonatal death the odds of dying were higher than if the outcome was a live birth. Women who had a stillbirth were 18 times more likely to die (95% CI 3.71-83.42) whilst women who had a neonate who died early in its life were 88 times more likely to die (95% CI 2.62-2955.19) than those with a live birth. Finally, women who had complications and stayed in the hospital for more than 7 days had significantly raised odds of dying when compared to those who stayed in the hospital for up to 4 days. Odds were raised by a factor of 5 for those who stayed for over a week compared to those who only stayed for up to 3 days (95% CI 1.50-18.12). Service Factors From the long list of service factors tested, only APGAR score, availability of equipment (e.g. blood, drugs), use of caesarean section, a postpartum blood transfusion and evacuation were significantly related to maternal death (see Table 4).If a woman delivered a stillbirth (APGAR score 0) her odds of dying were 55 times higher (95% CI 9.09-333.23) than if the woman had delivered a child with a normal APGAR score of 6 to 10. There was no significant difference in odds of dying between Table 3: Results of conditional logistic regression studying maternal mortality in QECH using medical/clinical factors
*NS = Not significant at 95% level mothers of children with low APGAR scores (score 1 to 5) and of those with children with normal APGAR scores. It was not possible to identify from the questionnaire results whether certain procedures such as caesarean section or blood transfusions were required, only if they were conducted. However, if some equipment was needed to be used but was not available e.g. blood, then a woman in this situation had odds of dying which were 75 times higher (95% CI 6.98803.76) than women who received all the equipment needed. Mothers obtaining a caesarean section were 7 times more likely (95% CI 2.08-26.07) to die than women who did not have this operation, and if a woman received a blood transfusion the odds of dying were raised by 38.37 (95% CI 2.44-603.33). Finally, if a woman was not evacuated after birth then the odds of dying were raised by a factor of 16 when compared to a woman who was evacuated (95% CI 1.49167.53). Demographic Factors After an initial analysis of the demographic factors displayed in Table 1 marital status and educational background were not used in the multivariate analyses due to the amount Table 4: Results of conditional logistic regression studying maternal mortality in QECH using service-based factors
*NS = Not Significant at 95% level of missing data on these variables. Out of the four remaining demographic variables, only birth weight and parity of the mother were significantly related to maternal death in the final logistic regression model (see Table 5). Women who had delivered very low birth weight babies (under 1.5kg) had odds of dying which were 83 times higher (95% CI 10.24-676.20) than women who had normal birth weight children (over 2.5kg). Mothers of low birth weight children (between 1.5kg and 2.5kg) had odds of maternal death which were 3.5 times higher (95% CI 1.86-6.63) than mothers of children whose weight was in the normal range. With respect to the parity of the mother, nulliparous mothers have raised odds of dying when compared to mothers of low parity (1-3 previous births). These raised odds are by a factor of 3.3 (95% CI 1.46-7.66). Overall Analysis Condition on admission to the hospital was seen to explain a large proportion of the overall variation in mortality risks, and the combined model would be extremely similar to the medical/clinical model. On exclusion, the combined model displayed other significant Table 5: Results of conditional logistic regression studying maternal mortality in QECH using demographic factors
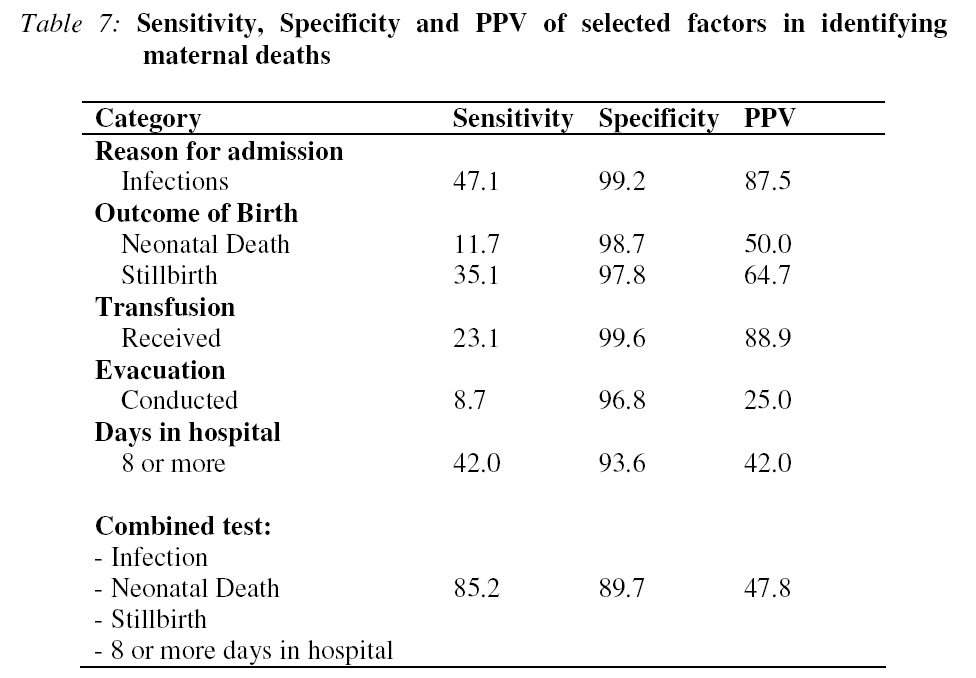
*NS = Not Significant at 95% level relationships, and the reason for admission, outcome of the birth, whether a postpartum transfusion was conducted, if there was the requisite availability of equipment and the number of days the mother stayed in hospital were related to maternal death (Table 6). The odds ratios in this final model were higher in all the significant categories when compared to the individual factor models. The relationships described in previous sections are therefore still valid for the overall model, although the odds ratios and the confidence intervals have changed. Identification of High-Risk Mothers The conditional logistic regression model shown in Table 6 indicates the main causes associated with maternal death. To assess if these factors can successfully identify and highlight highrisk mothers on admission to the maternity ward the sensitivity, specificity and PPV of using each factor separately to predict maternal death was calculated (Table 7). Taken individually, it is seen that each factor is not good at identifying mothers at risk of dying, as many mothers who die are not being identified as high-risk. A better test is using three of the variables together in one test to predict maternal mortality. In this instance, mothers who were admitted into Queen Elizabeth with an infection, had a stillbirth or a neonatal death, or stayed in the hospital for longer than a week were identified. Out of 88 mothers who died with complete data on these variables, 75 of them would have been identified using these criteria, and only 13 mothers would not have been pinpointed, giving a sensitivity of 85.2%. If the controls are analysed in the same way, only 82 mothers would have been identified as being highly at risk of death, giving a specificity of 89.7%. The PPV indicates that almost a half (47.8%) of mothers with these characteristics died. Therefore, placing those mothers who were admitted due to an infection, who had a stillbirth or neonatal death or who stayed in the hospital for over a week into a service Table 6: Results of conditional logistic regression studying maternal mortality in QECH using all potential factors except condition on arrival
*NS = Not Significant at 95% level environment such as a high-dependency ward with ready access to care from both obstetricians and physicians would have concentrated most of those mothers who subsequently died into a care environment more likely to have averted their deaths. Discussion This study set out to identify the Motherhood Initiative, the MMR within the hospital is still very high. Even though it was impossible to compare all the potential factors due to the large amount of missing data within the dataset, the contribution of a range of clinical, service related and demographic factors has been investigated. These factors come together and result in major complications and death. The scale of the missing data is not surprising because there is evidence from both developed and developing countries that care providers frequently fail to elicit important information about women’s obstetric and medical history and sometimes even fail to take appropriate action when evidence of high-risk is obtained 12 . The clinical condition of the patient at the moment of admission is critical in determining fetal outcome. It appears that good fetal outcome is closely related to good maternal outcome, although conversely it can be thought that a critically ill patient is more likely to have a bad fetal outcome. McDermott et al, in a study conducted in rural Malawi, showed that mortality among infants of mothers who died was 37 times higher than the rate of death among infants born to mothers who survived13 . The birth weight of babies is another important determinant of maternal mortality. Mothers of children who had a very low birth weight (under 1.5kg) were more likely to die than mothers of low birth weight children (1.5kg to 2.5kg). Both of these groups had raised odds when compared to mothers of normal weight babies. Causality in this instance is unknown but maternal conditions such as severe pre-eclampsia are associated with intrauterine growth restriction while also causing serious maternal morbidity. In this study, mothers of high parity were not significantly more likely to die. This defies the belief that high parity is associated with a high incidence of maternal mortality and morbidity. The result may be due to the fact that women of high parities are a minority among the obstetric population in this hospital. However, the result indicates that further investigations are needed to assess the changes to the risk for lower parity women when compared to those of higher parity. Availability of drugs, equipment, blood and blood products also play a major role on maternal death. This study has shown that a lack of equipment raises the odds of dying, and having a blood transfusion also greatly raises the odds of mortality. The relationship between maternal death and blood transfusions is presumed to be due to severe anaemia, which about 40% of women in the study were classified as having. Therefore this result may be due to the women who had a transfusion not getting the required amount of blood needed and not the transfusion itself. This is usually due to scarcity of blood and blood products, which is a common problem in QECH. Operative delivery also poses a high risk of maternal mortality. In this study women who had a caesarean section were seven times more likely to die than those who did not have the operation. Studies conducted in Malawi by Fenton et al. showed that women undergoing caesarean section can suffer from preoperative haemorrhage, shock, anaemia and ruptured uterus. Hence it was noted that these major preoperative complications are associated with a high maternal and perinatal mortality14 . In a hospital setting it is most important for clinicians to maintain a review process for indications and outcomes of surgery, so as to be sure that the association highlighted above is indeed due to the underlying condition necessitating caesarean section, and not to the procedure itself. The identification of high-risk mothers is a possible strategy to follow in order to reduce the level of maternal mortality. Although generalisation of these results is not possible due to the non-random selection of controls, our findings indicate that the use of a set of identification criteria, i.e. an infection on arrival, a stillbirth or neonatal death, or those staying in hospital for over a week, would aid identification of a very highrisk sub-group. The majority of mothers who died would have been 'flagged' using these criteria, without imposing an excessive burden on the service by identifying large numbers of women. These women could be provided with additional medical and nursing input at an early stage, perhaps via a high dependency ward, and monitored intensively. The configuration of services in many hospitals tends to present a barrier to the rapid involvement of infectious disease physicians in the care of severely ill obstetric patients and specific measures to overcome such barriers are required. The strategy are required. The strategy outlined above needs to be tested in future research. The study had a number of limitations. Firstly, the need to exclude all non-postpartum deaths due to the controls only being taken from postpartum mothers is an obvious drawback. About half of the maternal deaths were therefore not analysed, which reduced the statistical power of the study, resulting in large confidence intervals for the odds ratios. A second drawback was the amount of missing data in the dataset. A number of variables, such as marital status and educational level, could not be analysed due to the amount missing values. Cases and their associated controls were dropped from the analysis if there was missing data on any of their variables included in the model, again reducing statistical power. Another drawback was that HIV testing was not undertaken at the time of the study so diagnosis of HIV/AIDS related morbidity was on clinical grounds. Finally, some of the potential explanatory variables may not be direct causes of mortality. Some medical procedures may be used to try and save the mother’s life, such as a blood transfusion. The association between these procedures and maternal mortality may therefore not be due to the actual procedures themselves. A further consideration is that the data are from 2001 and 2002. This fact is mitigated by anecdotal evidence that little has changed in the conditions within the hospital in the intervening period. Therefore the results are considered to still be applicable. The new programme, Road Map, to tackle maternal mortality in Malawi which started in 2007 may have an accelerated impact in reducing maternal deaths. However, such impact would not be felt after just a few months of the launch. Furthermore, the specific approach of focusing obstetric, medical and nursing energy for the benefit of critically ill patients has not been part of the strategic approach to maternal mortality reduction thus far. Acknowledgements The research was funded by the UK Department for International Development via the ‘Opportunities and Choices’ Programme based at the University of Southampton. The views expressed are those of the authors. Appendix Calculation of sensitivity, specificity and positive predictive value (PPV) The following table explains how the sensitivity, specificity and PPV are calculated. The specific factors tested are those that were significant in the final logistic regression model.
References
© Copyright 2009 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh08036t2.jpg] [rh08036t7.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}