 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 5, No. 4, Autumn, 2007, pp. 183-186 Association of inherited thrombophilia and antiphospholipid syndrome with severe preeclampsia Maryam-sadat Hosseini M.D., Parviz Gharehkhani M.D., Maryam Sadeghi M.D. Department
of Gynecology and Obstetrics, Shaheed Beheshti University of Medical Sciences, Tehran, Iran. Received: 10 June 2007; accepted: 27 December 2007 Code Number: rm07035 Abstract Background: Severe preeclampsia is a quite well-known entity
with high incidence of both maternal and fetal morbidity and mortality.
Although little is known about its etiology, inherited disorders of hemostasis
and antiphospholipid syndrome have been postulated as common causes. The
present study was conducted to evaluate the association of these two entities
with preeclampsia in a group of Iranian patients. Key words: Severe preeclampsia, Factor V leiden, Protein C, Protein S, Antithrombin III, Lupus anticoagulant antibody, Anticardiolipin IgG and IgM. Introduction Despite many advances achieved in obstetrics and gynecology during the recent decades, severe preeclampsia remains one the most common concerns that complicates approximately 5% of all pregnancies. It is often distressing for the patient and frustrating for the physician (1). Although its etiology has been a matter of continuing debate, vascular endothelial inflammation and dysfunction have been proposed as the main etiologic factors (1). Unfortunately, severe preeclampsia is not a preventable illness and delivery is the only definitive treatment (1-3). Severe preeclampsia is frequently associated with preterm delivery and its subsequent complications; however, it could cause seizure, blindness, renal ischemia, hepatic rupture, or even death in mother (1-3). Therefore, determining the etiologic factors of severe preeclampsia is one of the most important priorities of gynecologists. Inherited disorders of hemostasis and antiphospholipid syndrome have been postulated by prior investigators as common causes (4-6), however, controversies have aroused about their actual mechanisms. Some have demonstrated a significant association between severe preeclampsia and antiphospholipid syndrome (7,8), while others failed to show any association (9,10). The present study was designed to evaluate the association between severe preeclampsia and inherited disorders of hemostasis and antiphospholipid syndrome in a group of Iranian patients referring to a referral center for Gynecology and Obstetrics in Tehran. Materials and methods For this case-control study from April 2002 to March 2003, 26 females with severe preeclampsia were matched with 26 healthy parturients as controls. Severe preeclampsia was defined as diastolic blood pressure ≥110mmHg, severe proteinuria (+2) as well as other signs and symptoms including headache, blurred vision, epigastric pain, oliguria, thrombocytopenia, elevated liver enzymes, intrauterine growth retardation, and pulmonary edema (1). Parturients referring to the same hospital (similar socioeconomic status) who did not meet the diagnostic criteria of severe preeclampsia were matched according to the age, gestational age, parity, and previous history of abortion with the cases. A similar questionnaire was completed for all subjects. Meanwhile, 10cc peripheral blood samples were obtained and indices of inherited disorders of hemostasis such as factor V Leiden, protein C, protein S, and antithrombin III (AT III) as well as antiphospholipid syndrome ie, lupus anticoagulant antibody, and anticardiolipin antibody (IgM and IgG) were determined. The normal range of the abovementioned indices were considered as follow: factor V Leiden: >120pg/l, anticardiolipin IgM<7pg/l and IgG<10pg/l, protein C: 70-130pg/l, protein S: 65-140pg/l, and AT III: 80-120pg/l. Lupus anticoagulant antibody was considered either positive or negative. All subjects were requested to fill an informed consent. T-test, Mann-Whitney U-test, chi square, and Fisher's exact test were used for data analysis, when appropriate. In case of significant association, odd's ratio of index with severe preeclampsia was calculated with 95% confidence interval. A p-value of less than 0.05 was considered to be statisticallysignificant. Results The study population included 26 cases with the mean (± standard deviation) age of 27.6±7.6 years, mean gestational age of 33.9±5.4 months, and mean parity of 1.8±1.3 as well as 26 controls with mean age, gestational age and parity of 24.5±4.7, 36.8±3.5 and 1.4±1.2, respectively. There was no significant difference (NS) between the two groups in any of the aforementioned variables.The mean value of factor V Leiden in the control group was 137.3±20.0pg/l as compared to 138.8±22.7pg/l in the severe preeclamptic patients (NS). Table 1 outlines the frequency of positive subjects in different indices of inherited disorders of hemostasis. As shown, factor V Leiden was found abnormally high just in one parturient with severe preeclampsia. Table I. Frequency of abnormal values in different indices of inherited disorders of hemostasis in case and control subjects
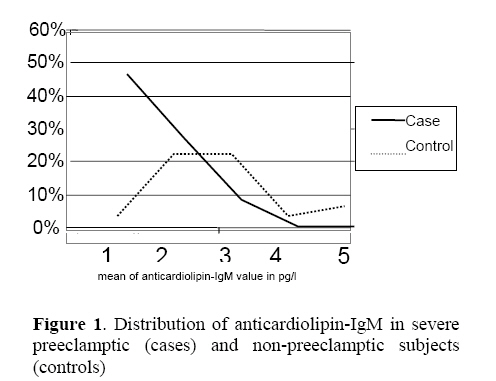
Fisher's exact test did not reveal a significant association between factor V Leiden and severe preeclampsia. The mean value of protein C and S were 107.6±32.6 and 60.6±14.5pg/l in preeclamptic patients, while these values were 118.8±26.1 and 58.0±17.1pg/l in controls, respectively, and t-test revealed insignificant differences between the two groups. Of 26 cases, 7(26.9%) and 14(53.9%) had abnormal values of protein C and S, respectively, however, the differences with the control subjects (34.6% and 65.4%) were not statistically significant (table 1). Similarly, the antithrombin III level did not differ between case and control subjects (97.4±16 vs. 99.0±11.7pg/l). The mean of anticardiolipin-IgM value was 4.48±2.69pg/l in severe preeclamptic parturients as compared to 3.27±2.0pg/l in controls (p<0.001). IgM>4pg/l was found in 2 (7.7%) non-preeclamptic (controls) and 7(27.9%) severe preeclamptic parturients that showed a statistical significant difference (p<0.05). Indeed, severe preeclamptic parturients were 4.4 times more likely to develop elevated levels of IgM (OR=4.4, 95%CI=1.9-10). The mean of anticardiolipin-IgG value was 6.04±9.6pg/l in cases and 4.88±2.8pg/l in controls (NS). Abnormally elevated IgG level was reported in one severe preeclamptic female (3.8%) as compared with 4 (15.4%) controls (NS). Finally, lupus anticoagulant antibody was similarly detected in one case and one control. Figure 1 represents the distribution of anticardiolipin-IgM in severe preeclamptic and non-preeclamptic subjects. As shown, controls are more likely to have low IgM levels. Discussion Results have revealed that indices of inherited disorders of hemostasis including factor V Leiden, antithrombin III, protein C, and protein S as well as anticardiolipin-IgG and lupus anticoagulant antibody were not associated with severe preeclampsia, however, anticardiolipin-IgM was found more frequently in severe preeclamptic subjects. Although anticardiolipin-IgM was reported within the normal range in both groups (<7pg/l), preeclamptic parturients were more frequently found to have IgM>4pg/l than non- preeclamptic subjects, thus, preeclamptic patients are more likely to develop elevated level of IgM. Decreased Antithrombin III, inherited as autosomal dominant traits, is associated with a 70-90% increased risk of thrombosis (11, 12), however, several studies failed to address its role in severe preeclampsia (13-15). Deficiency of protein C has been documented in approximately 0.2% of the general population and may be manifested as decreased antigenic factors or dysfunctional proteins. Deficiency of protein S has similar prevalence but could also produce symptoms because of decreased free protein level (16, 17). Dekker and colleagues (1995) have reported deficiencies of protein C and S in less than 1% and 25% of severe early-onset preeclamptic parturients, respectively (14), however, this association was not supported in other studies (13, 18). Similarly, there are some controversies around the role of factor V Leiden in preeclampsia. Dizon-Townson et al (1996) reported predisposition to severe preeclampsia in females with mutation in factor V Leiden, whereas others disagreed these findings (19, 20). Prior investigators have also demonstrated an increased risk of preeclampsia in the presence of antiphospholipid syndrome and anticardiolipin-IgM and -IgG antibodies (19, 21-23). They have reported an odd's ratio of 6.2 in their studies, whereas, more recent studies failed to show this association (24, 25). These controversies in different studies could be explained in part by different methodological approaches or the fact that preeclampsia is a multifactorial disorder. Nevertheless, sample size imparts an important role in interpretation of the results. Our study has some potential weaknesses. Like previous studies of the same design, there was a risk of a selection bias and recall bias as well. Our sample size was quite small; however, we may address matched controls, similar socioeconomic status and our study protocol as the strong points of this study. In conclusion, the present case control study reveals a modest association between anticardiolipin-IgM antibody and development of severe preeclampsia; however, routine screening tests for indices of inherited disorders of hemostasis are not recommended due to the high expenses and shortness of their association with preeclampsia. Finally, we believe cohort studies may shed further insight into the mechanisms of preeclampsia. References
© Copyright 2007 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm07035f1.jpg] |
| |||||||||

{kind=link}